Monkeypox in South Asia: a systematic review
Kinley Wangdi, Ripon Adhikary, Ziqi Liu, Sotiris Vardoulakis, Rosemary A. McFarlane, Manas Kotepui, Wenbiao Hu, Apiporn T. Suwannatrai, Tsheten Tsheten

TL;DR
This paper reviews monkeypox cases in South Asia, highlighting travel-related transmission and the need for better surveillance and diagnostics.
Contribution
The study provides a systematic review of monkeypox epidemiology and mitigation strategies in South Asia.
Findings
Most monkeypox cases in South Asia were linked to recent travel, especially to UAE and Saudi Arabia.
Common symptoms included skin lesions, fever, and lymphadenopathy, with diagnostic challenges due to co-infections.
India had the highest number of cases, and public health responses varied with limited vaccine availability.
Abstract
Monkeypox (Mpox) has emerged as a significant public health concern globally and in South Asia. Therefore, this systematic review aimed to provide a synthesis of the epidemiological pattern, clinical features, disease severity, and mitigation strategies in the region. A systematic review was conducted across four databases including PubMed, Scopus, Web of Science, and Ovid from inception to August 2024. Out of 2,430 studies, only 19 met the inclusion criteria with 111 confirmed Mpox cases. Forty percent (44) of patients were males and 45.9% (51) did not specify their sex. Young to middle-aged adults were most affected, with rare cases in a neonate. Around two-thirds (73.0%, 81) of Mpox patients were from India, followed by Pakistan (16.2%, 18) and Nigeria (resident in India) (9.9%, 11). Sixty-eight percent (76) of Mpox patients reported recent travel, particularly to UAE (27%, 21) and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
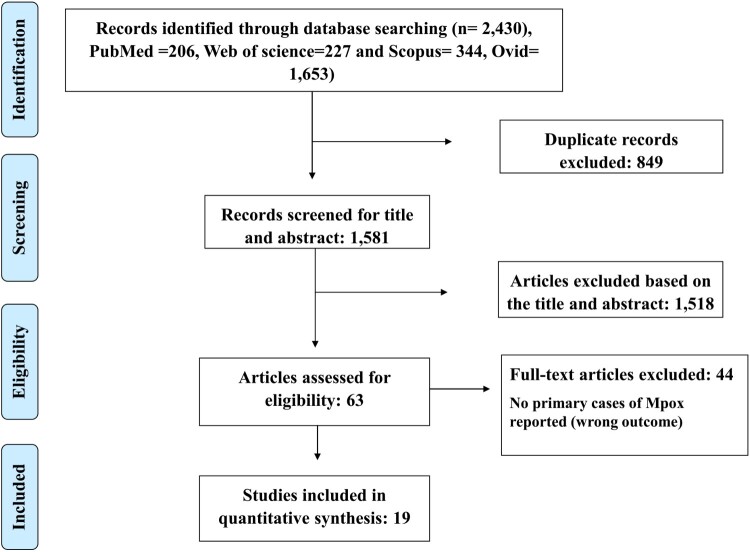 Figure 1
Figure 1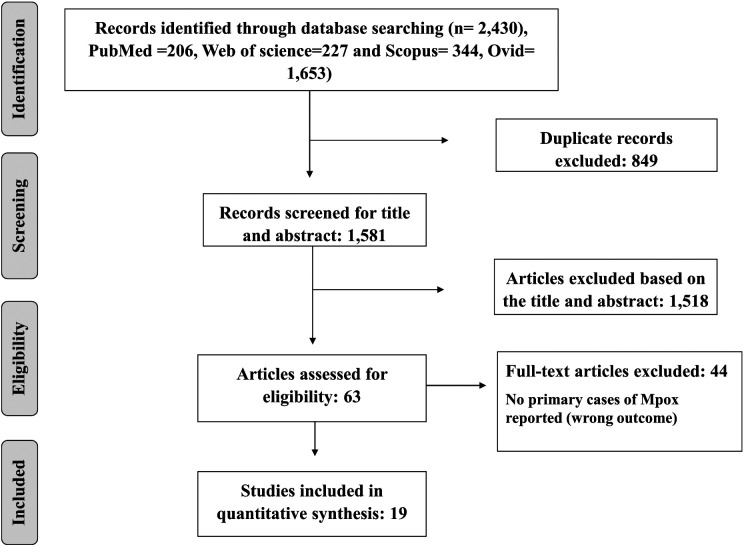 Figure 2
Figure 2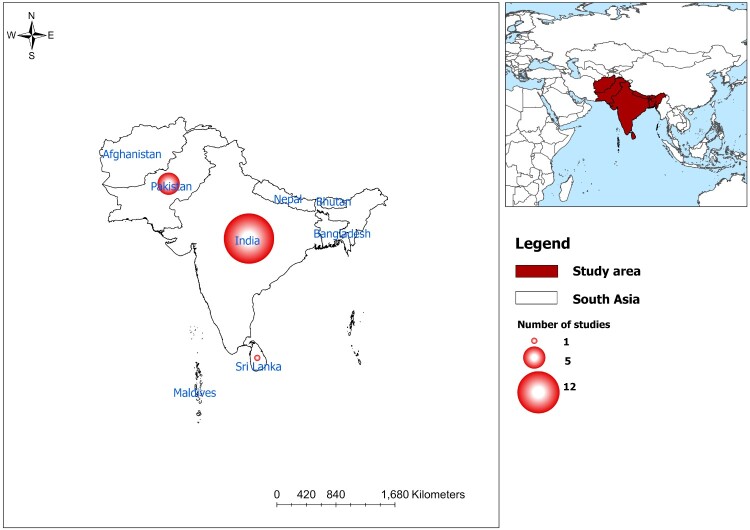 Figure 3
Figure 3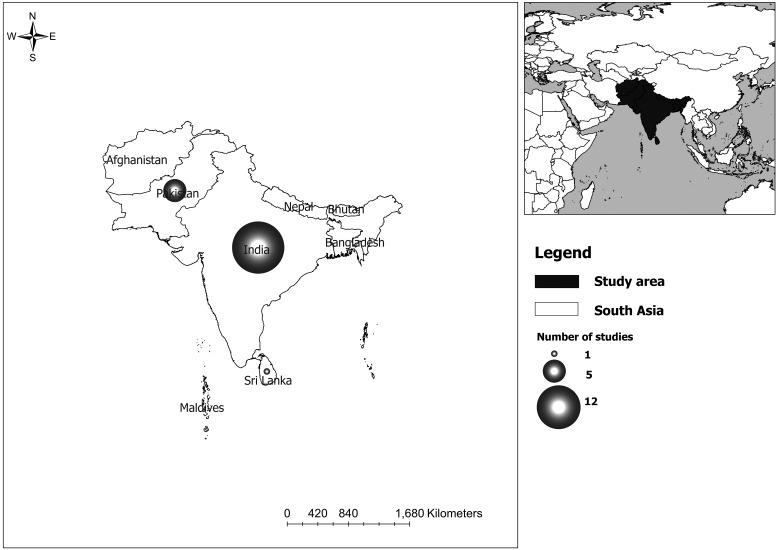 Figure 4
Figure 4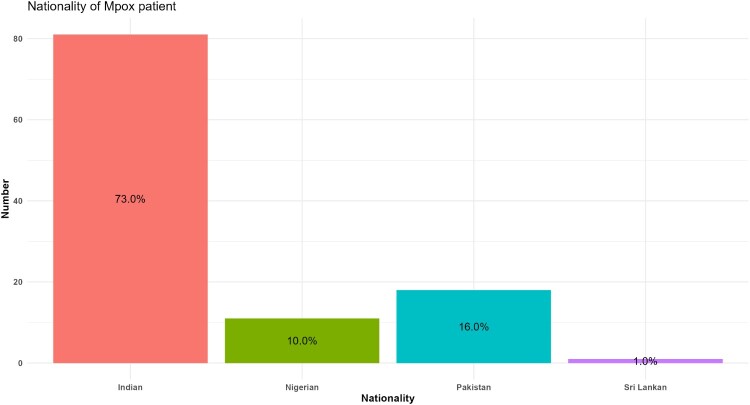 Figure 5
Figure 5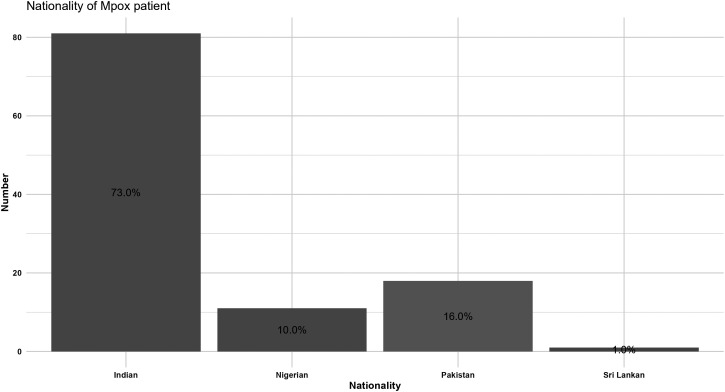 Figure 6
Figure 6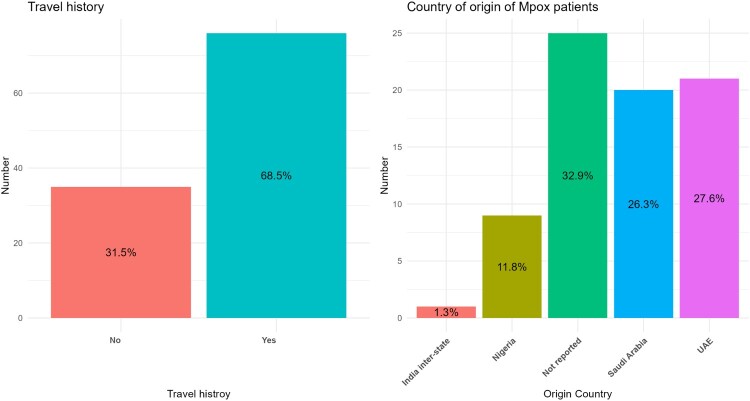 Figure 7
Figure 7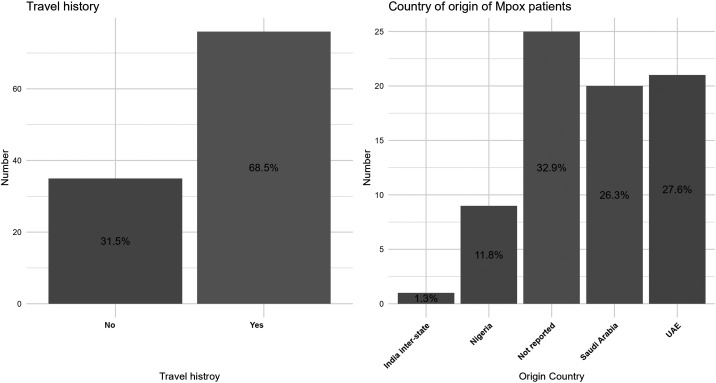 Figure 8
Figure 8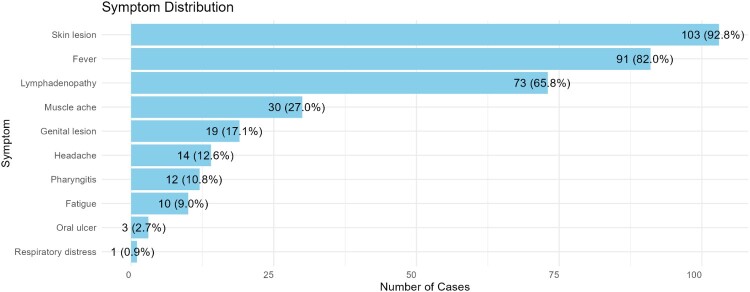 Figure 9
Figure 9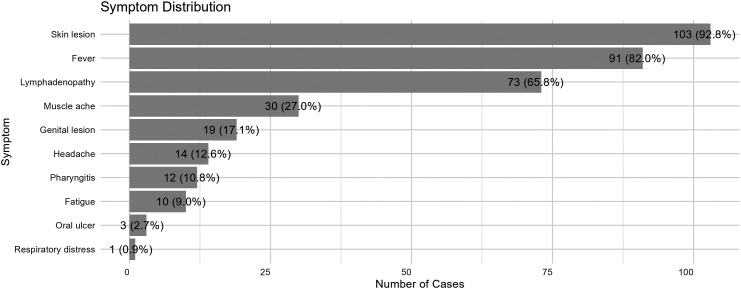 Figure 10
Figure 10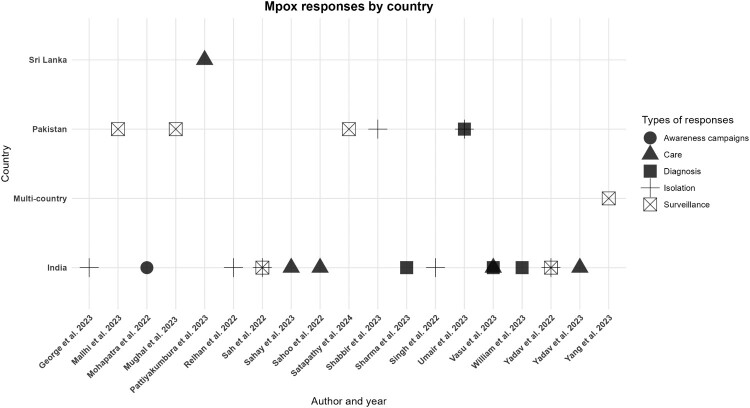 Figure 11
Figure 11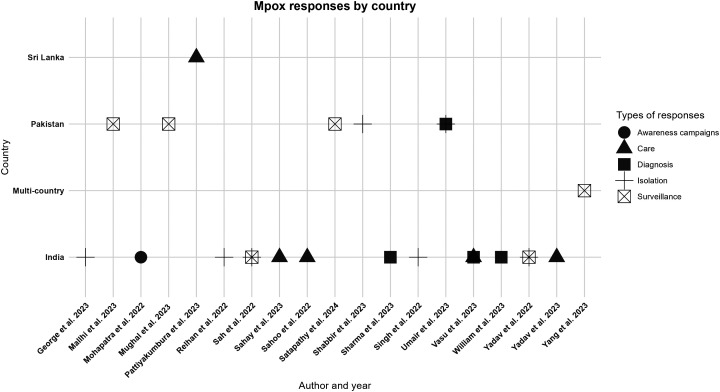 Figure 12
Figure 12- —Australian National Health and Medical Research Council
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPoxvirus research and outbreaks · Bacillus and Francisella bacterial research · Yersinia bacterium, plague, ectoparasites research
Introduction
Monkeypox is caused by the Monkeypox virus (MPXV; hereinafter referred to as Mpox), which belongs to the Orthopoxvirus genus of the Poxviridae family [1]. It was first identified at a polio research facility in Copenhagen in 1958 in cynomolgus monkeys (Macaca fascicularis), shipped from Singapore [2]. However, the first human cases were reported in Central and West Africa in the 1970s [3]. Zoonotic infection is associated with multiple wild mammals in Africa [2]. Over the years, sporadic outbreaks have been reported in non-endemic regions primarily due to human-to-human transmission. Additionally, international trade and travel have contributed to the spread of the infection, where as importation of infected animals has been rarely implicated [4]. Mpox in humans has an incubation period of 5–21 days and symptoms include fever, a vesicular – pustular eruption and lymphadenopathy [5–7]. It has an estimated mortality rate of 10.6% in Central Africa and <3.6% in West Africa [8, 9]. The primary mode of transmission from person to person is contact with infectious lesions or respiratory droplets. Transmission through seminal fluid has been reported [10, 11].
While historically confined to endemic regions in Africa, cases have now been reported in multiple non-endemic regions including Europe, America and Asia. Since the World Health Organization (WHO) declared Mpox a public health emergency on 23 July 2022 [12], 126 countries have reported cases [5]. Between January 2022 and August 2024, WHO reported over 10,000 laboratory confirmed cases and 220 deaths among confirmed cases [13]. In the WHO South-East Asia Region (SEAR), there were 959 cases and 11 deaths reported as of September 2024 [14]. India was the first country in SEAR to report Mpox, on 12 July 2022 [15]. Since then, many countries in the region have reported Mpox cases including deaths [16, 17]. The index cases of Mpox were acquired overseas with subsequent cases infected locally [14]. Despite ongoing efforts, the disease continues to spread, particularly in densely populated areas with limited healthcare resources.
South Asia has experienced a steady increase in Mpox cases, many linked to individuals returning from endemic areas. However, challenges such as delayed diagnosis, insufficient public awareness, and inadequate healthcare infrastructure have hindered timely response efforts [17]. Given the region’s high population density and interconnected travel networks, there is a pressing need for robust surveillance mechanisms to prevent further outbreaks and mitigate the disease’s impact. Understanding the epidemiology and clinical profile of Mpox in South Asia is crucial for improving case identification, optimizing treatment protocols, minimizing transmission risk, and enhancing patient outcomes [18].
As the region prepares for Mpox, there is a paucity of information regarding Mpox cases in the South Asia. This systematic review aimed to provide a comprehensive analysis of Mpox cases in South Asia by examining epidemiological trends, clinical characteristics, disease severity, and public health responses. By synthesizing available evidence, this study seeks to identify knowledge gaps, inform policy development, and supports efforts to enhance regional preparedness and outbreak response.
Methods
Search strategy
A comprehensive search strategy was developed to identify peer-reviewed studies reporting Mpox cases in South Asia including Afghanistan, Bangladesh, Bhutan, India, Maldives, Nepal, Pakistan, and Sri Lanka. The search was conducted across four major databases: PubMed, Scopus, Web of Science, and Ovid from inception to August 2024. The strategy utilized two domains: Domain 1 (D1), focused on Mpox-specific terms such as “monkeypox,” “mpox,” “monkey pox,” and “Orthopoxvirus,” and Domain 2 (D2), targeted geographic terms relevant to South Asia, including “Afghanistan,” “Bangladesh,” “Bhutan,” “India,” “Maldives,” “Nepal,” “Pakistan,” “Sri Lanka,” and “Asia.” Boolean operators were used to combine the domains (D1 AND D2), ensuring search results focused on studies linking Mpox with the South Asian region.
Search fields were restricted to titles and abstracts in PubMed, TITLE-ABS-KEY in Scopus, TS (Topic) in Web of Science, and keyword mapping (.mp) in Ovid to ensure a comprehensive and precise search. Full search strings were tailored to each database to optimize retrieval accuracy. The detailed search terms used for each database are shown in Supplementary Table 1.
Results were exported into EndNote version 20.0 (Clarivate Analytics, Philadelphia, PA, USA) for deduplication, and unique entries were imported into Rayyan for systematic review management. Studies were initially screened based on titles and abstracts. Studies selected by title and abstract underwent full text screening for the final selection. Reference lists of included studies were also hand-searched to identify additional relevant articles.
Eligibility criteria
To ensure relevance, inclusion and exclusion criteria were applied rigorously. The PICO (Population, Intervention, Context, and Outcome) framework used to identify eligible studies for this review is included in Supplementary Table 2. We included studies involving humans of all age/sex categories. Studies were excluded if they only involved animals, in-vitro, reviews or those in language other than English.
Study selection
A two-stage selection process was employed. In the first stage, two independent reviewers (RKA and ZL) screened the titles and abstracts of all retrieved articles to assess eligibility based on the eligibility criteria. Articles considered potentially relevant proceeded to full-text screening in the second stage. Disagreements during any stage were resolved through discussion or by consulting a third reviewer (KW). Finally, reference lists of selected studies were manually reviewed to ensure comprehensive inclusion of relevant articles.
Data extraction
Data from included studies were extracted using a standardized extraction form. The form was piloted on three studies to ensure consistency between reviewers, and included fields such as study characteristics Author and reference, country, cases, age (years), comorbidity, methods of diagnosis, mode of transmission, intervention, recommendations. Data extraction was independently performed by two reviewers (RKA and ZL) and cross-checked for accuracy. Discrepancies were resolved through team discussion or involvement of a third reviewer (KW).
Risk of bias and data synthesis
The methodological quality of the included studies was assessed using the Joanna Briggs Institute (JBI) critical appraisal checklists appropriate for analytical cross-sectional, case–control, and cohort studies [19]. The full risk of bias in individual studies was not assessed because of heterogeneity in study design including case reports, viewpoints, and mini review. Extracted data were synthesized descriptively and presented in tabular and narrative formats. Quantitative findings were tabulated to summarize study characteristics, clinical presentations, and public health responses. Narrative synthesis was employed to analyse qualitative findings, such as risk factors, clinical outcomes, and research gaps. We used ArcGIS Pro version 3.3 (ESRI, Redlands, CA) to create a choropleth map by countries to indicate the number of studies retrieved and included from each country. The graphs were created using Rstudio Desktop Version: 2025.05.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Study selection
From the four electronic databases including PubMed, Scopus, Web of Science, and Ovid, a total of 2,430 articles were retrieved. After removing 849 duplicates, 1,581 records were screened based on title and abstract. Then 1,518 records were removed based on title and abstract leaving 63 articles. Forty-four articles did not meet the eligibility criteria and were excluded after reviewing full text. Nineteen studies were included in the final analysis (Figure 1). Figure 1.PRISMA flow chart for study selection.
Study characteristics
Of the 19 studies [20–38], 12 (68.4%) were from India [20, 22, 25–28, 31, 32, 34–37] followed by Pakistan [21, 23, 29, 30, 33], Sri Lanka [24], and multi-country [38] (with data from India) (Figure 2). In total, there were 111 confirmed cases with two deaths [29, 32]. Nearly half of the confirmed cases were males (44, 39.6%), and 14.4% (16) were females, while 45.9% (51) did not specify their gender. Nearly two-thirds (81, 73.0%) of Mpox patients were from India, followed by Pakistan (18, 16.2%) and Nigeria (11, 9.9%) and one from Sri Lanka (1, 0.9%) (Figure 3). Mpox cases in South Asia predominantly affected young to middle-aged adults, typically between 22 and 35 years. The youngest patient was a neonate while the oldest patient was 60 years old (Table 1). The first confirmed case was reported in India in 2022 involving a 35-year-old male traveller from the United Arab Emirates (UAE). The first Mpox-related death was also reported in India in a 22-year-old male with encephalitis [37] followed by a 40-year-old Pakistani man due to complications from human immunodeficiency virus (HIV) [29]. While most cases were among adults, exceptions included neonatal case, such as an 8-day-old infant from Sri Lanka who contracted Mpox from close family members [24]. Figure 2.Study locations with bubbles size corresponding to the number of studies reviewed from inception to August 2024. Only 18 studies are presented here with one study based on multi-country. Figure 3.Distribution of Mpox patients by nationality. Table 1.Demographic characteristics of the included studies from South Asia.Author and referenceCountryCasesAge (years)ComorbidityMethods of diagnosisMode of transmissionInterventionRecommendationsGeorge et al. 2023 [20]India11HSV, transaminitisPCRHuman-to-humanIsolation of the patientEarly detection of patientsMallhi et al. 2023 [21]Pakistan5AdultsNRPCRHuman-to-human, travel-relatedScreening at entry pointsImprove healthcare preparednessMohapatra et al. 2022 [22]India10NSNRRT-PCR, serologyHuman-to-humanScreening and awareness campaignsAccurate differentiation between Mpox and HFMDMughal et al. 2023 [23]Pakistan5AdultsNRPCRHuman-to-humanPublic health alert issuedNeed for a syndemic responsePattiyakumbura et al. 2023 [24]Sri Lanka1NeonateNRPCR, X-rayMother-to-neonate transmissionNeonatal care; oxygen therapyAwareness for neonatal casesRelhan et al. 2022 [25]India5Mean 31Hepatitis B (one case)PCRHuman-to-humanIsolation and testing centres establishedEnhanced community surveillanceSahay et al. 2023 [27]India8AdultsNRPCRSurface-to-human potentialRigorous disinfection protocols in isolation wardsSurface decontaminationSahoo et al. 2022 [28]India12Median 28HIV (one case)PCRHuman-to-human, sexual contractConservative treatment; condom usage post-recoveryPrevention of STI-related transmissionSah et al. 2022 [26]India4AdultsNRPCR, serologyHuman-to-humanContact tracing; isolationStrengthened surveillance in SEARSatapathy et al. 2024 [29]Pakistan7NSHIVPCRHuman-to-human, travel-relatedLimited interventions; screeningPublic health educationShabbir et al. 2023 [30]Pakistan2AdultsNRPCRHuman-to-humanQuarantine measures, awareness campaignsImproved screening at entry pointsSharma et al. 2023 [31]India122NRPCR, genome sequencingHuman-to-humanGenome sequencingEarly warning systemsSingh et al. 2022 [32]India1021–31One fatal case with encephalitisPCRHuman-to-humanExpanded isolation unitsInclusion of vaccination protocolsUmair et al. 2023 [33]Pakistan416,18,32,34VZVPCRHuman-to-humanCase isolation; genomic sequencingAwareness for high-risk groupsVasu et al. 2023 [34]India10Mean 33One fatal case with encephalitisPCRHuman-to-humanTesting and monitoring protocolsAddress stigma in health-seekingWilliam et al. 2023 [35]India1022–35NRPCRHuman-to-humanTesting in isolated hospitalsManagement of asymptomatic casesYadav et al. 2022 [36]India231 &35NRPCR, genome sequencingHuman-to-human, close contactCase isolation and contact tracingStrengthened surveillance of travellersYadav et al. 2023 [37]India122NRPCR, genome sequencingHuman-to-humanSupportive ICU careRecognition of atypical presentationsYang et al. 2023 [38]Multi-country12NSNRSecondary dataHuman-to-humanSurveillance of global casesResearch on stigma effectsNS – Not specified; NR – not reported; HSV – herpes simplex virus; PCR – polymerase chain reaction; VZV – varicella zoster virus; HFMD – Hand foot and mouth disease; ICU – intensive care unit; STI – sexually transmitted infection; SEAR – WHO South-East Asia Region.
Travel history and other modes of transmission
Sixty-eight (76, 68.5%) patients reported a history of travel in the last three weeks prior to the diagnosis (Figure 4 and Supplementary Table 3). UAE was the most common destination of travel with 27% (21) of patients followed by Saudi Arabia (20, 26.3%) and Nigeria (9, 11.8%). However, 32.9% (25) did not report the country of travel (Figure 4). Figure 4.Travel history and country of travel amongst Mpox patients in the South Asia region.
The common mode of transmission was person-to-person. Several studies, including those from India and Pakistan, emphasized the role of close personal and sexual contact in spreading the virus. Notably, cases in India involving Nigerian nationals residing in Delhi were potentially linked to intimate contact or shared living spaces [25]. Neonatal transmission was reported in Sri Lanka, where a newborn contracted the virus from her mother and possibly her father, both of whom had symptoms after returning from Saudi Arabia [24] (Table 1).
Fomite transmission through contaminated surfaces was identified as a potential risk factor in healthcare and household settings. A study from India demonstrated the persistence of Mpox virus on surfaces in hospital isolation wards, emphasizing the need for rigorous disinfection and hygiene practices to mitigate secondary infections [27]. Healthcare workers also faced exposure risks due to environmental contamination and improper use of personal protective equipment (PPE) in isolation wards, as demonstrated in hospital-based studies in New Delhi [27]. Additionally, certain population groups, such as men who have sex with men (MSM), have shown higher prevalence rates of Mpox [21, 39] (Table 1).
Clinical features and disease severity
Common signs and symptoms among confirmed cases were vesiculo-pustular rashes (103, 92.8%,, fever (91, 82.0%), lymphadenopathy (73, 65.8%), and muscle aches (30, 27.0%). The rash typically progressed through stages, starting as macules, progressing to papules, vesicles, pustules, and finally scabs, with some studies reporting centrifugal distribution, initially affecting the face before spreading to other body parts, including the palms and soles. Atypical lesions that localized predominantly in the genital and perianal regions were also presented in 17.1% (19) of patients. Oral ulcers and follicular tonsillitis were observed in 10.8% (12) of patients (Figure 5). Figure 5.Symptoms of Mpox in the South Asia region. *Skin rash included vesicle, pustule, and macule.
Rare but severe complications, such as meningoencephalitis, have been reported in South Asia. For example, a fatal case in Kerala, India, involved a 22-year-old male with the clinical manifestation of fever, seizures, and altered sensorium, eventually progressing to acute brainstem dysfunction [32]. This case highlights the potential for Mpox to cause severe neurological involvement. Mpox in neonate (Sri Lanka) was associated with complications, including bronchopneumonia, emphasizing the need for specialized care in vulnerable populations [24].
Comorbidities such as HIV infection, have been identified as contributing factors to disease severity. For instance, the first fatal case of Mpox in Pakistan involved a 40-year-old man with HIV who succumbed to encephalitis [29]. Co-infections with other viruses, such as herpes simplex virus (HSV) and varicella zoster virus (VZV), have also been reported, leading to diagnostic challenges and influencing clinical outcomes [31, 33]. Immunocompromised individuals were particularly vulnerable to severe Mpox [33].
Risk of bias
Of 19 studies, only four studies qualified for risk of bias assessment – two each for case reports [20, 24] and case series [25, 28]. For case reports, studies clearly described demographic characteristics, patients’ history, current clinical conditions of patients, diagnostic methods, and treatment. The post-interventional conditions, adverse events, and takeaway lessons were clearly described in the papers (Supplementary Table 4). Similarly, case studies outlined clear inclusion criteria, conditions were reliably measured, consecutive and complete inclusion of participants. The demographics, clinical information of the participants were clearly outlined. The outcomes or follow up results of cases were clearly reported. Statistical analysis done where they were appropriate (Supplementary Table 5).
Diagnosis and source of infection
Accurate and timely diagnosis of Mpox is essential for effective case management and control of transmission. Nearly all the studies employed polymerase chain reaction (PCR) and genomic analysis [20–37] except for one study that used secondary data, and diagnostic methods were not reported [38]. Two studies reported the sources of samples for diagnosis: these were blood, urine, and lesion swabs of body fluids [20, 25] (Table 1).
Public health responses
The emergence of Mpox in South Asia has prompted varied governmental responses across countries including awareness campaigns, guidelines for managing (care) of Mpox patients, diagnosis, isolation protocols, and surveillance. However, responses varied across countries. India implemented all five recommended measures, while Pakistan effectively carried out surveillance, isolation, and diagnosis but fell short in conducting widespread awareness campaigns. While Sri Lanka reported only implementing guidelines for managing Mpox patients (Figure 6 and Table 1). Figure 6.Country-specific interventions for Mpox in the South Asia region.
While no specific Mpox vaccine has been deployed widely in South Asia, governments have considered vaccination for high-risk groups. India's public health guidelines discuss the potential role of smallpox vaccines, given their cross-protective efficacy against Mpox [35]. However, logistical challenges and limited vaccine availability have hindered large-scale implementation. Therefore, the capacity to manufacture vaccines locally would greatly improve South Asia vaccine access [40].
In Pakistan, the National Institute of Health (NIH) spearheaded surveillance and monitoring efforts, particularly at points of entry such as airports, where travellers were screened for symptoms. Educational campaigns were conducted to address stigma associated with Mpox, particularly among vulnerable populations such as the MSM community [21]. These campaigns aimed to encourage early reporting and reduce barriers to seeking healthcare. Sri Lanka adopted similar strategies, integrating Mpox monitoring into existing surveillance frameworks for other infectious diseases [24].
Discussion
This systematic review offers a comprehensive synthesis of current knowledge on Mpox in South Asia, highlighting key epidemiological patterns, clinical presentations, disease severity, and mitigation measures. In the region, Mpox cases were frequently reported among travelers returning from the Middle East and other international destinations. Human-to-human transmission and stigma associated with Mpox resulted in delayed diagnosis and poor compliance with isolation. All cases reported similar clinical manifestations to those reported in other areas. Mpox response in the region were multifaceted but enhanced surveillance and education were two important measures that contained outbreaks. The findings highlight critical gaps in research and response strategies, emphasizing the need for region-specific responses.
Mpox cases in South Asia have predominantly been linked to travel from endemic regions, particularly the Middle East, with a smaller proportion involving local transmission [21, 27]. This trend highlights the critical role of cross-border mobility in the spread of Mpox and underscores the importance of effective screening at points of entry [41]. While India has reported the highest number of cases in the region, other countries like Pakistan and Sri Lanka have also documented cases, suggesting the need for robust surveillance systems. In 2025, global Mpox cases continue to be reported from Africa including Gambia, Sierra Leone, Guinea, Liberia, Ghana, and Togo [42]. Cases have decreased in the Americas to 902 cases and one death in nine countries with Brazil (425 cases and 1 death) and the United States (245) reporting the most cases from the region [42]. In Europe, 117 cases were reported between April and May 2025, mostly by Germany [33], the Netherlands [21], Spain [14], and France [13, 43].
In South Asia, Mpox cases have predominantly been reported among young to middle-aged adults, reflecting global trends in disease epidemiology [44]. However, rare instances involving a neonate has also been documented, such as the case from Sri Lanka, highlighting the potential vulnerability of this age group despite their low representation in overall case counts [24]. This neonatal case underscores the importance of strengthening maternal and child health surveillance within Mpox surveillance systems to ensure early detection and appropriate clinical management.
Human-to-human transmission remains the primary mode of spread in the region, while contaminated fomites and potential sexual transmission were other sources of infection, similar to findings from other parts of the world [44, 45]. Several studies identified certain population, including MSM, people who engage in higher-risk sexual practices, and immunocompromised patients, such as those with HIV, were at a higher risk of Mpox infection [21, 29]. The stigma associated with these groups may delay diagnosis and treatment, reduce compliance with isolation and other preventive measures, and result in reluctance to disclose contacts among infected individuals, further exacerbating transmission risks [46]. Misconceptions about Mpox, and the perceived link to specific sexual behaviours has deterred individuals from seeking medical care, potentially leading to spreading of disease in communities [38]. This is especially relevant in cases involving MSM communities, where stigma may have amplified delays in seeking healthcare access [25].
The clinical presentation of Mpox in South Asia aligns with global patterns, with commonly reported symptoms including vesiculo-pustular rashes, fever, lymphadenopathy, and myalgia [20, 34]. However, several studies documented atypical manifestations such as genital lesions, localized rashes, and neurological complications, including encephalitis [33, 37]. These findings highlight the need for healthcare providers to recognize diverse presentations to avoid misdiagnosis, particularly in settings with overlapping diseases such as VZV or HFMD [47].
Similar to other studies, this study reported that the pre-existing comorbidities, such as HIV, diabetes, and hypertension were associated with disease severity [48]. Additionally, co-infections with other viral pathogens such as HSV and VZV were documented, further complicating clinical outcomes [33, 49]. These findings reinforce the importance of early identification and targeted management strategies for populations with existing comorbidities, including immunocompromised individuals and neonates.
Government responses to Mpox in South Asia were multifaceted with various strategies used to contain outbreaks. Enhanced surveillance and screening measures, particularly at airports and points of entry, have played a crucial role in identifying and isolating cases early. In India, specific guidelines were issued for healthcare workers to facilitate symptom recognition and management [30, 32], while in Pakistan, educational campaigns targeted stigma reduction, particularly among high-risk groups such as MSM [25, 38]. Despite these efforts, the absence of a widely deployed Mpox vaccine in the region remains a critical gap [21, 50]. To date, there is no proven effective antiviral treatment for Mpox. Some antivirals have received emergency use authorization in some countries and are being evaluated in clinical trials. It is a priority to continue evaluation and to focus on optimizing supportive care for patients [51]. While smallpox vaccines have been considered for high-risk groups, challenges such as limited vaccine availability and logistical barriers have hindered large-scale implementation. In addition, all studies failed to outline the public acceptance of vaccine. Therefore, strengthening vaccination strategies by overcoming the logistical barriers, bolstering diagnostic capacity, prioritization of vaccine strategies, and public acceptance should be explored. Furthermore, addressing social stigma through public awareness campaigns are essential components of an effective Mpox mitigation plan in South Asia.
Polymerase chain reaction and genomic analysis were the commonly used diagnostic methods using swabs from lesions and body fluids [20–37]. In the absence of skin lesions, testing can be done using swabs of the throat or anus. Other methods including immunohistochemistry of skin lesions and electron microscopy, which can provide important clinical evidence [52]. However, PCR or genetic sequence remains a gold standard for the diagnosis of Mpox. So, strengthening these diagnostic capabilities should be undertaken for future management of Mpox in the region.
This systematic review is limited by the available studies, which varied in their scope, methodology, and reporting quality. Many studies lacked detailed demographic, clinical, and temporal data. These may have influenced the findings of this review. Potentially this is due to studies predominantly reporting case reports or case series with limited ability of the disease to cause widespread local infection. Future research should prioritize standardized data collection and reporting to facilitate regional and global comparisons.
The analysis of Mpox in South Asia highlights several significant research gaps that must be addressed to enhance disease management and control. To strengthen Mpox preparedness and response, we recommend enhancing early detection through improved lesion recognition, community-based surveillance, screening at entry points, surveillance of travellers, and the establishment of robust early warning systems. Healthcare preparedness should be reinforced by ensuring accurate differentiation between Mpox and similar conditions such as HFMD, recognizing atypical and asymptomatic presentations, and incorporating vaccination protocols where feasible. The role of animal reservoirs in zoonotic transmission also remains poorly understood [50]. Public health responses should prioritize a syndemic approach, surface decontamination, and prevention of STI-related transmission. Awareness campaigns must address neonatal and high-risk groups, promote public health education, and reduce stigma that hinders health-seeking behaviours. Finally, collaborative efforts addressing these gaps can support evidence-based policy, control and preparedness for Mpox in South Asia.
Conclusion
Mpox is becoming a serious public health problem in the region with some countries reporting locally acquired cases alongside the ongoing risk of importation due to international travel and trade. Addressing the research gaps and enhancing diagnostic, surveillance, and response capabilities will be critical to mitigating the disease's impact in the region. A coordinated approach involving cross-border collaboration, community engagement and education, and investment in healthcare infrastructure is required to improve Mpox management, prevention and preparedness. Future public health strategies must incorporate strengthened surveillance, improved diagnostic capacity, culturally sensitive response and targeted interventions to reduce transmission in high-risk groups and ensure effective outbreak control in South Asia.
Author contributions
KW, TT, and RA were involved in conceptualization, formal analysis, supervision, validation, visualization, writing – original draft, reviewing, and editing. RA and ZL were involved in data curation, investigation, and writing – review and editing. SV, RM, MK, WH, and ATS were involved in supervision and critical revision of manuscript. All authors approved the final draft.
Supplementary Material
Supplementary file.docx
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kugelman JR, Johnston SC, Mulembakani PM, et al. Genomic variability of monkeypox virus among humans, democratic republic of the Congo. Emerg Infect Dis. 2014;20(2):232–239.24457084 10.3201/eid 2002.130118 PMC 3901482 · doi ↗ · pubmed ↗
- 2Bonilla-Aldana DK, Rodriguez-Morales AJ. Is monkeypox another reemerging viral zoonosis with many animal hosts yet to be defined? Vet Q. 2022;42(1):148–150.35686457 10.1080/01652176.2022.2088881 PMC 9225742 · doi ↗ · pubmed ↗
- 3Moss B. Understanding the biology of monkeypox virus to prevent future outbreaks. Nat Microbiol. 2024;9(6):1408–1416.38724757 10.1038/s 41564-024-01690-1 · doi ↗ · pubmed ↗
- 4Wickramasinghe M, Weerasekera M, Perera N. Mpox outbreak in previously Non-endemic countries: A review on impact on Asia. Clin Pathol. 2024;17:2632010 ( 241300679).10.1177/2632010 X 241300679 PMC 1160347239610468 · doi ↗ · pubmed ↗
- 5WHO. 2022-24 Mpox (Monkeypox) Outbreak: Global Trends 2024 [Available from: https://worldhealthorg.shinyapps.io/mpx_global/.
- 6Patel A, Bilinska J, Tam JCH, et al. Clinical features and novel presentations of human monkeypox in a central London centre during the 2022 outbreak: descriptive case series. Br Med J. 2022;378:e 072410.35902115 10.1136/bmj-2022-072410 PMC 9331915 · doi ↗ · pubmed ↗
- 7Thornhill JP, Barkati S, Walmsley S, et al. Monkeypox virus infection in humans across 16 countries – April-June 2022. N Engl J Med. 2022;387(8):679–691.35866746 10.1056/NEJ Moa 2207323 · doi ↗ · pubmed ↗
- 8Bunge EM, Hoet B, Chen L, et al. The changing epidemiology of human monkeypox-A potential threat? A systematic review. P Lo S Negl Trop Dis. 2022;16(2):e 0010141.35148313 10.1371/journal.pntd.0010141 PMC 8870502 · doi ↗ · pubmed ↗