Socioeconomic value of treatments for chronic idiopathic constipation in Japan
Atsushi Nakajima, Aki Unno, Takumi Ota, Ayako Shoji, Tatsuhiro Uenishi, Ataru Igarashi

TL;DR
This study compares the cost-effectiveness and quality of life outcomes of three treatments for chronic idiopathic constipation in Japan.
Contribution
The study introduces a novel approach by including non-traditional socioeconomic factors like productivity loss and caregiver burden in evaluating treatment effectiveness.
Findings
Elobixibat 10 mg was associated with lower total costs and better quality of life compared to linaclotide and lubiprostone.
Sensitivity analyses confirmed the robustness of elobixibat's cost-effectiveness, though it was sensitive to changes in drug effectiveness.
Scenario analyses showed consistent results when adjusting for discounting and mortality assumptions.
Abstract
Chronic idiopathic constipation (CIC) is a common disorder associated with socioeconomic burden. The aim of this study was to quantify the socioeconomic burden of CIC, including non-traditional value elements, and to compare the cost-effectiveness of 3 treatments for CIC with unique mechanisms of action: elobixibat 10 mg, linaclotide 0.5 mg, and lubiprostone 48 μg. We compared medical costs and CIC-specific quality of life (QoL) among patients treated with elobixibat 10 mg, linaclotide 0.5 mg, and lubiprostone 48 μg using a Markov cohort simulation model of 4 mutually exclusive health states (CIC, unimproved, improved, and death) with 4-week cycles and a 2-year time horizon. In addition to costs and QoL scores, which were discounted at 2.0% per year, we considered productivity loss and caregiver burden for patients requiring assistance with daily living and defecation management.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
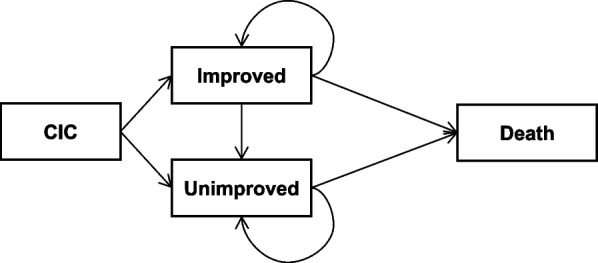 Figure 1
Figure 1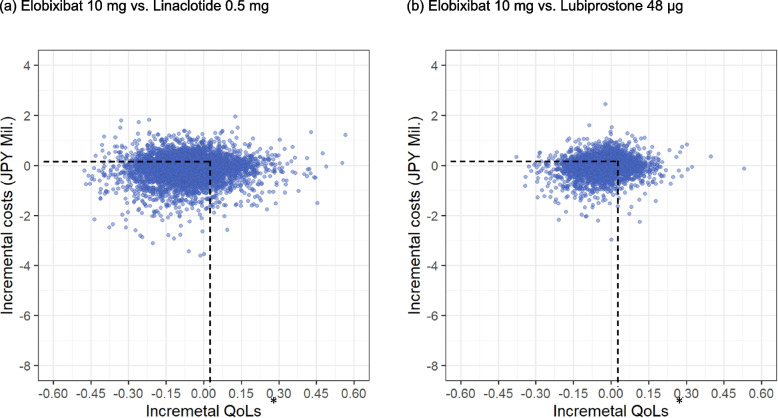 Figure 2
Figure 2- —EA Pharma Co., Ltd.
- —Mochida Pharmaceutical Co., Ltd.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal motility and disorders · Gastroesophageal reflux and treatments · Congenital gastrointestinal and neural anomalies
Introduction
Chronic idiopathic constipation (CIC) is a common disorder that physicians treat in clinical practice. CIC is associated with increased risk of all-cause death, cardiovascular disease, and stroke [1] and can cause a variety of issues that contribute to socioeconomic burden, including abdominal pain, sleep disturbance, and productivity loss [2]. However, the impact of CIC on society in Japan is not as well understood as in other countries.
Guidelines for CIC management in Japan have established the role of drugs with unique mechanisms of action (elobixibat, lubiprostone, and linaclotide) for patients whose symptoms do not improve with first-line treatments, such as osmotic and stimulant laxatives, lactulose, and polyethylene glycol [2]. A network meta-analysis (NMA) of randomized clinical trials (RCTs) of drugs found differences in efficacy [3]. However, higher efficacy does not necessarily justify selection because the cost of these drugs vary and their overall costs and benefits have not yet been compared.
A cost-effectiveness study comparing lubiprostone and linaclotide in the United States found that the 2 drugs had similar effectiveness but different in medical costs [4, 5]; however, this analysis included only direct costs. Globally, rising drug prices have driven discussions about how to measure and communicate the full value of treatments beyond medical costs and quality of life (QoL). In 2018, a “value flower” framework was proposed. This framework consists of 12 elements of value [6], including traditional value elements of socioeconomic burden like quality-adjusted life-years, net costs, and productivity loss, and newer concepts, such as family spillover effects and insurance value [7]. Recent studies have expanded the scope of disease burden to include other value elements like caregiver burden, impact on daily life and society, and happiness [8–10]. Given the diverse daily challenges associated with CIC, the burden of this condition likely extends beyond medical costs alone.
The aim of this study was to quantify the socioeconomic burden of CIC in clinical practice using both traditional and non-traditional value elements and to compare the cost-effectiveness of elobixibat, linaclotide, and lubiprostone.
Methods
Model overview
This cost-effectiveness analysis compared costs and quality of life (QoL) among patients treated with elobixibat 10 mg, linaclotide 0.5 mg, and lubiprostone 48 μg. We developed a Markov cohort simulation model with 4 mutually exclusive health states (CIC, unimproved, improved, and death), a 4-week cycle, and 2-year time horizon based on previous cost-effectiveness studies on CIC and irritable bowel syndrome with constipation [11–13] (Fig. 1). We chose this simple model to minimize the number of hypothetical parameters and enhance transparency and reproducibility, because of the lack of long-term studies on actual disease transition in patients with CIC undergoing treatment with these drugs in Japan. Costs and QoL were discounted at 2.0% per year, which is the rate recommended for cost-effectiveness analyses in Japan [14]. The mean ± SD age of the initial population was assumed to be 62.9 ± 10.1, based on a survey of patients in Japan with any bowel movement disturbance [15].Fig. 1. Model structure
Patients with CIC started 1 of the 3 treatments at the start of the model and transitioned to either the unimproved or improved state based on the proportion of patients achieving 3 or more spontaneous bowel movements (SBMs) per week. This threshold was established based on the following: (1) in the Evidence-Based Clinical Guidelines for Chronic Constipation 2023 in Japan, the Japanese Gastroenterological Association defines one of the diagnostic criteria of CIC as “fewer than 3 spontaneous bowel movements per week” [2]; (2) the Cleveland Clinic Constipation Scoring System assigns a score of 0 for fewer than 2 bowel movements per week [16]; and (3) SBM responders are defined as patients with 3 or more SBMs per week and at least 1 additional SBM per week from baseline [17–19].
Patients generally continued their initial treatment and remained in the state they transitioned into after initiation. However, based on expert opinion, 15% of patients in the improved state transitioned to the unimproved state per year irrespective to treatment types, reflecting the likelihood of symptom recurrence despite continued treatment. Otherwise, patients remained in their respective states until death. No patients in the unimproved state transitioned to the improved state.
This trial was registered with the UMIN Clinical Trials Registry (registration number: UMIN000055903; registration date: 21 October 2024). All analyses were based only on secondary information and no human participant was enrolled for this study. The model was programmed in R using a previously validated open-source model [20]. AS developed an initial model, which was updated via an internal validation and quality check by TU.
Model parameters
Model parameters are shown in Table 1.Table 1. Model parametersParametersValue(per cycle)DetailsSourceTransition probabilityImproved (SBM goal achievement)Elobixibat0.6012458Estimated using NMA resultImproved to unimproved0.0124Converted to a 28-day rate15% per year, based on expert opinionmortality0.0010Converted to a 28-day rate12.9 per 1000 people in 2022 [21]Risk ratio to EloElobixibat1.0000linaclotide0.7155Estimated using NMA resultlubiprostone0.8829Estimated using NMA resultQoLImproved state1.64Marquis et al. [22]Unimproved state1.88Marquis et al. [22]Treatment costs (JPY)Drug price Elobixibat4,715.2NHI drug price listlinaclotide3,869.6NHI drug price listlubiprostone5,600.0NHI drug price listAdditional treatment in the unimproved stateDisimpaction333.3Converted to 28-day costsNHI Medical Service Fee Points (J022-2): once every 12 weeksEnema1,300.0Converted to 28-day costsNHI Medical Service Fee Points (J022): once every 2 weeksCaregiving costs (JPY)Improved state303.3249% of population aged ≥ 65 years (41.74669) × % of time per day for care in improved state (4.0238095) × % of patients who need care (6.2952) × average wage (286,839.6)Unimproved state437.9366% of population aged ≥ 65 years (41.74669) × % of time per day for care in unimproved state (5.8095238) × % of patients who need care (6.2952) × average wage (286,839.6)41.74669%% of population aged ≥ 65 years62.9 ± 10.1 [15]4.0238095%% of time per day for care in improved state16.9 min per work day (7 h) [23]5.8095238%% of time per day for care in unimproved state24.4 min per work day (7 h) [23]6.2952%% of patients who need care18.3% (number of people in the population aged 65 or over requiring care) [24] † × 34.4% (proportion requiring defecation management) [25]286,839.6Average wage311,800 per month [26], converted to 28-day rateProductivity loss (JPY)Improved state34,371.1456% of population aged < 65 years (58.25331) × % of total work productivity impairment for improved state (20.57) × average wage (286,839.6)Unimproved state58,783.5149% of population aged < 65 years (58.25331) × % of total work productivity impairment for unimproved state (35.18) × average wage (286,839.6)58.25331%% of population aged < 65 years62.9 ± 10.1 [15]20.57%% of total work productivity impairment for improved state20.57% (total work productivity impairment in the matched cohort without CIC) [27]35.18%% of total work productivity impairment for unimproved state35.18% (total work productivity impairment in the cohort diagnosed with CIC) [27]286,839.6Average wage311,800 per month [26], converted to 28-day rateCIC* Chronic idiopathic constipation, elo Elobixibat, JPY Japanese yen, NHI National health insurance, NMA Network meta-analysis, QoL Quality of life, SBM Spontaneous bowel movement^*^The unit costs for elobixibat 10 mg, linaclotide 0.5 mg, and lubiprostone 48 μg were calculated by multiplying the cost per day from the unit price, listed as of the fiscal year 2024 and 28 days^†^Calculated by dividing the number of people who needed care services in Japan in 2022 (6,582,416) by the number of people aged 65 years and over in 2022 (36,027,000)
We performed an NMA using the same methods as the previous NMA report, including the same 7 RCTs that reported mean change in SBMs per week for the target drugs (S1 Appendix in Supporting Material), except for those on magnesium oxide and polyethylene glycol [3]. Authors from pharmaceutical companies had no involvement in the NMA. To estimate the proportion of patients achieving 3 or more SBMs per week, we randomly sampled 1000 numbers based on the distribution of the synthesized mean and reported standard deviations (SDs) of the eligible studies and calculated the proportion of numbers greater than 3, following a previous methodology [28]. The resulting proportions were 0.6012458 for elobixibat 10 mg, 0.4302036 for linaclotide 0.5 mg, and 0.5308396 for lubiprostone 48 μg.
QoL was based on the Patient Assessment of Constipation (PAC)-QoL score, a CIC-specific measure that has been used in recent clinical trials and observational studies of patients with CIC to capture disease-specific benefits provided by the target drugs [29–31]. In this measure, higher values correspond to more severe symptoms. Reported values in patients with 3 or more and 0–1 complete evacuations [22] were used for the improved and unimproved states, respectively. These values were accumulated per cycle and divided by 26, the number of cycles in the 2-year time horizon. We also calculated the mean duration in the “improved” health state.
Drug costs were incurred per cycle in both the improved and unimproved states, and additional bowel management costs (i.e., disimpaction every 12 weeks and enema every 2 weeks) were included in the unimproved state. The unit costs for f elobixibat 10 mg, linaclotide 0.5 mg, and lubiprostone 48 μg were calculated based on the cost per day from the unit price, listed as of the fiscal year 2024 (Table 1). Caregiver costs were also considered for patients aged 65 years or over requiring daily living assistance, as this care includes defecation management. These costs were estimated by multiplying (1) the proportion of time per caregiver workday spent on defecation management, (2) the proportion of patients who need daily care including defecation management, and (3) the average wage [26]. For the first value, we used the number of minutes spent on defecation care in patients before (for the unimproved state) and after (for the improved state) treatment with the target drugs [23], converted into proportions of a 7-h day (assumed typical daily working hours for caregivers). The second value was derived by multiplying the proportion of the population aged 65 years and over using any care services [24] and the proportion of that population requiring comprehensive daily care, which includes defecation management [25]. We set the threshold for productivity loss and use of care services as 65 years because employment until 65 years is strongly recommended for employees who want it in Japan as of April 1, 2025.
We additionally considered productivity loss in patients with CIC aged less than 65 years using work impairment data reported by Tomita et al. [27] for patients with (for the unimproved state) and without (for the improved state) CIC, multiplied by the average wage [26].
Sensitivity analyses
To investigate the uncertainty inherent in the model, deterministic sensitivity analysis (DSA), probabilistic sensitivity analysis (PSA), and scenario analyses were conducted. In the DSA, all input parameters were varied by ± 20% of the base-case value. PSAs were conducted through 10,000 Monte Carlo simulations by sampling from distributions assigned to input parameters (Supplemental Table 2).
Additionally, 6 scenario analyses were conducted. In Scenario 1, we included 2 add-on treatments for patients who remained in the unimproved state for 3 cycles to reflect real clinical practice for such patients. The add-on treatments included stimulant laxatives (senna extract or sennoside, JPY 186.4 per cycle) and osmotic laxatives (magnesium oxide, JPY 365.4 per cycle). We also considered a 4% rate of improvement from the unimproved state, based on rates of 2–6% used in a previous study [12]. In Scenario 2, we used a 0 and 3% discount rates for both costs and QoL, given the short 2-year time horizon. In Scenario 3, we used a mortality rate for the unimproved state 1.19 times higher than that for the improved state, based on previous research demonstrating poorer survival in individuals with symptoms of chronic constipation [32]. In Scenario 4, we extended the time horizon to 5 and 10 years to assess the long-term trend. In Scenario 5, we used alternative overall work impairment rates with less difference between the improved and unimproved states (25.29% and 35.54%, respectively) [33]. In Scenario 6, we excluded caregiving burden, because the data on time spent providing care involved a limited number of nurses.
The statistical analysis software R (version 4.3.0, The R Foundation for Statistical Computing, Vienna, Austria) was used for analysis.
Results
Base-case results
Total costs for 2 years of elobixibat 10 mg, linaclotide 0.5 mg, and lubiprostone 48 μg were 1,306,890, 1,383,131, and 1,368,940 Japanese yen (JPY), respectively. QoL scores were 1.697, 1.731, and 1.711, respectively. Patients treated with elobixibat 10 mg showed lower total costs and better QoL scores than those treated with linaclotide 0.5 mg (JPY + 76,241, QoL + 0.034) and lubiprostone 48 μg (JPY + 62,050, QoL + 0.014) (Table 2).Table 2 The result of base-case analysisStrategyCosts (JPY)QoLDuration in improved state (mean) (cycles)MedicalCaregivingProductivitylossTotal∆(vs. elo)∆(vs. elo)∆(vs. elo)Elobixibat 10 mg138,2669,2521,159,3721,306,8901.69713.273Linaclotide 0.5 mg123,1009,7541,250,2771,383,13176,2411.7310.0349.476−3.797Lubiprostone 48 μg162,9839,4571,196,5001,368,94062,0501.7110.01411.722−1.551elo* elobixibat, JPY Japanese yen, QoL quality of life*Based on previously reported values of 1.64 (improved state) and 1.88 (unimproved state), which were accumulated every cycle and divided by 26, the number of cycles in the 2-year time horizon
Sensitivity analysis
The DSA showed that the base-case results were generally robust to changes in most input parameters but were sensitive to the effectiveness of elobixibat and lubiprostone; effectiveness of − 20% for elobixibat and + 20% for lubiprostone resulted in higher costs and poorer QoL for elobixibat 10 mg than lubiprostone 48 μg (Table 3).Table 3 The result of deterministic sensitivity analyses (±20% of the base-case value)ParameterStrategyLower (−20%)Upper (+20%)Costs (JPY)QoLCosts (JPY)QoL∆(vs. elo)∆(vs. elo)∆(vs. elo)∆(vs. elo)EfficacyelobixibatElobixibat 10 mg1,375,0351.7211,238,7461.673Linaclotide 0.5 mg1,383,1318,0961.7310.0101,383,131144,3851.7310.058Lubiprostone 48 μg1,368,940−6,0951.711−0.0101,368,940130,1941.7110.038linaclotideElobixibat 10 mg1,306,8901.6971,306,8901.697Linaclotide 0.5 mg1,453,026146,1361.7480.0511,355,73248,8421.7140.017Lubiprostone 48 μg1,368,94062,0501.7110.0141,368,94062,0501.7110.014lubiprostoneElobixibat 10 mg1,306,8901.6971,306,8901.697Linaclotide 0.5 mg1,383,13176,2411.7310.0341,383,13176,2411.7310.034Lubiprostone 48 μg1,406,88999,9991.7320.0351,286,526−20,3641.690−0.007QoLElobixibat 10 mg1,306,8901.3571,306,8902.036Linaclotide 0.5 mg1,383,13176,2411.3850.0281,383,13176,2412.0770.041Lubiprostone 48 μg1,368,94062,0501.3690.0121,368,94062,0502.0530.017Medical costElobixibat 10 mg1,302,9341.6971,310,8481.697Linaclotide 0.5 mg1,377,95875,0241.7310.0341,388,30477,4561.7310.034Lubiprostone 48 μg1,364,48761,5531.7110.0141,373,39462,5461.7110.014Drug costelobixibatElobixibat 10 mg1,283,1941.6971,330,5871.697Linaclotide 0.5 mg1,383,13199,9371.7310.0341,383,13152,5441.7310.034Lubiprostone 48 μg1,368,94085,7461.7110.0141,368,94038,3531.7110.014linaclotideElobixibat 10 mg1,306,8901.6971,306,8901.697Linaclotide 0.5 mg1,363,68456,7941.7310.0341,402,57895,6881.7310.034Lubiprostone 48 μg1,368,94062,0501.7110.0141,368,94062,0501.7110.014lubiprostoneElobixibat 10 mg1,306,8901.6971,306,8901.697Linaclotide 0.5 mg1,383,13176,2411.7310.0341,383,13176,2411.7310.034Lubiprostone 48 μg1,340,79833,9081.7110.0141,397,08390,1931.7110.014Productivity lossElobixibat 10 mg1,075,0161.6971,538,7651.697Linaclotide 0.5 mg1,133,07658,0601.7310.0341,633,18694,4211.7310.034Lubiprostone 48 μg1,129,64054,6241.7110.0141,608,24069,4751.7110.014Caregiving costElobixibat 10 mg1,305,0401.6971,308,7411.697Linaclotide 0.5 mg1,381,18076,1401.7310.0341,385,08276,3411.7310.034Lubiprostone 48 μg1,367,04962,0091.7110.0141,370,83262,0911.7110.014elo elobixibat, JPY Japanese yen, QoL quality of life*Based on previously reported values of 1.64 (improved state) and 1.88 (unimproved state), which were accumulated every cycle and divided by 26, the number of cycles in the 2-year time horizon
The PSA showed that approximately 72.3% and 64.0% of observations showed better QoL for elobixibat 10 mg than linaclotide 0.5 mg and lubiprostone 48 μg, respectively. Additionally, 57.2% and 51.6% of observations showed lower costs for elobixibat 10 mg than linaclotide 0.5 mg and lubiprostone 48 μg, respectively. Overall, 41.2% and 34.0% of observations showed better QoL and lower costs for elobixibat 10 mg than linaclotide 0.5 mg and lubiprostone 48 μg, respectively (Table 4) (Fig. 2).Table 4 The result of probabilistic sensitivity analysisStrategyCosts (JPY)QoLBase-casePSABase-casePSATotal∆(vs. elo)95% CrI†∆(vs. elo)95% CI†Elobixibat 10 mg1,306,8901.697Linaclotide 0.5 mg1,383,13176,24168,507 – 83,9751.7310.0340.032 - 0.036Lubiprostone 48 μg1,368,94062,05057,020 – 67,0801.7110.0140.013 - 0.015elo* elobixibat, JPY Japanese yen, QoL quality of life, PSA probabilistic sensitivity analysis*Based on previously reported values of 1.64 (improved state) and 1.88 (unimproved state), which were accumulated every cycle and divided by 26, the number of cycles in the 2-year time horizon†Derived through 10000 Monte Carlo simulations by sampling from distributions assigned to input parametersFig. 2 The result of the probabilistic sensitivity analysis
Scenario analyses
In Scenario 1, in which patients who remained in the unimproved state for 3 cycles received additional stimulant or osmotic laxatives, total costs increased for all target drugs. Elobixibat was associated with lower total costs (Table 5) and better QoL (unchanged from base-case analysis) than the other 2 drugs, but the difference in total costs decreased (Table 5).Table 5 The result of scenario analysis: add-on treatments in the unimproved state (additional costs and transition from the unimproved to improved state)StrategyTotal costs (JPY)∆ (vs. elo)QoL*∆ (vs. elo)Add-on costs (stimulant) (JPY)∆ (vs. elo)Add-on costs (osmotic) (JPY)∆ (vs. elo)Elobixibat 10 mg1,210,3591.6631,4102,764Linaclotide 0.5 mg1,254,64044,2811.6860.0231,84744,7183,62145,138Lubiprostone 48 μg1,259,35648,9971.6720.0091,58949,1763,11449,347elo Elobixibat, JPY Japanese yen, QoL Quality of life^*^Based on previously reported values of 1.64 (improved state) and 1.88 (unimproved state), which were accumulated every cycle and divided by 26, 65, and 130, the number of cycles in the 2-, 5-, and 10-year time horizon
Scenario 2, in which no discounting and 3% discount rate were applied for costs and QoL, and Scenario 3, in which higher mortality was assumed for the unimproved state, yielded similar results to the base-case analysis (Tables 6 and 7).Table 6 The result of scenario analysis: other discount ratesStrategyCosts (JPY)QoLMedicalCaregivingProductivity lossTotal∆(vs. elo)∆(vs. elo)0%Elobixibat 10 mg141,1959,4491,184,0841,334,7281.733Linaclotide 0.5 mg125,7049,9601,276,7981,412,46277,7341.7680.035Lubiprostone 48 μg166,4289,6581,221,9511,398,03763,3091.7470.0143%Elobixibat 10 mg136,8139,1551,147,1121,293,0801.679Linaclotide 0.5 mg121,8099,6511,237,1191,368,57975,4991.7130.034Lubiprostone 48 μg161,2749,3581,183,8741,354,50661,4261.6930.014elo* Elobixibat, JPY Japanese yen, QoL Quality of life^^Based on previously reported values of 1.64 (improved state) and 1.88 (unimproved state), which were accumulated every cycle and divided by 26, 65, and 130, the number of cycles in the 2-, 5-, and 10-year time horizonTable 7 The result of scenario analysis: higher mortality in the unimproved stateStrategyCosts (JPY)QoLMedicalCaregivingProductivity lossTotal∆(vs. elo)∆(vs. elo)Elobixibat 10 mg138,0989,2411,157,8161,305,1551.695Linaclotide 0.5 mg122,9059,7381,248,1851,380,82875,6731.7290.034Lubiprostone 48 μg162,7659,4441,194,7251,366,93461,7791.7090.014elo Elobixibat, JPY Japanese yen, QoL Quality of life^*^Based on previously reported values of 1.64 (improved state) and 1.88 (unimproved state), which were accumulated every cycle and divided by 26, 65, and 130, the number of cycles in the 2-, 5-, and 10-year time horizon
Scenario 4, in which the time horizon was extended, yielded similar results to the base-case analysis (Table 8), but the difference in QoL between drugs was reduced because a greater proportion of patients remained in the unimproved state over time (Supplementary Figure S4).Table 8 The result of scenario analysis: longer time horizonScenarioStrategyCosts (JPY)QoLMedicalCaregivingProductivity lossTotal∆(vs. elo)∆(vs. elo)5-yearElobixibat 10 mg338,91122,8282,905,0813,266,8201.638Linaclotide 0.5 mg300,03523,7953,080,3103,404,140137,3201.6650.027Lubiprostone 48 μg396,64423,2232,976,6503,396,517129,6971.6490.01110-yearElobixibat 10 mg645,52243,7725,656,3966,345,6901.535Linaclotide 0.5 mg568,16645,1025,897,5846,510,852165,1621.5530.018Lubiprostone 48 μg749,94044,3155,754,9046,549,159203,4691.5430.008elo* Elobixibat, JPY Japanese yen, QoL Quality of life^*^Based on previously reported values of 1.64 (improved state) and 1.88 (unimproved state), which were accumulated every cycle and divided by 26, 65, and 130, the number of cycles in the 2-, 5-, and 10-year time horizon
In Scenario 5, assuming overall work impairment rates with less margin between the improved and unimproved states [33], and Scenario 6, excluding caregiving burden, the difference in total costs between drugs decreased, but overall results were similar (Tables 9 and 10).Table 9 The result of scenario analysis: no caregiving burdenStrategyCosts (JPY)QoLMedicalCaregivingProductivity lossTotal∆(vs. elo)∆(vs. elo)Elobixibat 10 mg138,26601,159,3721,297,6381.697Linaclotide 0.5 mg123,10001,250,2771,373,37775,7391.7310.034Lubiprostone 48 μg162,98301,196,5001,359,48361,8451.7110.014elo* Elobixibat, JPY Japanese yen, QoL Quality of life^^Based on previously reported values of 1.64 (improved state) and 1.88 (unimproved state), which were accumulated every cycle and divided by 26, 65, and 130, the number of cycles in the 2-, 5-, and 10-year time horizonTable 10 The result of scenario analysis: higher overall impairment in the improved stateStrategyCosts (JPY)QoLMedicalCaregivingProductivity lossTotal∆(vs. elo)QoL*∆(vs. elo)Elobixibat 10 mg138,2669,2521,269,3011,416,8191.697Linaclotide 0.5 mg123,1009,7541,333,0781,465,93249,1131.7310.034Lubiprostone 48 μg162,9839,4571,295,3491,467,78950,9701.7110.014elo Elobixibat, JPY Japanese yen, QoL Quality of life^*^Based on previously reported values of 1.64 (improved state) and 1.88 (unimproved state), which were accumulated every cycle and divided by 26, 65, and 130, the number of cycles in the 2-, 5-, and 10-year time horizon
Discussion
We investigated the cost-effectiveness of 3 CIC treatments with unique mechanisms of action and found that elobixibat 10 mg was associated with lower costs and higher QoL over 2 years than linaclotide 0.5 mg and lubiprostone 48 μg. This is the first study comparing the cost-effectiveness of these 3 drugs as treatments for CIC. In addition to traditional value elements such as medical costs, QoL, and productivity loss, we also included caregiving costs as an additional value element. However, the difference in QoL between drugs was smaller than the change reported in patients who self-rated their CIC as “minimally improved” (− 0.55) [22].
The results of the DSA showed that the parameter with the highest impact on the base-case results was drug effectiveness. Although the effectiveness values were derived from an NMA of RCT data, we applied a ± 20% variation (sufficiently wider variability than expected in clinical settings) to robustly assess the impact of uncertainty. However, because the settings in RCTs may differ from actual clinical conditions, and given the uncertainty in efficacy suggested in the previous NMA study [3], ongoing evaluation of real-world efficacy is important to refine these cost-effectiveness estimates further. The results of the PSA suggest that elobixibat was associated with better QoL but no superiority in total costs.
The model used in this study was based on previously published simple models for CIC [11–13]. To validate its applicability to real-world clinical conditions, we performed 6 scenario analyses to account for factors such as add-on treatment for patients in the unimproved state, different discount and mortality rates, longer time horizons, and a smaller difference in productivity loss between the improved and unimproved states and found that all of them had a limited impact on the base-case results, indicating the robustness of our results.
Previous cost-effectiveness studies in the United States have examined linaclotide and lubiprostone. One study estimated monthly medical costs of 727 U.S. dollars (USD) for linaclotide and USD 737 for lubiprostone (equivalent to 2-year costs of about JPY 2,617,200 and 2,653,200, respectively [1 USD = 150 JPY]) [5], while another study of patients treated with linaclotide reported medical costs of USD 33,453 (JPY 5,017,950) and productivity loss of USD 36,972 (JPY 5,545,800) [34]. However, given that drug costs are significantly higher in the US than in Japan (linaclotide USD 523 [35] vs 28.0, lubiprostone USD 374 [35] vs. 40.6), these results are not directly applicable to the Japanese setting. Nonetheless, both the US and Japanese studies indicate that the cost of productivity loss exceeds that of medical treatment. Recent surveys of Japanese patients with CIC reported annual productivity losses of JPY 1.218 million and 1.343 million [27, 36], which are comparable to our results if all patients were assumed at work (JPY 0.995–1.073 million per year), particularly considering that more than half of patients remained in the improved state throughout the study period.
In Japanese clinical guidelines, all 3 study drugs are recommended equally [2], with no specific recommendations differentiating them. However, the drugs have slightly different unit prices (Table 1) and effectiveness, as reported in a previous study [3]. Recently, there has been increasing focus on CIC-related symptoms, as CIC involves various symptoms that do not necessarily impose large medical costs but can significantly impact daily life and work productivity [36]. Additionally, some symptoms that exacerbate CIC can be improved by new drugs [37]. The latest Japanese guidelines recommend considering symptoms at diagnosis [2]. Therefore, when selecting treatments for CIC, it is important to consider not only therapeutic effects, such as SBMs, but also other benefits, including improved QoL, reduced productivity loss, and reduced caregiver burden. In the present study, we considered an expanded socioeconomic burden beyond traditional value elements and found that elobixibat 10 mg was likely more cost-effective than the comparators. The cost-effectiveness of the subject drugs may change when considering their unique mechanisms of action (elobixibat: water secretion, promotion of colonic peristalsis, and restoration of the urge to defecate; linaclotide: activation of guanylate cyclase C, secretion of chloride ion and bicarbonate ion into the intestinal lumen, and concomitant fluid secretion; lubiprostone: activation of the type 2 chloride ion channel, promotion of the secretion of electrolytes and fluid into the intestinal tract), which are thought to influence CIC-related symptoms [38]. Patients with CIC are often unaware of the broader socioeconomic burdens associated with their condition, but providing this information along with data on clinical efficacy may help guide treatment selection and encourage adherence through communication between patients and physicians. We focused on CIC-specific clinical values, which is narrow in terms of policy implications, but our results may have broader implications for therapeutic decision-making, similarly to other therapeutic areas where numerous treatment options exist for a given condition.
Limitations of this study
This study has 2 important limitations. First, the base-case results showed some uncertainty, primarily driven by drug efficacy. We believe NMA is a reliable method to quantitatively synthesize efficacy data from RCTs, but the observed heterogeneity may contribute to uncertainty in our results (S1 Appendix). If real-world efficacy differs from RCT data, further research using real-world evidence will be necessary to refine cost-effectiveness estimates and strengthen generalizability. Second, although we considered an expanded set of cost-effectiveness elements beyond traditional ones, our analysis was limited to elements with quantifiable data, and other elements may affect cost-effectiveness. If data on these elements in Japan becomes available, future studies could more comprehensively evaluate the value of CIC treatments.
Other limitations are as follows: (1) We developed the simple and versatile model to enhance transparency and reproducibility, but it has limited ability to capture state- or drug-specific transitions, such as tolerability and adverse effects commonly seen in clinical practice. If these factors are considered, the results might differ; for example, a recent study reported a difference in the number needed to harm between drugs [29]. (2) We used a disease-specific measure of QoL, which has the advantage of representing disease-specific benefits and issues, but for comprehensive comparison between diseases in the context of health technology assessments, mapping to generic health utility measures is required. (3) We assumed a 4% improvement rate from the use of add-on stimulant or osmotic laxatives for patients who remained in the unimproved state, although no data were available to support it. (4) Our results may not be applicable to populations with substantially different responses to the target drugs than the Japanese population. (5) The results of this study may be influenced by factors such as the use of generic drugs.
Conclusions
Considering the medical costs, QoL, productivity loss, and caregiver burden associated with CIC treatments, elobixibat 10 mg was associated with better QoL and lower costs than linaclotide 0.5 mg and lubiprostone 48 μg.
Supplementary Information
Supplementary Material 1: Supporting_material_Socioeconomic value for CIC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Center for Outcomes Research and Economic Evaluation for Health. Guideline for Preparing Cost-Effectiveness Evaluation to the Central Social Insurance Medical Council. Available from: https://c 2h.niph.go.jp/tools/guideline/guideline_en.pdf. Accessed 31 Jan 2025.
- 2Incerti D, Jensen J. Applied cost-effectiveness modeling with R 2022. Available from: https://hesim-dev.github.io/rcea/slides-4hr.pdf. Accessed 31 Jan 2025.
- 3Director-General for Statistics, Information System Management and Industrial Relations, Ministry of Health. Labour and Welfare vital Statistics of Japan 2022. (in Japanese) Available from: https://www.mhlw.go.jp/toukei/saikin/hw/jinkou/houkoku 22/dl/all.pdf. Accessed 31 Jan 2025.
- 4Labour and Welfare, Ministry of Health. Annual Health, Labour and Welfare Report 2022. Available from: https://www.mhlw.go.jp/wp/hakusyo/kousei/21/dl/1-02.pdf. Accessed 31 Jan 2025. in Japanese.
- 5Cabinet Office. Annual Report on the Ageing Society 2021. Available from: https://www 8.cao.go.jp/kourei/whitepaper/w-2021/html/zenbun/s 1_2_2.html. Accessed 31 Jan 2025. in Japanese.
- 6Labour and Welfare,. Ministry of Health. Basic Survey on Wage Structure 2022. Available from: https://www.mhlw.go.jp/english/database/db-l/basicsurvey/xls/2022.xlsx. Accessed 31 Jan 2025.
- 7Institute for Clinical and Economic Review. Eculizumab and Efgartigimod for the Treatment of Myasthenia Gravis: Effectiveness and Value (final report). 20 Oct 2021. Available from: https://icer.org/wp-content/uploads/2021/03/ICER_Myasthenia-Gravis_Final-Report_Unmasked_Data.pdf. Accessed 31 Jan 2025.