Association between self-reported gender-based discrimination and maternal mortality rates: results of an ecological multi-level analysis across nine countries in Sub-Saharan Africa
Clara Orduhan, Ruth Waitzberg, Manuela De Allegri, Bona Chitah, Jean-Paul Dossou, Charlestine Bob Elwange, Adama Faye, Sharon Fonn, Christabel Kambala, Shafiu Mohammed, Hamidou Niangaly, Chenjerai Sisimayi, Wilm Quentin

TL;DR
This study finds that higher rates of self-reported gender-based discrimination are linked to higher maternal mortality in nine Sub-Saharan African countries.
Contribution
The study provides new evidence of a direct association between gender-based discrimination and maternal mortality in Sub-Saharan Africa.
Findings
A 1% increase in gender-based discrimination was linked to nearly two more maternal deaths per 100,000 live births.
The association remained strong after adjusting for region-level factors but not after including country-level factors.
The study highlights the need for further research to understand the causal pathways between discrimination and maternal mortality.
Abstract
Sub-Saharan Africa suffers from the highest maternal mortality ratio (MMR) in the world, with 542 deaths per 100,000 live births in 2017, relative to a global ratio of 211. Reducing gender-based discrimination (GBD) and increasing the empowerment of women and girls have recently been recognized as prerequisites for improving maternal health. Previous studies have shown GBD to result in low utilization of maternal health services and poorer quality of care. However, limited research is available on the relationship between GBD and maternal mortality in Sub-Saharan Africa (SSA). Therefore, the objective of this study was to assess whether GBD is associated with maternal mortality in SSA. We investigated the association between self-reported GBD and maternal mortality in an ecological study. We used data from two surveys: the Demographic and Health Surveys (DHS) and the Afrobarometer.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
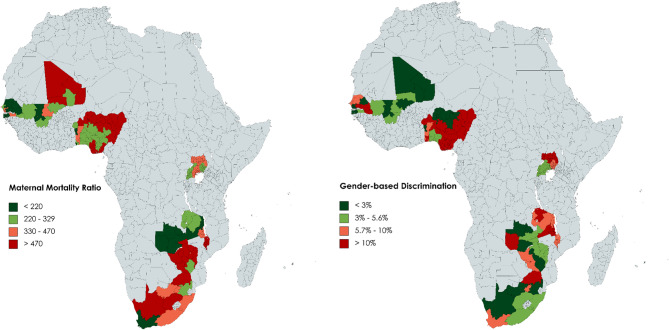 Figure 1
Figure 1- —Technische Universität Berlin (3136)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health · Global Health Care Issues · Demographic Trends and Gender Preferences
Background
Maternal mortality has declined substantially in the recent past, yet Sub-Saharan Africa (SSA) continues to suffer from the highest maternal mortality ratio (MMR) in the world, with 542 deaths per 100,000 live births in 2017, relative to the global MMR of 211 [1]. In 2015, the United Nations General Assembly adopted the 17 Sustainable Development Goals (SDGs). Target 3·1 of the SDGs calls for a reduction of the global MMR to less than 70 per 100,000 live births by 2030 [2]. The main causes for maternal deaths are obstructed labor, hemorrhage, eclampsia, sepsis, and unsafe abortions [3, 4]. Most of these deaths could be avoided if all women had timely access to high quality maternal health care services [5].
Traditionally, strategies to reduce maternal deaths have focused on improving access to high quality reproductive health services. The Millennium Development Goals for instance, through target 5·B sought to improve access to reproductive health services [6]. However, more recently, reducing gender inequality and increasing the empowerment of women and girls have been recognized as prerequisites for improving maternal health [7]. Gender inequality is the systemic disparity in rights, opportunities, and outcomes between genders. Gender inequality is often driven and perpetuated by discrimination, particularly gender-based discrimination [8, 9].
In this work, we conceptualize Gender-based discrimination (GBD) as any unequal treatment that occurs because of a person’s gender [10, 11]. GBD can either hinder women’s demand for health care or health workers’ supply of care. Some studies have shown GBD to be related to low utilization of maternal health services [12]. For example, due to culturally entrenched and religiously accepted gender roles and norms, women tend to have lower decision-making power, with negative effects on their ability to access maternal health care services [13], notably when the husband denies permission [5]. Similarly, intimate partner violence can discourage women from seeking family planning services or antenatal care [14]. Discrimination also takes place at health facilities, where women may be denied family planning services if they come alone or if they are unmarried [15]. Male-dominated intra-household resource allocation leads to a lack of resources for women to receive family planning services [13, 16]. More generally, GBD and unequal power balance between men and women are some of the root causes of gender inequities in physical and mental health outcomes, and among the most influential of the social determinants of health [17–20]. GBD also permeates content and process of health research, participation in medical trials, and therefore also medical treatment. Finally, gender imbalances exist among health providers, where women are less present and receive lower payment [21, 22]. The first step to mitigating these unwanted behaviors is increasing awareness of GBD among women.
The Partnership for Maternal, Newborn, and Child Health (PMNCH) explicitly recognizes the need to tackle gender inequality operating at the broader societal level as a means of improving maternal health outcomes [23]. Many studies have assessed the relation between GBD and maternal health care outcomes using different measures and definitions of GBD, such as male-dominated intra-household resource allocation, women’s status, economic dependency, gender inequality, and gender gap [13, 15, 16, 22, 24–30]. Yet, to our knowledge, previous research has not attempted to quantify the relationship between self-reported GBD and maternal mortality in SSA. To address this research gap, we aim to directly investigate whether higher levels of perceived GBD are associated with higher levels of maternal deaths across several SSA countries. More specifically, our study has the following objectives: (1) to map the level of self-reported GBD and MMR in different African countries, (2) to examine the association between self-reported GBD and MMR at the regional level, and (3) to explore the relevance of other regional and country-level factors in explaining MMR.
Methods
Study design and data sources
This is an ecological study, with a cross-sectional design. We used data from two main periodic surveys conducted by networks of researchers: Demographic and Health Surveys (DHS) and Afrobarometer.
DHS are large-scale household surveys with an average sample size of 5,000 to 30,000 households, conducted across many low- and middle-income countries (LMICs) using standardized questionnaires [31]. Afrobarometer surveys measure social, political, and economic conditions in more than 30 African countries [32]. Ordinarily, these are measured with the help of face-to-face interviews in applicable local dialects with each survey round containing randomly selected samples of 1,200 or 2,400 people in each country. Working with trained and skilled national partners ensures the quality of data collection [32].
We used data from the DHS for our outcome (dependent) variable, i.e., MMR. Data from Afrobarometer was used for our main independent variable, i.e., GBD. Since DHS phase VII, the inclusion of two questions to exclude deaths due to an act of violence or an accident have improved maternal mortality estimates [33]. Therefore, this paper utilized data from DHS phase VII, conducted between 2015 and 2018 (see Appendix 1). From round seven (R7), Afrobarometer started to include a question to explore self-reported GBD of women [34]. Therefore, we used data from Afrobarometer R7, conducted between 2016 and 2018. We decided against using the DHS gender-based violence module to construct our GBD variable since we aimed to investigate and capture GBD in general, not only in its overt manifestation as violence [31].
Both data sources provide geocoded data at the region-level. We picked all SSA countries for which we had data from DHS and Afrobarometer for the mentioned time periods and matched the datasets at the corresponding geocoded regional level. That led to the following country selection: Benin, Malawi, Mali, Nigeria, Senegal, South Africa, Uganda, Zambia, and Zimbabwe. We then modeled the analysis as a random intercept two-level model to assess further information at the region- and at the country-level.
Variables and measurement
Outcome variable
Our outcome variable of interest is the MMR, which captures the number of maternal deaths per 100,000 live births [35]. To estimate maternal mortality, we built a variable from DHS using the sibling history approach [36]. Using a catalogue of detailed questions, this method asks women to name and count their sisters who died from maternal causes [36]. We coded this variable as continuous, differing by region of residence, and calculated it as follows [36]:
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:\mathrm{MMR}=\frac{\mathrm{MMRate}}{\mathrm{FR}}\:\mathrm x\:\text{100,000},$$\end{document} \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:\mathrm{MMRate}=\frac{\mathrm{Number}\:\mathrm{of}\:\mathrm{maternal}\:\mathrm{deaths}}{\mathrm{Womenyears}\:\mathrm{of}\:\mathrm{exposure}\:\mathrm{of}\:\mathrm{sisters}\:}\mathrm x\text{1,000},$$\end{document} \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:\mathrm{FR}=\frac{\mathrm{Number}\:\mathrm{of}\:\mathrm{births}}{\mathrm{Womenyears}\:\mathrm{of}\:\mathrm{exposure}\:\mathrm{of}\:\mathrm{female}\:\mathrm{respondents}}\mathrm x\text{1,000},$$\end{document}where MMRate is the maternal mortality rate, and FR is the fertility rate. We used the DHS guide to compute and estimate all relevant statistics with respect to DHS-7. We calculated the number of births and the number of maternal deaths for a period of zero to six years preceding the survey [37]. Women-years of exposure are the sum of women living in a given preceding time period, in our case zero to six years [36]. We generated the number of births out of the DHS Birth’s Recode and the number of maternal deaths as well as the women-years of exposure out of the DHS Individual Recode [38].
Exposure variable
Our main independent (exposure) variable of interest is the proportion of women who reported having experienced gender-based discrimination in the past year. Afrobarometer asks: “In the past year, how often, if at all, have you personally been discriminated against or harassed based on […] your gender?” [34] with answer categories distinguishing never, once or twice, several times, or many times. We transformed this categorical variable into a binary variable (0 = never/once or twice; 1 = several or many times.) and then used the proportion of women who reported having experienced GBD several or many times out of the full sample of women interviewed in a given region as a continuous variable.
Control covariates
At both the region- and the country-levels, we controlled for several covariates that have been shown to be associated with maternal mortality in previous analyses [39–46]. At the region-level we integrated the proportion of women who (1) have any school education, (2) are assigned with a high lived poverty index (LPI), which measures how frequently a person goes without basic needs such as food, water, or medicine [47], (3) have difficulties in obtaining medical treatments in general (not only relating to maternity), (4) never had to pay a bribe to obtain medical treatments, and who (5) have access to a piped water system close to their place of residence. At the country-level, we controlled for the (6) UNAIDS’ estimated HIV prevalence among the total population of ages 15–49, (7) the WHO’s calculated current health expenditure per capita in US$, and (8) the adolescents’ fertility rate measured by the United Nations Population Division, which means the average number of births per 1,000 women ages 15–19 (see Tables 1 and 2). We controlled all independent variables for multicollinearity and found that correlation values are consistently below ± 0·73 (>95% are below ± 0·7) (see Appendix 2). We did not control for median age or fertility rates, as these variables are captured by the outcome (dependent) variable, MMR.
Table 1. Variables, definitions, measurements, and sourcesVariableDefinitionMeasurementData source and DateOutcome VariableMMRNumber of maternal deaths per 100,000 live births during the six years preceding the survey per regionContinuous VariableDHS-VII, 2015-2018Individual and Birth Recode[48]Exposure Variable (Main Independent Variable)Self-reported experiencing GBDProportion of women reporting experiencing gender-based discrimination in the year preceding the survey per regionContinuous Variable, Unit of Measure in %Afrobarometer R7, 2016–2018[34]Covariates region-levelSchool educationProportion of women who have any kind of school educationContinuous Variable, Unit of Measure in %DHS-VII, 2015-2018Individual and Birth Recode[48]High LPIProportion of women who are assigned with a high lived poverty indexContinuous Variable, Unit of Measure in %Afrobarometer R7, 2016–2018[34]Difficulties in obtaining medical treatmentProportion of women who have difficulties in obtaining medical treatmentsContinuous Variable, Unit of Measure in %Afrobarometer R7, 2016–2018[34]Never pay bribes for medical treatmentProportion of women who never had to pay a bribe to obtain medical treatmentContinuous Variable, Unit of Measure in %Afrobarometer R7, 2016–2018[34]Access to waterProportion of women who have access to a piped water systemContinuous Variable, Unit of Measure in %Afrobarometer R7, 2016–2018[34]Covariates country-levelHIV PrevalenceHIV Prevalence among the population of ages 15–49Continuous Variable, Unit of Measure in %UNAIDS, 2020[49]Health ExpenditureCurrent health expenditure per capitaContinuous Variable, Unit of Measure in US$WHO, 2018[50]Adolescents’ Fertility RateAverage number of births per 1,000 women ages 15–19Continuous Variable, Unit of Measure in %UNPD, 2019[51]
Analytical approach
To generate an initial overview, we first mapped the levels of self-reported GBD and MMR in the selected 78 regions across the nine countries at a region-level. We classified four subgroups for each of the two continuous variables, from low, over medium-low, and medium-high, to high levels. For self-reported GBD the subgroups range from ‘<3%’, over ‘3–5·6%’, ‘5·7–10%’ to ‘>10%’. We formed these groups tailored to the distribution of the values, so that every group would contain approximately the same number of regions. We contrasted both variables with the help of a figure showing the levels in colors (see Fig. 1). For instance, in Mopti, Mali, we found, based on the Afrobarometer data, that 1·5% of the women reported experiencing GBD. Mopti belongs to the lowest level of < 3% reported GBD and that is why Mopti is colored in dark green in Fig. 1.
To examine the association between MMR and self-reported GBD and to assess the relevance of other region- and country-level factors in explaining MMR, we conducted a random intercept two-level model using the continuous variable measures in a linear regression. Level 1 is the region of residence, which is nested in level 2, the country. For this analysis, we used data from 160,275 women from the DHS survey and from 5,928 women from the Afrobarometer survey, living in \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{n}_{i}=78\:\text{r}\text{e}\text{g}\text{i}\text{o}\text{n}\text{s}$$\end{document} (level 1), nested in \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{n}_{j}=9\:\text{c}\text{o}\text{u}\text{n}\text{t}\text{r}\text{i}\text{e}\text{s}$$\end{document} (level 2). Since this in an ecological analysis, the model worked with the regional proportion of experienced GBD (based on the Afrobarometer), and the data were merged at the regional level – not at the level of individual cases. Choosing a random-intercept model, we interpreted the slope, i.e., the coefficients of the independent variables, as fixed across all 78 regions. On the other hand, the intercept is random across all 78 regions due to region- and country-specific residuals. Our analysis consists of four different models, each adjusted for more covariates. First, we conducted the Null Model, which only concentrates on our outcome variable and gives out the overall mean of the MMR across all regions. Then we integrated step by step our main independent variable of interest (Model 1), all region-level covariates (Model 2), and all country-level covariates (Model 3). By adjusting the model for independent variables, the model produces coefficients that show the association between the independent variables and the MMR, and show the independent association of self-reported GBD with MMR. We conducted all analyses of our random intercept two-level model in the statistics software SPSS (PASW Statistics 18.0). The equation of the full model (Model 3) is:
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\begin{aligned}\:{\mathrm y}_{\mathrm{ij}}&={\mathrm\beta\:}_0+{\mathrm\beta\:}_1{\mathrm x}_{1\mathrm{ij}}+{\mathrm\beta\:}_2{\mathrm x}_{2\mathrm{ij}}+{\mathrm\beta\:}_3{\mathrm x}_{3\mathrm{ij}}\\&+{\mathrm\beta\:}_4{\mathrm x}_{4\mathrm{ij}}+{\mathrm\beta\:}_5{\mathrm x}_{5\mathrm{ij}}+{\mathrm\beta\:}_6{\mathrm x}_{6\mathrm{ij}}+{\mathrm\beta}_7{\mathrm x}_7\mathrm j\\&+{\mathrm\beta}_8{\mathrm x}_8\mathrm j+{\mathrm\beta}_9{\mathrm x}_9\mathrm j+{\mathrm u}_{\mathrm j}+{\mathrm e}_{\mathrm i}\mathrm j,\end{aligned}$$\end{document}where \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{y}_{ij}$$\end{document} represents the MMR outcome variable for region \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:i$$\end{document} in country \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:j$$\end{document} . Every \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:x$$\end{document} represents a predictor variable, \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{\beta\:}_{0}$$\end{document} is the overall mean of the MMR across all 78 regions, \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{\beta\:}_{1-9}$$\end{document} are the described coefficients or fixed effects of the predictor variables on the MMR, and \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{e}_{ij}$$\end{document} and \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\:{u}_{j}$$\end{document} are the region- and country-specific residuals. Besides the estimates of fixed parameters as well as individual residuals, each model produces the Akaike’s Information Criterion (AIC). The comparison of the AIC for each model shows whether the inclusion of the covariates improves the fit of the model or not, i.e., if the AIC is smaller than the AIC of the model conducted before, it is a fit improvement [52]. Click or tap here to enter text.
Results
Table 2 describes the full sample population and distribution of the answers by variable used in the regression models. The majority of women (93%) did not experience gender discrimination in the last year, although there is high variance across countries and sub-regions (Fig. 1). Most women have no school education (72%) and don’t have piped water at home (54%).
Table 2. Descriptive statistics of regional independent variablesStudy Population(n = 160,275 [DHS]/5,928 [Afrobarometer)%Experienced gender discrimination – total5925100Yes4277No548993Have school education – total160,275100Yes44,89328No115,38272High Lived Poverty Index (LPI) – total5884100Yes102417No486083Obtaining medical treatment – total5927100Difficult177230Easy208035No contact206935Having to pay a bribe to obtain medical treatment – total5927100Never345558At least once3977No contact206935Have a piped water system in primary sampling unit/enumeration area – total5928100Yes267445No322554 *Sum of counts for each variable may not add up to total due to missing data
The two maps in Fig. 1 provide an overview of the levels of MMR and self-reported GBD across regions. They show that the reported experience of GBD is highest in Benin, Atacora (24·7%), Senegal, Tambacounda (23·0%), and Zambia, Northern region (18·2%). The highest MMRs, i.e., the number of maternal deaths per 100,000 live births, are in South Africa, Northern Cape (2079), Mali, Kidal (1992), and Mali, Toumbouctou (1273) (see Appendices 3, 4). Notably, large variations of both GBD and MMR were depicted among selected regions at in-country level in SSA.
Fig. 1. Mapped levels of MMR and reported GBD per region
Pooling data across 78 regions, located in nine countries, the Null Model generates an overall estimate of 417 (95% CI 310–523), indicating 417 maternal deaths per 100,000 live births (see Table 3). In Model 1, adjusted only for the main independent variable of interest, the coefficient of 0·88 (95% CI 0·65 − 1·12) indicates that a 1% increase in the proportion of women reporting GBD results in nearly one more maternal death per 100,000 live births. Adjusting for region-level covariates (Model 2), we observe an even more pronounced association between self-reported GBD and MMR, with the coefficient standing at 1·95 (95% CI 1·71 − 2·19), and this does not change with the inclusion of country-level covariates (Model 3). In the full model (Model 3), coefficients of most covariates point in the expected directions, which are positive for LPI (4·59 (95% CI 4·45 − 4·72)), difficulty in obtaining medical treatment (0·42 (95% CI 0·26 − 0·58)), HIV prevalence (38·15 (95% CI 13·67 − 62·62)), and adolescents’ fertility rate (0·92 (95% CI −2·8 − 4·64)); and negative for school education (−6·05 (95% CI −6·24-(−5·96))), never paying bribes for medical treatments (−1·74 (95% CI −1·88-(−1·58))), and health expenditure (−0·24 (95% CI −1·36 − 0·89)). However, the coefficient of access to piped water is positively associated with higher MMR (1·59 (95% CI 1·53 − 1·65)).
Looking at the AIC, the inclusion of the regional covariates improved the fit of Model 2 compared with the Null Model. By adding the country-level covariates, the AIC remained nearly the same (see Table 3).
Table 3. Results of the two-level linear regression analysisNull ModelModel 1 - adjusted for main independent variableModel 2- adjusted for covariates at region-levelModel 3 - adjusted for covariatesat country-levelFixed Effects95% CIFixed Effects95% CIFixed Effects95% CIFixed Effects95% CIMMR 417* (310; 523) 410* (303; 517) 781* (597; 965) 451* (14; 889)Reported GBD 0.88* (0.65; 1.12) 1.95* (1.71; 2.19) 1.95* (1.71; 2.19)School education −6.05* (−6.14; −5.95) −6.05* (−6.24; −5.96)High LPI 4.59* (4.45; 4.72) 4.59* (4.45; 4.72)Difficulty in obtaining medical treatment 0.42* (0.26; 0,58) 0.42* (0.26; 0.58)Never pay bribes for medical treatment −1.73* (−1.88; −1.58) −1.74* (−1.88; −1.58)Access to water 1.59* (1.53; 1,65) 1.59* (1.53; 1.65)HIV Prevalence 38.15* (13.67; 62.62)Health Expenditure −0.24 (−1.36; 0.89)Adolescents’ Fertility Rate 0.92 (−2.8; 4.64)Akaike’s information criterion (AIC); % change to null model2217826,7712217774,238; −0.002%2187952,673; −1.35%2187947,210; −1.35% *statistically significant at α = 0.05
Discussion
This is the first study to investigate the association between the proportion of women reporting GBD and MMR across several countries in SSA. Since data on obstetrics and MMR is usually incomplete or not routinely collected [53, 54], our work used alternative data sources based on surveys to monitor MMR and GBD. In addition, we built on standardized data collected across countries and regions, allowing for cross-country comparison.
We found a significant positive association between self-reported GBD and the number of maternal deaths, with nearly two more deaths per 1% increase in the proportion of women reporting being discriminated. There was large variation in both self-reported GBD and MMR across regions within countries, which requires a better understanding of the underlying factors.
Several previous studies have focused on GBD in the context of specific aspects of maternal health, such as the association between gender inequality and low utilization of maternal health services [12, 24, 26]. In fact, GBD is increasingly being recognized as affecting women’s health, by shaping resource allocation, both within and outside the household, and limiting access to health services [55, 56]. However, our analysis is the first to show that self-reported GBD is independently associated with MMR. In our model, the effect size of self-reported GBD was similar or larger to that of many factors that are well-known for their association with maternal mortality, such as having access to water, never having paid bribes, or the level of national health expenditures, even if it was considerably smaller than the effect sizes of education, or general poverty [39, 40, 45].
Our findings expand the literature by identifying GBD as an important risk factor to MMR that is related to the society where women live. More well known individual level risk factors include women’s characteristics such as age (younger than 20 or older than 35), weight (under or over), nutritional status, anemia, comorbidities, and low education; pregnancy characteristics such as number of pregnancies, having twins, pregnancy complications, and size of fetus; characteristics of the event of the delivery such as obstructed birth, Caesarean mode of delivery, the absence of a health professional at birth; and low access to maternal care such as antenatal care or postpartum care [53, 57–61]. However, the experience of GBD affects all women in a given region, and therefore has a pervasive effect on women’s health. Other studies found that low education of the partner is also a risk factor to MMR [61], yet it is still an individual level risk factor. Our study adds a collective risk factor that affects a whole society, which in the context of LMICs goes beyond the lack of resources or poverty.
Several studies have shown a negative association between GBD and women’s health beyond MMR. GBD was found to exacerbate the burden of chronic diseases, as it increased substantially the risk of having at least one physical health condition [62]. Perceived GBD negatively affects not only physical but also mental health and wellbeing [63, 64], while reducing access to women’s health care [65]. Even if women might have access to health care, GBD can prevent women from seeking antenatal and maternal health services due to gender inequalities in the quality of treatments [15]. GBD is expressed by women’s lower autonomy [66] and is associated with poorer mental and physical health and higher mortality not only for women, but for their children too [67]. While perceived GBD is more reported among women with high education or high SES, this group is also more resilient to the negative spillover effects of GBD on health [63, 68].
Strengths and limitations
The strengths of our paper are that we showed a positive association between GBD and maternal mortality based on standardized data collected across countries and regions. While there is evidence on the negative association of GBD and women’s health, the quality of these studies is not high [67]. Our work fills this gap by providing high-quality evidence on the increased burden of GBD on maternal health, specifically on MMR. Moreover, due to the usage of data collected across regions, our findings allow for cross-country comparison.
Our study has several limitations. First, our main outcome variable of regional MMR suffers from the problem that DHS does not ask for the residence of the women who died but instead assigns the maternal deaths to the regions the interviewed sisters live in, although the place of residence of the sisters (the one who died and the one who is interviewed) is not necessarily the same [36]. Also, some of our DHS estimates for the MMR differ significantly from estimates made by the WHO, UNICEF or other data sources [75]. That is why, there might be discrepancies between the MMR values used for our analysis and preceding findings made by other researchers. For instance, the overall MMR in South Africa, i.e., 532, is outstandingly high in our model compared to other data sources and estimation methods (see Appendix 4) [76]. More realistic estimates of MMR than those made in this analysis could lead to different correlations between MMR and self-reported GBD. Second, our main independent variable is a subjective and likely imprecise measure of experiencing GBD because the Afrobarometer asks only a single question to explore a woman’s experience with GBD [34]. As the understanding of GBD varies across countries, regions or individuals, our self-reported GBD variable reflects subjective realities, awareness, cultural norms and expectations, with minorities underestimating its frequency [77]. While there are indicators that measure gender equality in different fields such as education, health, labor market and political life [77–83], no indicator directly measures gender discrimination. The prevalence, or an ‘objective’ magnitude of GBD remains unknown. In addition, GBD has many dimensions, and while the Afrobarometer self-reported GBD question is broad and attempts to capture the overall experience of GBD, it does not indicate the source or context of GBD. For example, if it is domestic abuse or economic dependency that hinders women’s demand for health care, or GBD at the supply side, resulting in poor quality of care. More specific questions about the various dimensions of GBD could render refined results to support policy that tackles GBD. However, to our knowledge, there is no cross-country survey that explores the different dimensions of GBD in SSA. Third, data was unavailable across countries for several indicators that have been previously found to be associated with maternal mortality, such as health insurance coverage, access to or the quality of maternal care, chronic diseases or comorbidities [26, 84]. This means that our model does not fully account for all factors that influence maternal mortality, even though it does control for some of the most important ones [39–46]. In addition, we did not include unmet need for family planning such as reproductive health services and use of contraceptives as a control variable because of its strong correlation with self-reported GBD [15, 42, 85]. It is important to note that as an ecological study, we found an association between proportions of women who reported having experienced GBD and the regional MMR, but we did not investigate the relationship between a single woman being exposed to discrimination and the probability of her dying due to maternal health causes. Finally, we could not rule out endogeneity, as the same set of independent variables that are responsible for self-reported GBD may also be responsible for MMR [86].
Policy implications and future research
Our study has important implications for both policy and future research. First, our findings suggest that addressing GBD could contribute both to reducing MMR and to achieving the SDGs [2]. UNICEF’s “Gender Action Plan 2022–2025” provides an example of a high-level strategy that aims to address gender equality and reduce GBD [69]. National health strategies could follow this example and incorporate measures aimed at reducing GBD – not only because of its role in explaining maternal mortality. In addition, given that disrespectful maternal health care provision at health facilities has been widely reported in SSA, targeted training of health care providers on topics such as GBD and gender-based violence could contribute to improving the situation [13, 15, 16, 70].
Second, the findings of our study and its limitations point to the importance of better understanding and measuring the different dimensions and sources of GBD. While existing research has focused on associations between single dimensions of GBD, such as male-dominated intra-household resource allocation, and maternal health care outcomes [13, 16], limited evidence is available on the multidimensional effects of GBD on maternal health. One reason for this lack of a comprehensive understanding of the effects of GBD on maternal health is that a reliable tool for measuring the multiple dimensions of GBD is currently unavailable. The development of a comprehensive standard questionnaire on GBD could potentially overcome this problem and contribute to a better assessment of GBD across different cultural and educational backgrounds.
Third, while there is a rich body of evidence on risk factors associated with maternal mortality [58, 61, 71], more research is needed that explores the causal pathways linking GBD with maternal health outcomes, including maternal mortality. These pathways may include external mechanisms, such as male- dominated decision-making spaces leading to inadequate consideration of women’s health needs in the development of national health strategies and policies; [13] or the negative impact of GBD on women’s education and financial resources, which hampers their ability to use timely and appropriate health services [13, 16, 22, 27, 30]. Pathways may also include internal mechanisms, as women could internalize the symbolic societal violence generated by GBD, and as a consequence start to under-value their lives and limit their self-efficacy to take action to prevent maternal mortality [72]. This may disempower women and affect how they perceive the value of their own lives [73, 74]. In addition, more research is needed to explore perceived GBD in healthcare settings, assessing the effects of undervaluation and different treatment of women by health providers, and its impact on MMR. Finally, more knowledge could be produced on the effects of gender imbalance of health research and treatment guidelines and MMR [19].
Conclusions
In conclusion, our study found that maternal mortality is associated with self-reported GBD even after controlling for other determinants of maternal mortality. Our findings are important because they suggest that actions and measures to address GBD could help to improve maternal health and reduce maternal mortality. Further research is needed to better understand the different dimensions and sources of GBD as well as to unravel causal pathways between GBD and maternal health outcomes. A better understanding of GBD is a prerequisite for designing effective interventions to address the different sources of GBD. Ultimately, addressing GBD is needed not only because of its detrimental effects on maternal health but also to achieve the broader societal goals of gender equality.
Supplementary Information
Supplementary material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kyei-Nimakoh M, Carolan-Olah M, Mc Cann TV. Access barriers to obstetric care at health facilities in sub-Saharan Africa-a systematic review. Syst Rev. 2017;6. 10.1186/S 13643-017-0503-X.10.1186/s 13643-017-0503-x PMC 546171528587676 · doi ↗ · pubmed ↗
- 2United Nations. Goal 5: Improve Maternal Health. United Nations Millennium Development Goals. 2021. https://www.un.org/millenniumgoals/maternal.shtml. Accessed 28 Jan 2023.
- 3Alhusen JL, Ray E, Sharps P, Bullock L. Intimate Partner Violence During Pregnancy: Maternal and Neonatal Outcomes. https://home.liebertpub.com/jwh. 2015;24:100–6. 10.1089/JWH.2014.487210.1089/jwh.2014.4872 PMC 436115725265285 · doi ↗ · pubmed ↗
- 4Pedrana L, Pamponet M, Walker R, Costa F, Rasella D. Global Health Action Scoping review: national monitoring frameworks for social determinants of health and health equity Scoping review: national monitoring frameworks for social determinants of health and health equity. 2016. 10.3402/gha.v 9.2883110.3402/gha.v 9.28831 PMC 474486826853896 · doi ↗ · pubmed ↗
- 5Borrell C, Artazcoz L, Gil-González D, Pérez G, Rohlfs I, Pérez K. Perceived sexism as a health determinant in Spain. https://home.liebertpub.com/jwh. 2010;19:741–50. 10.1089/JWH.2009.159410.1089/jwh.2009.159420350207 · doi ↗ · pubmed ↗
- 6Govender V, Penn-Kekana L. Gender biases and discrimination: a review of health care interpersonal interactions. Glob Public Health. 2008;3 SUPPL. 1:90–103. 10.1080/1744169080189220810.1080/1744169080189220819288345 · doi ↗ · pubmed ↗
- 7PMNCH. PMNCH - Partnership for Maternal, Newborn and Child Health. 2023. https://pmnch.who.int/. Accessed 29 Jan 2023.
- 8DHS Program. Demographic and Health Surveys - Data. 2023. https://dhsprogram.com/Data/. Accessed 28 Jan 2023.