Youth depression in Ethiopia: a comprehensive systematic review and meta-analysis
Samuel Derbie Habtegiorgis, Animut Takele Telayneh, Lake Kumlachew, Nigussie Walelgn, Dawit Alemayehu, Molla Azmeraw, Kalkidan Worku Mitiku

TL;DR
This study finds that 36% of Ethiopian youth suffer from depression, with social support, gender, and alcohol use being key factors.
Contribution
The study provides the first comprehensive meta-analysis of youth depression prevalence in Ethiopia.
Findings
The pooled prevalence of youth depression in Ethiopia is 36%.
Female gender, poor alcohol use, and lack of social support are significant predictors of depression.
The depression rate is higher than the WHO's global mental health report estimates.
Abstract
Mental health is the state of well-being that manages our emotions, psychological stress, social well-being and it is essential at all stages of life. Depression is a mental health condition that causes repeated changes in mood and in how a person feels about everyday life. It can impact every aspect of life, including relations with friends, family, and the community. Depression, like most other mental health conditions, begins at the time of childhood or adolescence and can continue into adulthood. Depression among young people is widespread in developing nations like Ethiopia. This review aimed to compile data on Ethiopia’s youth depression. We searched through papers on the topic within the electronic databases of Worldwide Science, Google Scholar, Cochrane Library, PubMed, and Web of Science. The data were extracted using a Microsoft Excel™ format and exported to R (software) for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
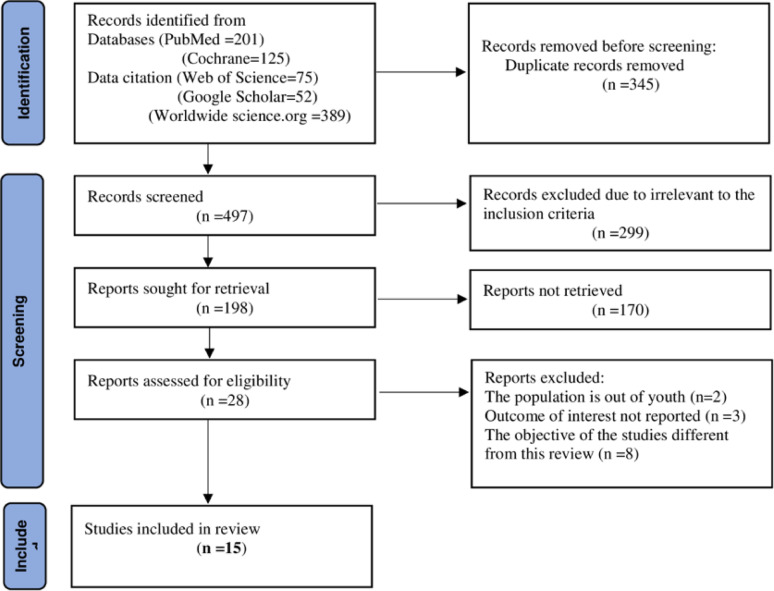 Figure 1
Figure 1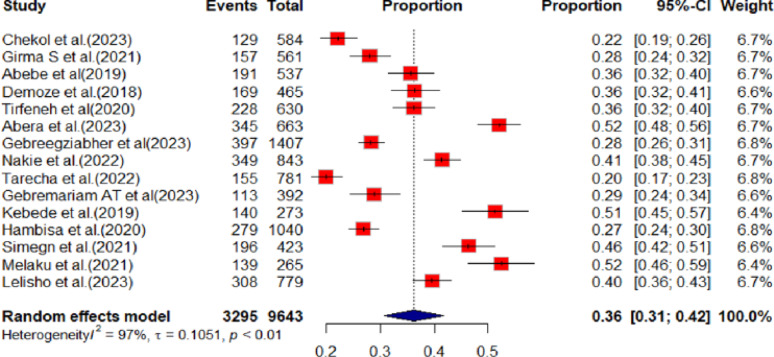 Figure 2
Figure 2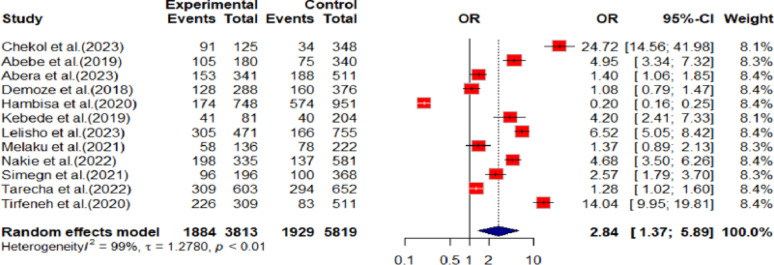 Figure 3
Figure 3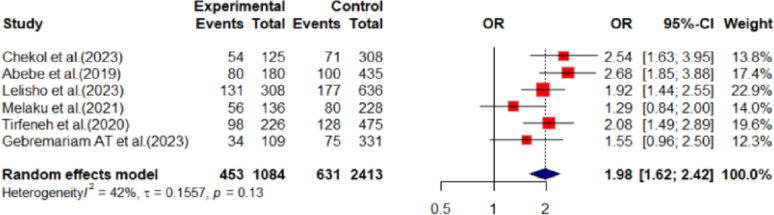 Figure 4
Figure 4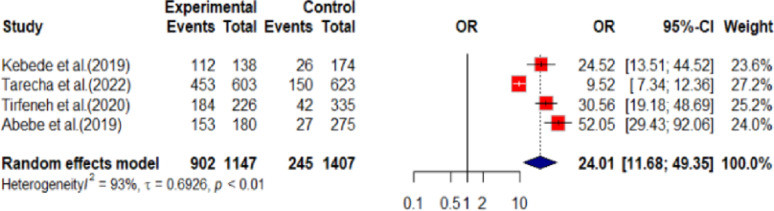 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild and Adolescent Psychosocial and Emotional Development · Mental Health Treatment and Access · COVID-19 and Mental Health
Introduction
Mental health is the state of well-being that manages our daily activities, including emotions, psychological stresses, social well-being or social interactions, and shapes our interactions, thinking, and how we view reality. Mental health is essential at all stages of life, from childhood, adolescence to maturity [1–3].
Depression is a mental health disorder that manifests itself with several repeated mood swings and feelings about day-to-day life. It affects nearly every part of life. It causes ongoing sadness, loss of interest, and difficulty thinking clearly. It can disturb sleep, appetite, and energy, while also leading to social withdrawal and strained relationships. At work or school, it reduces performance and increases absenteeism. If untreated, depression can contribute to chronic illness, economic hardship, and even suicide [6]. The onset of depression often occurs during childhood or adolescence. Depression is increasingly widespread in developing nations like Ethiopia [4, 5]. Like many diseases, depression is severe in some cases and mild in others. Depression can affect anyone, regardless of age, gender, location, income, social status, race, ethnicity, religion/spirituality, sexual orientation, background, or any other aspect of cultural identity. Although depression can develop at any age, three-quarters of cases begin before the age of 24.
[7].
Depression affects approximately one in every five people at any given time [8]. In recent years, studies have shown that the prevalence of depression among adolescents is increasing [9]. Globally, over 300 million people are estimated to suffer from depression which is equivalent to 4.4% of the world’s population. From this about 17.5% are youth age less than 25 years. One in eight adolescents has a risk of depression problems [2, 10] and the prevalence of depression varies across the globe, in China (12.4%) [11], in America (20%) [12], in sub-Saharan Africa countries (18.3%) [13]. Suicide thoughts and attempts related to mental illness or depression has increased [14, 15] and every year more than 700,000 people die due to suicide around the world. It is the fourth leading cause of death among 15–29-year-olds and 77% of global suicides occur in low- and middle-income countries [16]. Ethiopia is experiencing an ongoing increase in the prevalence of depression particularly among young people [17]. It may be aggravated by the ongoing COVID-19 pandemic, war, and regional and national conflicts [18, 19]. Studies conducted about depression in Ethiopia show the different magnitudes and factors. The magnitude is different in different studies. This review aimed to generate pooled magnitude and risk factors of youth depression in Ethiopia.
Methods
Searching approach of primary studies
We searched through papers on the topic within the electronic databases of Worldwide Science, Google Scholar, Cochrane Library, PubMed, and Web of Science. Boolean terms were used to combine the keywords for the condition, context, and population to search: Consequently, Mental health illness*(tab) OR Mental health problem*(tiab) OR Mental Disorder*(tiab) OR Psychiatric Illness*(tiab) OR Psychiatric Disease*(tiab) OR Mental Illness*(tiab) OR Psychiatric Disorder*(tiab) OR Behavior Disorder*(tiab) OR Psychiatric Diagnosis*(tiab) OR Severe Mental Disorder*(tiab) OR depression(tiab) OR “Mental disorders“[MeSH Terms] AND Ethiopia(tiab) OR Federal republic of Ethiopia(tiab) OR “Ethiopia“[MeSH Terms] AND Adolescent*(tiab) OR Teen*(tiab) OR Teenager*(tiab) OR Youth*(tiab) OR School adolescent*(tiab) OR School age*(tiab) OR college student* (tiab) OR “adolescent“[MeSH Terms]. The literature was systematically searched in the specified database during the period from March 21, 2024, to April 27, 2024. The articles considered for this study were published between 2013 and 2024, up to the time of the search.
After the two authors (SDH & KWM) independently searched the original articles, any disagreements about the included articles were solved through dialogue and agreement in the presence of the third author (ATT). Using conventional Microsoft Excel sheets, ATT and SDH retrieved the data from the included papers and then transferred it to R statistical software for further analysis.
This systematic review and meta-analysis were presented according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses [20].
Eligibility criteria
Inclusion criteria
We included studies for this review: (1) conducted on the mental health of high school, preparatory and college students (on adolescents and youth), (2) The outcome is mental health problems that include depression or depression disorder, and all types of observational studies conducted in Ethiopia, and published in English.
Exclusion criteria
Upon repeated requests from the cross-referring writers, articles with insufficient details were removed. Reviews and reports were not included in this study.
Data extraction
We extracted all reported and this review objective-related data by using an independently prepared Microsoft Excel data extraction format. Data extraction format for the primary outcomes includes Authors, study period, publication year, study design, data collection tool, data analysis method, mean age of participants, study area-specific place where the study took place and region (according to Ethiopian political administration), sample size, response rate, and magnitude of depression.
For factors related to depression, the data extraction format was prepared for each specific variable separately in different sheets of Microsoft Excel. For each factor, we extracted the data in the form of two-by-two tables to calculate the odds ratio as an event with exposure or experiment with the event, total experiment with the event, event with control, and total with control. Any disagreements between the two authors during extractions were solved through discussion together with the third author.
Outcome measurements
This meta-analysis and systematic review study has two outcomes: the primary outcome was to determine the prevalence, while the secondary outcome was to identify the factors associated with depression among youth. Concerning factors variables, we calculated the odds ratio from the primary studies using the two-by-two tables.
Quality assessment
To assess the quality of the included cross-sectional studies, we used the Newcastle-Ottawa Scale tools [21]. The tool is divided into three main sections: (1) explores the study’s methodological quality; (2) reviews the studies’ comparability; and (3) evaluates the original publications’ quality of outcome measurement and statistical analysis.
Statistical analysis
The data were extracted using a Microsoft Excel™ format, and the data were exported from Microsoft Excel to R (software) for management and further analysis. The data were presented using a text, table, and graph and forest plot. For this meta-analysis and review data with missing value were excluding from analysis. But before excluding it from the analysis different attempts have been implemented to find the missing data. Including contacting to principal investigator to request full data set. Furthermore, to exclude the data from analysis the situation of the missing data were considered. If the main outcome of this meta-analysis and review were not affected, included for final analysis.
Evaluation of risk of bias
The heterogeneity among the proportion of the former studies was checked by using the I^2^ test together with the p-values (I^2^ = 97), p < 0.01). Due to the presence of significant heterogeneity between previous studies, a random-effects regression model was used to estimate the pooled depression among youth in Ethiopia. Additionally, subgroup analysis with some possible variables (region, sample mean variation and study participants) was complimented. To assess publication bias, a funnel plot and Egger test were used and it was asymmetry by visual inspection and the Egger’s test also showed the presence of publication bias (p < 0.0081).
Results
Primary articles search
From searched articles by using the earlier stated database and other repositories, 842 potential articles were identified and 345 were excluded due to duplication. By further reading the title of the article and abstracts from the remaining 497 articles, 299 articles were excluded due to irrelevant to the inclusion criteria. One hundred and ninety-eight articles were evaluated in whole text of the articles, then 174 articles were excluded for being irrelevant after careful reading. This systematic review and meta-analysis include only 15 articles that met the inclusion criteria (Fig. 1).
Fig. 1. Showing flow diagram showing the process of selecting articles for meta-analysis youth depression in Ethiopia, 2024
Features of original articles
For these studies, 15 articles fulfil the inclusion criteria and are included for systematic review and meta-analysis. All included studies were conducted with cross-sectional study designs. Ten studies collected data using the Patient Health Questionnaire (PHQ-9/A) [22–27], and Depression, Anxiety, and Stress Scale-21 Items (DASS-21) [28–31] while the remaining studies used the Beck Depression Inventory (BDI-II) [32, 33], Kutcher Adolescent Depression Scale (KADS) [34], Center for Epidemiological Studies-Depression (CES-D) [35] and Hospital Anxiety and Depression Scale (HADS) [36] (Table 1).
Table 1. Included studies characteristics of depression in Ethiopia, 2024 (n = 15)AuthorsStudy periodData collection toolsMean ageAreaSampleResponse rate %Prevalence%Chekol et al. [22]June 18 to July 16, 2022PHQ-918.15 ± 1.295Bahir Dar city58496.922.1Girma S et al. [23]2, April to 30, May 2018.PHQ-916.83 ± 1.3Jimma town56197.328Abebe et al. [32]May and June 2016BDI-II18.6 ± 3.024Addis Ababa53794.435.5Demoze et al. [34]May 01 to 30, 2016KADSN/AAddis Ababa46597.436.4Tirfeneh et al. [25]January 1–30/2019PHQ-9N/AAksum63099.0536.2Abera et al. [28]March 1 to 31, 2021DASS-2117.61 ± 1.83Sawla66398.652.1Gebreegziabher et al. [24]June 8 -June 24, 2022PHQ-9 AN/AGondar town14079828.21Nakie et al. [31]Apr-2021DASS-2118.59 ± 1.792North Gojjam84396.141.4Tarecha et al. [26]March to April 2021PHQ-9 A17.81 ± 1.47Bahir Dar city78196.319.8Gebremariam AT et al. [27]3 July to 7 July 2020PHQ-916.9 ± 1.813Awash 7 kilo39296.228.91Kebede et al. [36]April to May 2017HADS1.61 ± 0.65St. Paul Hospital27398.551.3Hambisa et al. [37]April 15 to 30, 2013BDI-II20.9 ± 2:17HU104098.326.8Simegn et al. [29]June 30 to July 30, 2020.DASS-2122.96Gondar42310046.3Melaku et al. [30]January 03 to 31, 2019DASS-2122.03 ± 2.62Arsi26598.152.3Lelisho et al. [35]September 11 to 25, 2020CES-DN/AMTU77910039.5
Data analysis and magnitude of depression
Overall depression prevalence among youths in Ethiopia was determined to be 36% (95% CI: 31% to 42%) (Fig. 2).
Fig. 2. Showing the proportion of youth depression in Ethiopia, 2024
The random effect model was applied to estimate the depression among youth in Ethiopia, due to the significant existence of heterogeneity among primary studies (I^2^ = 97%, p < 0.01). To identify the potential sources of heterogeneity, we examined subgroup analysis with the region, sample means variation and study participants that could be likely characteristics related to the heterogeneity. Addis Ababa is the area where more depressed youth were found next to South Nations, Nationalities, and Peoples’ Regional State (SNNPRS)and Undergraduate university students are 10% more depressed than high school students (Table 2). To assess publication bias, a funnel plot was used and it was asymmetry by visual inspection which indicates the presence of publication bias. The Egger’s test also showed the presence of publication bias (p < 0.0081).
Table 2. Subgroup prevalence of youth depression in Ethiopia, 2024 (n = 15)VariablesCharacteristicsNo, of studiesTotal ParticipantsPrevalence (95% CI)RegionAmhara5403831% (95% CI: 21;42)Oromia282640% (95% CI: 16;64)Addis Ababa3127541% (95% CI: 31;51)Tigray163036% (95% CI: 32;40)SNNSPRS2144246% (95% CI: 34;58)Afar139229% (95% CI: 24;34)Harari1104027% (95% CI: 24;30)Sample meanLower9413037% (95% CI: 30;44)Higher6551335% (95% CI: 25;44)Study participantHigh school students7530033% (95% CI: 24;41)Undergraduate university students5278043% (95% CI: 34;53)HIV positive youth153736% (95% CI: 32;40)Orphan centred adolescents146536% (95% CI: 32;41)Community resident adolescents156128% (95% CI: 24;32)
Factors associated with youth depression
Of the fifteen primary studies included in the review and meta-analysis, thirteen identified three variables that were significantly associated with depression.
Females were nearly three times more likely to be depressed (OR: 2.84, 95% CI: 1.37 to 6.89) as compared to male youth (Fig. 3).
Fig. 3. Showing sex difference and youth depression in Ethiopia,2024
Youths who use alcohol are 98% more likely depressed (OR: 1.98, 95% CI: 1.62 to 2.42) when compared to the youths who didn’t ever use alcohol (Fig. 4).
Fig. 4. Showing ever alcohol use and youth depression in Ethiopia,2024
Similarly, youths have 24 times the likelihood of not being depressed if they get social support (OR: 24.01, 95% CI: 11.68 to 49.35) compared to youths who lack social support (Fig. 5).
Fig. 5. Showing social support and youth depression in Ethiopia,2024
Discussion
Depression is one of the most common mental disorders worldwide. Reported prevalence is higher in developed countries due to better detection, while the actual burden in developing countries may be equally high or even higher but often remains hidden because of limited resources and underdiagnosis. Half of all mental health disorders start before the age of fourteen tackling this issue on a global level is saving the later life burden of mental health disorders and will take its part in achieving SDGs3 [5, 38].
In this study, the overall pooled prevalence of youth depression in Ethiopia was 36% (95% CI: 31% to 42%), which is higher than systematic review and meta-analysis studies conducted in different countries [39], in the USA [40], and in Bangladesh [41]. Geographic differences may be the cause of the discrepancy, which is related to environmental aspects such as social stability, political stability, economic standing, and work availability. Instabilities in politics and the economy are prevalent across Ethiopia. However this study is aligned with a single study depression prevalence conducted in Meghalaya, India [42], global systemic review and meta-analysis [43], in Uganda [44] in South Africa [45].
But the prevalence of this study is lower than a study conducted in six Middle East countries [46], in Nepalese youth [47], and in Chandigarh, India [48]. The discrepancy may arise from the fact that the majority of research was carried out in the COVID-19 pandemic era. Around the world, the pandemic was annoying, and this could lead to a rise in youth depression prevalence.
This systematic review and meta-analysis also pooled the factors associated with the occurrence of depression among youths.
In this review, female youths were 2.84 times more likely to be depressed as compared to male youths. This study was supported by WHO reports [5], studies in Canada [49] and in Ethiopia [50].
This gap may be caused by a variety of circumstances, such as the possibility that female hormone fluctuations may cause depression [49], premenstrual issues, relationship issues, teenage pregnancy, abuse, a lack of social support, and similar circumstances. Similarly, youths who had ever used alcohol were more depressed as compared to non-alcohol users. This finding is also supported by different studies [42, 51–53]. The relationship between depression and alcohol use may be reciprocal. People with depression might drink regularly to cope with their symptoms, while even infrequent drinkers may experience depressive symptoms due to alcohol’s effects or withdrawal. Although drinking may provide short-term relief, over time it often worsens depressive symptoms and overall well-being.
This meta-analysis and systematic review indicate that social support plays a major role in young people’s depression. When compared to young people who receive adequate social support, those who receive insufficient social support are over 24 times more likely to be depressed. This finding is confirmed by various studies [54–56]. This may be related to the belief that a complex interplay of biological, psychological, and social components leads to depression. Adolescent sadness decreases when they receive an acknowledgement from the community and have got chance to participate in local issues. On the other hand, depression will be exacerbated as a youth is socially rejected, faces financial difficulty, instability in politics, economic crises, and other dysfunctional circumstances and conditions that worsen the depression of an individual’s life.
Strengths and limitations of the study
The strength of this study is that it has tried to comprehensively review youth depression in Ethiopia. Additionally, the review addressed the main databases for this meta-analysis and systematic review, however, this systematic review and meta-analysis also have several limitations should be noted. Studies that were not fully accessible were excluded, potentially affecting the generalizability of the findings. Additionally, variations in the measurement tools used across the included studies may have influenced the pooled estimates of depression.
Conclusion
This systematic review and meta-analysis revealed a substantially high prevalence of depression among youth in Ethiopia. Policymakers should acknowledge the significant impact of social support on mental health, given that inadequate support may result in severe consequences, and should implement strategies to enhance awareness and interventions at both community and family levels to effectively reduce the burden of youth depression.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Desa U. The sustainable development goals report 2023: special edition-July 2023. New York, USA, 2023.
- 2Organization WH. World mental health report: Transforming mental health for all. 2022.
- 3Organization WH. Depression and other common mental disorders: global health estimates. 2017.
- 4Nair S et al. Epidemiological survey of mental health in adolescent school children of Gujarat, India. BMJ Paediatrics Open, 2017. 1(1).10.1136/bmjpo-2017-000139 PMC 586219629637154 · doi ↗ · pubmed ↗
- 5Health FD. R.o.E.M.o., National Mental Health Strategy 2012/13–2015/16. Public policy document, Federal Democratic Republic of Ethiopia, 2012.
- 61. 9(3):194–5., D.A.T.m.h.c.o.w.i.n.E.w.w.s.b.c.T.L.P.M
- 7Page MJ et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ, 2021. 372.10.1136/bmj.n 71PMC 800592433782057 · doi ↗ · pubmed ↗
- 8Gebreegziabher ZA, Eristu R, Molla A. Depression, Anxiety, Somatic symptom and their determinants among High School and Preparatory School Adolescents in Gondar Town, Northwest Ethiopia, 2022. Non-recursive Structural Equation Modeling. med Rxiv, 2023: p. 2023.01. 27.23285096.