Aripiprazole-Induced Priapism in a Pediatric Patient: A Case Report
Sebastian G Tobia Gonzalez, Gaayana Raju, Leon I Smith-Harrison

TL;DR
A child developed priapism after taking aripiprazole, highlighting the need for early recognition and conservative treatment in pediatric cases.
Contribution
Reports a rare case of aripiprazole-induced priapism in a pediatric patient and emphasizes the effectiveness of conservative management.
Findings
An 8-year-old boy developed priapism after inadvertent aripiprazole administration.
Conservative management successfully resolved the priapism without surgical intervention.
Doppler ultrasound showed normal penile blood flow without thrombosis.
Abstract
Drug-induced non-ischemic priapism is a rare but critical condition in children. Aripiprazole, an atypical antipsychotic, has been associated with priapism, mostly in adults. Prompt recognition is essential to prevent permanent sequelae. An 8-year-old boy, with a complex past medical history including prior dystonic reactions, presented with acute dystonia and subsequent priapism following inadvertent administration of Aripiprazole. The erection persisted for approximately five hours, partially responsive to Diphenhydramine and Benztropine. Urologic evaluation confirmed ischemic priapism. Conservative management was successful, and no surgical intervention was needed. Doppler ultrasound of the penis showed normal flow without thrombosis. The patient remained clinically stable, experiencing only brief, intermittent episodes of erection, each of which resolved with conservative…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
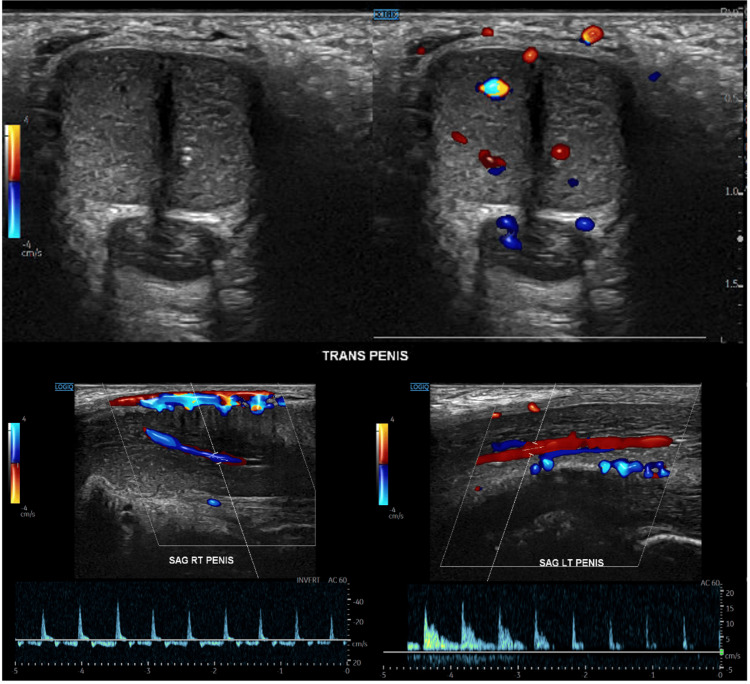 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSexual function and dysfunction studies · Urinary Bladder and Prostate Research · Hormonal and reproductive studies
Introduction
Priapism is an uncommon urological emergency in children, most often associated with sickle cell disease and other hematologic disorders [1-5]. In patients without such conditions, drug-induced priapism is a leading cause, although it remains rare. Several psychotropic agents have been implicated, including risperidone, quetiapine, lithium, atomoxetine, and oxcarbazepine.
Aripiprazole, a third-generation atypical antipsychotic, is widely prescribed in pediatric psychiatry because it is generally well tolerated and carries a lower risk of weight gain and metabolic disturbances compared to other antipsychotics [6]. Nonetheless, rare adverse effects, such as priapism, have been documented. While adult cases are reported, pediatric cases remain exceedingly scarce [7].
This report describes an unusual case of aripiprazole-induced priapism in a child with a complex medical history, highlighting the importance of vigilance, early recognition, and adherence to standard management guidelines.
Case presentation
An 8-year-old boy with a history of attention-deficit/hyperactivity disorder, oppositional defiant disorder, dextro-transposition of the great arteries (status post arterial switch), gastrostomy dependence, and bilateral vocal cord and diaphragmatic paralysis was admitted with acute dystonic reactions and simultaneous onset of priapism following inadvertent re-administration of aripiprazole by his caregiver.
Medication history: Aripiprazole had been initiated several months earlier for behavioral regulation but was discontinued after the patient developed extrapyramidal side effects. No recent dose changes had been made, and no other medications were added or withdrawn during this period. Clonidine, previously prescribed for sleep disturbances, had been withheld and was restarted during hospitalization.
At presentation, the patient exhibited dystonic movements together with a painful, rigid penile erection. The priapism persisted for approximately five hours. Diphenhydramine provided only transient relief, and benztropine was ineffective. Lorazepam was administered for sedation.
Physical examination showed a rigid, tender, non-pulsatile penis. Penile Doppler ultrasonography demonstrated preserved arterial and venous flow without thrombosis, findings that seemed inconsistent with the clinical impression (Figure 1). However, based on the painful, prolonged rigidity, the episode was diagnosed as ischemic priapism, likely a partial or stuttering variant, reconciling the Doppler findings with the clinical scenario.
Doppler evaluationPenile Doppler ultrasonography demonstrated preserved arterial and venous blood flow without evidence of thrombotic complications or vascular compromise.
Management was conservative, consisting of sedation, cold compresses, and discontinuation of aripiprazole. Pediatric urology consultation confirmed no immediate need for surgical intervention. The patient gradually improved, and clonidine was reintroduced. Following resolution of the acute event, only brief, self-limited erections (<15 minutes) occurred. Laboratory investigations (CBC, CMP, creatine kinase) were normal throughout.
Discussion
Ischemic priapism results from impaired venous drainage and subsequent hypoxia within the corpora cavernosa [3,8,9]. In children without hematologic disorders, drug-induced priapism is a predominant cause. Aripiprazole-induced priapism is estimated to occur in approximately 1 in 10,000 adults, but pediatric cases remain rare [7,10].
The pathophysiology is incompletely understood. Proposed mechanisms include alpha-adrenergic antagonism and dopaminergic modulation, both of which may disturb vascular tone and detumescence [11-13]. In this case, the close temporal relationship between accidental re-exposure to aripiprazole and the simultaneous onset of dystonia and priapism strongly supports a causal role [14].
The discrepancy between clinical ischemia and Doppler findings emphasizes the complexity of pediatric cases. The episode was interpreted as a stuttering or partial ischemic variant, a scenario where tissue hypoxia occurs despite preserved arterial inflow.
According to the American Urological Association (AUA) and European Association of Urology (EAU) guidelines, ischemic priapism requires urgent treatment to prevent long-term erectile dysfunction [3,8,15]. First-line interventions include aspiration of corporal blood, saline irrigation, and intracavernosal phenylephrine. Surgical shunting is reserved for refractory cases. In this patient, conservative therapy was effective, but clinicians must remain prepared to escalate promptly if symptoms persist. Expert consensus reports, such as the AFUD Thought Leader Panel, also highlight the need for timely intervention to preserve erectile function [16,17,18].
Drug-induced priapism in children has been reported with multiple psychotropics, including stimulants and atomoxetine [16]. Although aripiprazole is generally considered to have a more favorable metabolic and prolactin-related safety profile compared to other antipsychotics [6,17], this case demonstrates that even agents with relatively low risk can rarely cause serious adverse effects such as priapism. Few published reports involve aripiprazole specifically in pediatrics, underscoring the rarity of this event. Moreover, many reports lack detailed dosing or follow-up data, limiting generalizability [18]. This case contributes by documenting the temporal relationship, detailed clinical course, and follow-up in a medically complex child.
Lessons learned by this case include:
(i) Thorough medication history, including previous adverse reactions and recent dose adjustments, is essential. (ii) Clinicians must maintain a high index of suspicion for priapism in children presenting with genitourinary complaints during psychotropic treatment. (iii) Early urologic consultation and close monitoring are critical. (iv) Conservative management may suffice in selected cases, but adherence to standardized protocols is mandatory when ischemia persists.
Conclusions
This case illustrates that aripiprazole, though widely considered safe in pediatric populations, can precipitate priapism, even in patients without hematologic risk factors.
Given the single-patient nature of this report, management recommendations cannot be generalized. However, such reports enhance pharmacovigilance and increase clinician preparedness for rare but potentially serious drug reactions in children.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Priapism associated with antipsychotics: role of alpha 1 adrenoceptor affinity J Clin Psychopharmacol Andersohn F Schmedt N Weinmann S Willich SN Garbe E 68713020102007565110.1097/JCP.0b 013e 3181 c 8273 d · doi ↗ · pubmed ↗
- 2Priapism, its incidence and seasonal distribution in Finland Scand J Urol Nephrol Kulmala RV Lehtonen TA Tammela TL 9396291995761805410.3109/00365599509180545 · doi ↗ · pubmed ↗
- 3American Urological Association guideline on the management of priapism J Urol Montague DK Jarow J Broderick GA 1318132417020031450175610.1097/01.ju.0000087608.07371.ca · doi ↗ · pubmed ↗
- 4Priapism associated with oxcarbazepine, aripiprazole, and lithium J Am Acad Child Adolesc Psychiatry Negin B Murphy TK 1223122444200510.1097/01.chi.0000183496.44266.bd 16292111 · doi ↗ · pubmed ↗
- 5Priapism impact profile questionnaire: development and initial validation Urology Burnett AL Anele UA Derogatis LR 137613818520152586383110.1016/j.urology.2015.02.025PMC 4480192 · doi ↗ · pubmed ↗
- 6Tolerability and pharmacokinetics of aripiprazole in children and adolescents with psychiatric disorders: an open-label, dose-escalation study J Clin Psychopharmacol Findling RL Kauffman RE Sallee FR 4414462820081862627210.1097/JCP.0b 013e 31817 dd 520 · doi ↗ · pubmed ↗
- 7Priapism associated with atypical antipsychotic medications: a review Int Clin Psychopharmacol Sood S James W Bailon MJ 9172320081809050310.1097/YIC.0b 013e 3282 f 1c 1ef · doi ↗ · pubmed ↗
- 8European Association of Urology guidelines on priapism Eur Urol Salonia A Eardley I Giuliano F 4804896520142431482710.1016/j.eururo.2013.11.008 · doi ↗ · pubmed ↗