The cost of inaction to strengthen the resilience of primary health care in Latin America and the Caribbean: a modelling study
Tharindu Wickramaarachchi, Nick Scott, Pablo Villalobos Dintrans, Marina Gonzalez-Samano, Manuela Villar Uribe

TL;DR
This study estimates the health and economic costs of not strengthening primary health care in Latin America and the Caribbean, showing significant impacts from potential future health system disruptions.
Contribution
The study introduces a modeling approach to quantify the societal costs of health system shocks in primary health care across 33 LAC countries.
Findings
Modeled health shocks could result in millions of unintended pregnancies and tens of thousands of deaths between 2026–2030.
The estimated societal economic cost of these shocks ranges from $7 to $37 billion.
Strengthening primary health care is shown to be economically justified to mitigate these impacts.
Abstract
The Latin America and the Caribbean (LAC) region will face future public health emergencies due to pandemics, natural disasters, migration, economic crisis or other unforeseen events. These events disrupt healthcare service coverage with consequences for morbidity, mortality and economic productivity. This study aimed to estimate the health and economic cost of potential future health system shocks, as a proxy for the cost of inaction to strengthen the resilience of primary health care. For 33 countries in LAC, primary health care shock scenarios were modelled as short-term reductions to the coverage of antenatal care and child health interventions using the Lives Saved Tool, and to family planning services and non-communicable disease management using custom models. Primary health care shocks starting in 2026 and leading to 25–50% relative coverage reductions (50% being a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
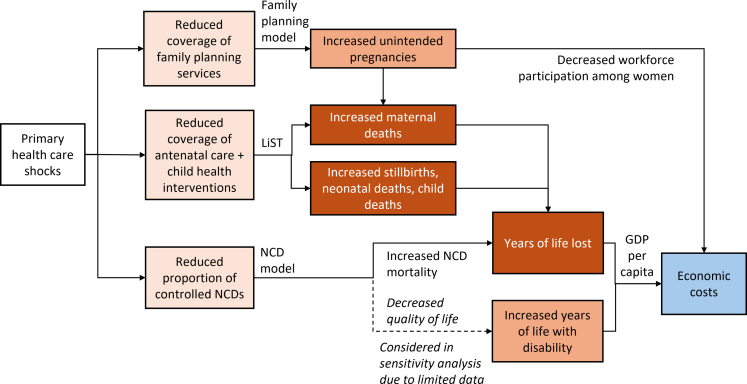 Figure 1
Figure 1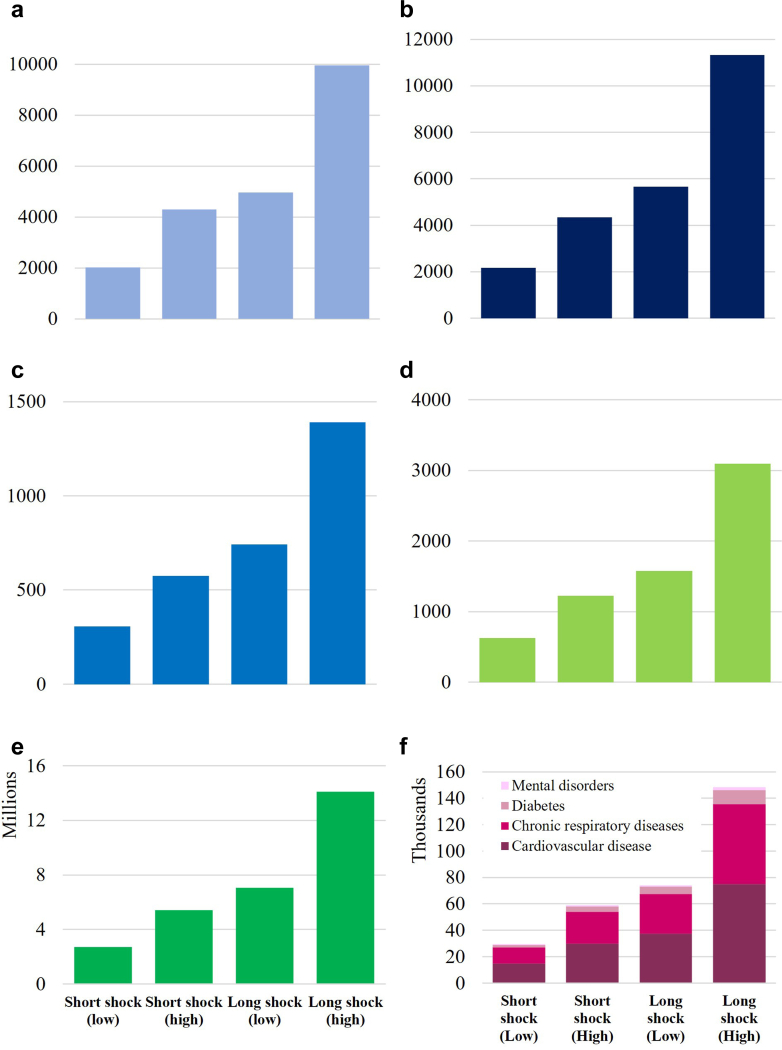 Figure 2
Figure 2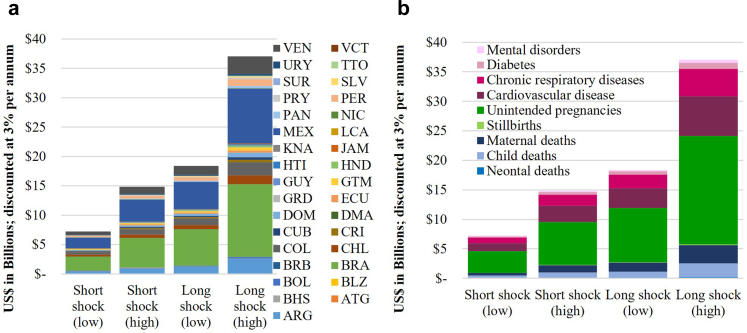 Figure 3
Figure 3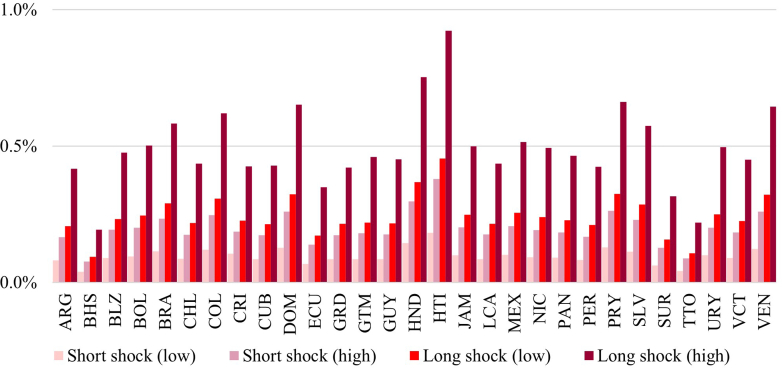 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare Systems and Reforms
Research in contextEvidence before this studyCountries in the Latin American and Caribbean (LAC) were significantly impacted by COVID-19, with excess morality rates well above the Organisation for Economic Co-operation and Development (OECD) average. The COVID-19 pandemic uncovered challenges in maintaining routine health care services in many LAC countries.The LAC region is vulnerable to various future public health emergencies or health system shocks due to pandemics, natural disasters, migration, economic crises or other unexpected events. These events could disrupt healthcare service coverage with consequences for morbidity and mortality, and the majority burden is likely to fall within the remit of primary health care (PHC). Quantifying the potential health and economic cost of such shocks could provide a strong rationale for investment to build PHC resilience.We searched PubMed databases and Google Scholar for any relevant literature published after 2020 with keywords: (“primary health care” or “health service disruptions” or “disruption scenarios”) and (“Latin America and the Caribbean”) and (“modelling” or “economic cost”). Several studies modelled the impact that shocks to specific health care services could have on health but not economic outcomes, and some studies estimated the health and economic impacts of shocks but considering a limited subset of interventions or services. There were studies that argued the importance of building resilience in PHC; however, no studies were identified that quantified the health and economic impact of shocks to PHC service coverage.Added value of this studyThis study estimated the health and economic cost of reductions in PHC service coverage due to potential future health system shocks, as a proxy for the cost of inaction to improve PHC resilience. We assumed that without investment in PHC resilience, PHC service coverage would reduce when a shock occurred. We estimated that if a shock occurred that led to a 25–50% relative reduction in PHC service coverage with recovery time ranging from one to five years, then across the 33 countries in the LAC region this could lead to an additional 35,000–174,000 deaths (stillbirths, neonatal deaths, child deaths, maternal deaths and deaths due to non-communicable diseases) and 2.7–14.1 million unintended pregnancies, corresponding to US$7.2–37.0 billion in societal economic costs per shock.Implications of all the available evidenceFuture unforeseen events with potential to disrupt PHC service coverage could have significant health and economic consequences in the LAC region. Considerable investment to build resilience in PHC would be warranted if it could minimise or eliminate the impact of such shocks on service coverage.
Introduction
More than five years since the COVID-19 pandemic declaration, the evidence is clear: COVID-19 had a significant impact on Primary Healthcare Systems (PHC) worldwide.1 In addition to the millions of deaths directly caused by COVID-19 globally between 2020 and 2021, the COVID-19 pandemic led to substantive disruptions to the coverage and quality of healthcare services. For example, there was an observed increase in maternal deaths (odds ratio [OR] = 1.37), stillbirths (OR = 1.28) and neonatal deaths (OR = 1.01) globally during vs before the pandemic2^,^3 due to reductions in antenatal and delivery care services and reduced healthcare seeking behaviours among pregnant women. Disruptions to healthcare services were most prominent in low- and middle-income countries (LMICs),4 related to weaknesses in the health systems.5
COVID-19 hit Latin American and Caribbean (LAC) countries harder than any other region, accounting for about 30% of global COVID-19 deaths despite having only 8% of the world's population.6 The COVID-19 pandemic revealed that many LAC health systems were not sufficiently strong to absorb the shock, and as a consequence they faced challenges in maintaining routine care. Available evidence indicates that pre-existing system challenges—such as workforce shortages, fragmented service delivery, and limited hospital bed availability—exacerbated the pandemic's impact.7, 8, 9 Disruptions in care—such as an 8% drop in DTP3 vaccination coverage in 2020 compared to the 2015–2019 average—illustrated how PHC struggled to maintain essential services, with the largest reductions observed in Argentina, Mexico, and Brazil.8 In 14 LAC countries, an average of 20% of households reported healthcare disruptions in mid-2020, most often due to healthcare supply constraints.7^,^10 In Brazil, Ecuador, Mexico, and Peru, hospitalizations for treatable conditions fell by 28% and related mortality increased by 15%, disproportionately affecting poorer regions; it was estimated that maintaining services could have prevented at least 96,000 deaths.11 Care management programs for non-communicable diseases (NCDs) were also impacted, with a 39% reduction in diabetes blood tests in Argentina and a 41% reduction in Chile in 2020, and a 63% reduction in breast cancer screenings in Brazil compared to the 2018–19 average.10
A strong PHC is critical to a health system's capacity to absorb and recover from shocks,8 and evidence shows that countries with stronger PHC were able to respond faster and more effectively to the COVID-19 pandemic.12 Studies have identified that lower pre-pandemic intervention coverage, related to weaker PHC systems, were associated with larger disruptions of services.13 Although there is much heterogeneity, countries with larger PHC expenditure per capita, such as Uruguay, Brazil, Costa Rica, and Chile, had lower excess mortality rates over the initial COVID-19 years than countries like Haiti, Peru or Mexico.8^,^14^,^15 Countries with stronger PHC are able to place greater emphasis on community-based services, helping to reduce pressure on hospitals and broader health systems while minimising complications and direct mortality. The relevance of strong PHC in responding to other health crises has been observed for influenza,16 SARS outbreak in 2003,14 and cholera.17
The majority of the burdens associated with health emergencies fall within the remit of PHC.18^,^19 A robust PHC system, which is people- and community-oriented and offers comprehensive, continuous, and coordinated care, can significantly enhance preparedness and resilience during and after health emergencies.8 Regional resolutions by Pan American Health Organization (PAHO) Member States emphasize a PHC approach to address population needs, accelerate pandemic recovery, and move towards universal health care.20 The World Bank (WB) has also called for investments in PHC-based systems to prepare for future public health emergencies, protect lives, and foster human capital. The WB-PAHO Lancet Regional Health Americas Commission on PHC and Resilience seeks to guide future development of PHC and resilience in the region. Despite efforts to date, there remains a critical need to transform PHC systems in LAC to effectively prevent, respond to and recover from health system shocks, particularly as the region faces risks compounded by weak health systems, fragmentation, constrained budgets, and long-standing inequalities.20
Quantifying the health and economic impacts of potential shocks to PHC services can provide rationale for investing in PHC resilience. Previous work has modelled the impact that shocks to specific health care services could have on health outcomes. For example, one study estimated that a 9·8–18·5% reduction in high-impact maternal and child health interventions and a 10% increase in wasting for a six month period could result in 253,500 additional child deaths and 12,200 additional maternal deaths across 118 LMICs.21 Another study estimated that reductions to family planning services of different length (3–12 months) and magnitude (5–40%) in 114 LMICs could lead to 325,000 to 15 million additional unintended pregnancies.22 In general, while some modelling studies are available that estimate the impact of shocks to health services, they have estimated health impacts only or have estimated health and economic impacts but for a limited subset of interventions. To our knowledge, studies are not available quantifying the health impact of shocks to PHC service coverage, or the economic outcomes associated with these shocks.
The objective of this modelling study was to estimate the health and economic cost of reductions in PHC service coverage due to potential future health system shocks for 33 countries in the LAC region. This evidence can be used as a proxy for the cost of inaction to strengthen PHC, and to provide a rationale to support investment in improving PHC resilience.
Methods
Overview
The potential impact of health system shocks (e.g., epidemiological events such as COVID-19, dengue, and Zika; demographic such as migration; natural disasters, including floods, hurricanes, fires, and earthquakes; and economic, such as recessions and economic crisis) on PHC were approximated as reduced service coverage, with the magnitude and duration of the coverage reduction dependent on the nature of the health system shock. The impact of coverage reductions were estimated for family planning, antenatal care, child health, and NCD services domains (Fig. 1), compared to a scenario with maintained coverage (“strengthened primary health care”).Fig. 1Framework used to estimate the health and economic costs of shocks to primary health care services. The Lives Saved Tool (LiST)23, 24, 25 was used to estimate the impact of reduced coverage of antenatal care and child health interventions and custom models were used to estimate the impact of reduced primary health care coverage on family planning and non-communicable disease (NCD) mortality and years lived with disability.
Settings
The modelling was undertaken for 33 countries in the LAC region. Some countries did not have all service domains modelled due to limited data to parametrize the models (Supplementary Material, Appendix A).
Model structure
The impact of health system shocks on antenatal care and child health service domains was modelled using the Lives Saved Tool (LiST).23, 24, 25LiST is a modelling tool widely used to estimate the health impacts of changes in intervention coverage, with extensive model details and resources available online at livessavedtool.org. A full list of interventions considered for each service domain is available in Supplementary Material, Appendix B (Table B.1). Reduced antenatal care service utilization and reduced coverage of child health interventions (including interruptions to routine Bacillus Calmette–Guérin vaccine (BCG), pentavalent, and polio immunization programs) were modelled to increase maternal deaths, stillbirths, newborn deaths and child deaths relative to the effect sizes in Table 1.Table 1. Effect sizes for the interventions modelled in LiST and relative reduction in mortality risk of non-communicable diseases (NCDs).Effect sizes for the LiST modelInterventionImpactEffect size****SourceTetanus toxoid vaccinationNewborn mortality (due to tetanus)RR = 0.06 (0.02, 0.20)Blencowe et al., 201026Prevention of malaria during pregnancyMaternal anemiaRR = 0.90 (0.84, 0.95)Moorthy et al., 202027Small for gestational age birthsIRR = 0.65 (0.55, 0.77)Eisele et al., 201228Syphilis detection and treatmentNewborn mortalityRR = 0.20 (0.13, 0.32)Blencowe et al., 201129Preterm birthRR = 0.36 (0.27, 0.47)Blencowe et al., 201129StillbirthRR = 0.18 (0.10, 0.33)Blencowe et al., 201129Iron supplementationMaternal anemiaRR = 0.51 (0.38, 0.7)Hansen et al., 202330Low birth weightRR = 0.30 (0.13, 0.68)Hansen et al., 202330Small for gestational age birthsRR = 0.39 (0.17, 0.86)Hansen et al., 202330Multiple micronutrient supplementationMaternal anemiaRR = 0.51 (0.38, 0.70)Hansen et al., 202330Stillbirth (vs iron supplementation)RR = 0.91 (0.86, 0.98)Hofmeyr et al., 202331Small for gestational age births (vs iron supplementation)RR = 0.93 (0.88, 0.98)Oh et al., 202032Hypertensive disorder case managementMaternal mortality (due to hypertensive disorders)RR = 0.50 (0.30, 0.60)Pollard et al., 201333Diabetes case managementStillbirthRR = 0.9Syed et al., 201134Malaria case managementMaternal mortalityRR = 0.2 (0.10, 0.25)Pollard et al., 201333Pentavalent (DPT, Hib, HBV)Child mortalityRR = 0.06 (0.03–0.12)Fulton et al., 201635Pneumococcal–Three dosesChild pneumonia (clinical)RR = 0.94 (0.91–0.98)Lucero et al., 200936All-cause mortalityRR = 0.89 (0.79–1.01)Lucero et al., 200936Rotavirus—three dosesSevere diarrheaRR = 0.5 (0.34–0.62)Lamberti et al., 201637Meningococcal A single doseMeningococcal meningitisOR = 0.019 (0.002–0.138)Daugla et al., 201438Malaria vaccine boosterSevere malariaRR = 0.65 (0.52–0.84)The RTS,S Clinical Trials Partnership, 201139Measles single doseChild mortalityRR = 0.15 (0.13–0.17)Sudfeld et al., 201040Vitamin A supplementationChild mortalityRR = 0.88 (0.79–0.98)Imdad et al., 202241Zinc supplementationIncidence of diarrheaRR = 0.87 (0.81–0.94)Yakoob et al., 201142Relative reduction in mortality for the NCD modelNCD categoryNCD conditionRelative reduction in mortality when controlled****SourceCardiovascular diseaseAll conditionsRR = 0.89 (0.81–0.98)Statins:Mills et al., 200843RR = 0.95 (0.92–0.99)Pharmacological blood pressure lowering: The Blood Pressure Lowering Treatment Trialists' Collaboration44Chronic respiratory diseasesChronic obstructive pulmonary diseaseHR = 0.72 (0.53–0.99)Mintz et al., 202345DiabetesDiabetes mellitus type 2HR = 0.93 (0.88–0.99)Campbell et al., 201746Mental disordersAny psychological disorderRR = 0.84 (0.74–0.96)aSarah et al., 201647RR: Relative Reduction; IRR: Incidence Rate Ratio; HR: Hazard Ratio.aThe relative reduction in mortality from any psychological disorder.
The impact of health system shocks on family planning services was modelled as a relative reduction in the proportion of women accessing modern contraception services free of charge (57.8% as a proxy for public vs private access).48 Those impacted were modelled to shift from modern methods (average effectiveness 91–99% based on country-specific methods mix; Supplementary Material, Appendix Table D.3) to traditional methods (average effectiveness of 82%).23 This change in contraception effectiveness was modelled to increase unintended pregnancies, accounting for country-specific fertility rates and overall contraception prevalence rates (Supplementary Material, Appendix B). Additional maternal deaths were also included from the additional pregnancies based on country-specific maternal mortality ratios.
The impact of health system shocks on NCDs was estimated using a simple compartmental model (Supplementary Material, Appendix B), with NCDs across four categories (cardiovascular disease, chronic respiratory disease, diabetes, and mental disorders) selected for inclusion because they are amenable to PHC as well as the availability of estimates for the relative reduction in mortality when NCDs are controlled (Table 1). Cancers were not included because, although reduced screening is likely to lead to missed diagnoses and opportunities for early treatment, it is not clear to what extent a short disruption to screening would be noticeable following the shock, and whether the role of PHC, as opposed to tertiary care, would be critical in the treatment to prevent cancer-specific mortality. This makes this analysis an underestimate of the impact of health system shocks on NCDs. For each country, the model projected the cause-specific mortality for each NCD (based on IHME estimates),49 as well as the proportion of people with each NCD accessing primary health care (based on universal health care coverage index).50 In the health system shock scenarios, the proportion of people accessing PHC was reduced, leading to increased mortality based on estimates of the impact of primary health care (Table 1).
Data inputs
The data domains used to populate the models considered for this study are described in Table 2 including their sources. Country-specific values are available in the Supplementary Material for population projections (Supplementary Material, Appendix D Tables D.1 and D.2), epidemiological indicators (Appendix Table D.3), NCD prevalence (Appendix Table D.4), NCD mortality rates (Appendix Table D.5), estimated proportion of NCDs that are controlled (Appendix Table D.6), age distribution of NCD deaths (Appendix Table D.7), healthy life expectancy by age (discounted and undiscounted; Appendix Tables D.8 and D.9), economic parameters (Appendix Table D.10), baseline coverages of the interventions in the LiST model (Appendix Table D.11), coverages for the shock scenarios of the interventions in the LiST model (Appendix Tables D.12–D.15), percentage of women (18–49 years old) using modern contraception methods for shock scenarios (Appendix Table D.16), and percentage of women (18–49 years old) using traditional contraception methods for shock scenarios (Appendix Table D.17).Table 2. Main data inputs and their sources.ModelData inputSourceLiST modelPopulation projectionsUN WPP 2024 projectionsMortality rates: maternal mortality, neonatal mortality, child mortality, stillbirthsWHO Global Health Observatory; WHO Maternal, Newborn, Child and Adolescent Health and AgeingPrevalence of stunting and wastingBaseline coverage of interventions (ANC, vaccines and child health)LiST v6.3623, 24, 25 based on country surveys; regional estimatesaNCD modelPopulation projectionsUN WPP 2024 projectionsPrevalence of NCD conditionsIHME/GBD49Mortality rates for NCD conditionsIHME/GBD49Percentage controlled/managed NCD conditionsˆEstimated using UHC index and country data50Family planning modelPopulation projectionsUN WPP 2024 projectionsContraception prevalence rateWHO Global Health Observatory; WHO Maternal, Newborn, Child and Adolescent Health and AgeingUnmet need for family planningBirth ratesUN WPP 2024 projections; used as a proxy for pregnancy rateFamily planning method mixLiST v6.3623, 24, 25 based on country surveys; regional estimatesaEconomic modelAge- and country-specific healthy life expectancyIHME/GBD49Age-distribution of NCD mortality (by cause)Derived from deaths; IHME/GBD49GDP per capitaWorld Bank data51Female workforce participation ratesWorld Bank data52Maternal time out of workforceUNICEF53; The Caribbean Society for Human Resource Professionals54UHC: Universal Health Coverage; IHME: Institute for Health Metrics and Evaluation; GBD: Global Burden of Disease; NCD: non-communicable disease.aExtracted from LiST; based on country surveys or regional estimates if no survey conducted for the country (Appendix Tables D.3 and D.11).
Scenarios
Assuming that a potential health system shock occurs in 2026, several scenarios were projected for the period 2026–2030:
- 1.Strengthened PHC: Assuming investment occurs to strengthen PHC, such that PHC intervention coverages remain constant when the health system shock occurs.
- 2.Short PHC shock (low/high): PHC intervention coverage in 2026 assumed to experience relative reductions of (a) 25% or (b) 50%, before returning to baseline levels in 2027 and maintained through to 2030.
- 3.Long PHC shock (low/high): PHC intervention coverage in 2026 assumed to experience relative reductions of (a) 25% or (b) 50%, before linearly increasing to reach baseline levels again by 2030.
These scenarios were derived such that the PHC shock corresponds approximately to the first year of COVID-19 (for example, in Brazil an 42.5% reduction in appointments for physicians was observed).55
Health impact of PHC shock scenarios
For each scenario, the main outcomes compared to the strengthened PHC scenario were stillbirths, neonatal deaths, child deaths, maternal deaths, deaths due to NCDs and unintended pregnancies over the period of 2026–2030.
Societal economic costs of PHC shock scenarios
The health impacts of each scenario compared to the strengthened PHC scenario were converted to societal economic costs using a value of statistical life year approach following global investment frameworks (Supplementary Material, Appendix E).56^,^57 A lifetime time horizon for those impacted across the 2026–2030 period. For each country, excess deaths (maternal, newborn and child deaths, stillbirths, and NCD-related deaths) were converted to years of life lost based on country-specific distributions for the age of different NCD deaths and age of pregnancies, combined with country- and age-specific expected years of life remaining.58^,^59 Years of life lost were valued at 2023 GDP per capita, with future years discounted at 3% per annum.
Additional unintended pregnancies were assumed to lead to reduced workforce participation, with country-specific maternity leave policies used to estimate time out of the workforce and adjustments made for workforce participation among women.58^,^60 Time out of the workforce was valued at country-specific GDP per worker, with future years discounted at 3% per annum.
Sensitivity analysis
Two sensitivity analyses were run. First, where additional stillbirths and newborn deaths resulting from the additional pregnancies were also considered; these were not included in the main analysis to avoid circular logic in counting the societal economic costs (i.e., in the strengthened scenario their conception did not occur, whereas in the health system shock scenario they contributed many years of life lost), however they would still be expected outcomes. Second, there are likely to be additional impacts from disrupted NCD services leading to increased years lived with disability; however, studies are not available quantifying how NCD disability weights are impacted by accessing PHC. Therefore, a sensitivity analysis was conducted considering the additional economic costs of the health system shock scenarios if accessing PHC led to a 5% reduction in disutility weights for each NCD.
Ethics
Ethics approval was not required as this study only used aggregate, publicly available data and did not involve any participants.
Role of funding source
This work was funded by the World Bank. Co-authors from the World Bank contributed to the study design, analysis, and reviewing and editing of the manuscript.
Results
Strengthened PHC scenario
In the strengthened PHC scenario with service coverage maintained over 2026–2030, across the 33 countries and the subset of service domains considered, we estimated 367,000 stillbirths, 429,000 neonatal deaths, 327,000 child deaths, 41,000 maternal deaths, ∼7 million deaths from NCDs (deaths due to cardiovascular diseases: 4.5 million; chronic respiratory diseases: 1 million; diabetes: 1.2 million and mental disorders: 211,000) and 57 million births (Supplementary Material, Appendix Figure F1).
PHC shock scenarios: health impacts
Depending on the magnitude (low or high) and duration (short or long) of the shock to PHC services, we estimated an additional 600–3100 stillbirths, 300–1400 neonatal deaths, 2000–10,000 child deaths, 2100–11,300 maternal deaths, 29,000–149,000 deaths from NCDs and 2.7–14.1 million unintended pregnancies across the 33 countries over 2026–2030 (Fig. 2, Table 3).Fig. 2Cumulative additional health outcomes for each primary health care shock scenario. Additional child deaths (a), maternal deaths (b), neonatal deaths (c), stillbirths (d), additional unintended pregnancies (e) and additional NCD deaths (f) over 2026–2030.Table 3. Cumulative health outcomes of primary health care shock scenarios, 2026–2030.ScenarioExcess stillbirthsExcess neonatal deathsExcess child deathsExcess maternal deathsExcess NCD deathsAdditional unintended pregnanciesShort primary health care shock (low; 25%)6273062025217129,4882,708,996Short primary health care shock (high; 50%)12265744291434359,0815,417,993Long primary health care shock (low; 25%)15777414959565474,1647,054,927Long primary health care shock (high; 50%)30951390996011,313148,52814,109,854
The increase in total deaths attributable to each shock (neonatal deaths, child deaths, maternal deaths, stillbirths and deaths due to NCDs, over the entire shock duration) ranges from 0.43 to 2.15% of total annual deaths, depending on the magnitude and recovery duration.
NCD deaths were the largest share of total excess mortality (85%), followed by maternal deaths (6%), child deaths (6%), stillbirths (2%) and neonatal deaths (1%). These distributions of excess deaths were influenced by the specific interventions modelled (Supplementary Material, Appendix B) and their baseline coverages (Supplementary Material, Table D.11). The breakdown of excess NCD deaths by sub-condition was dependent on relative mortality rates (Supplementary Material, Table D.5) as well as the proportion of people with each sub-condition controlled (Supplementary Material, Table D.6), who were susceptible to the PHC disruptions.
PHC shock scenarios: economic impacts
The excess health burden in the shock scenarios corresponded to a total discounted economic cost ranging from US7.2–37.0 billion ([Fig. 3](#fig3)), depending on the magnitude and duration of the shock. Reductions in workforce participation due to additional unintended pregnancies represented the largest share of the economic cost (49–50%), followed by excess deaths due to NCDs (35–36%) and maternal deaths (6–8%).Fig. 3**Cumulative societal economic cost of primary health care shock scenarios (FP + MNCH + NCDs), disaggregated across countries (a), and across cause of mortality or unintended pregnancies (b).** Costs are total over 2026–2030 across the 33 countries and subsets of service areas modelled, presented in 2023 US with 3% per annum discounting applied. The economic costs vary across countries due to relative population size and epidemiological indicators. FP = family planning; MNCH = maternal, newborn and child health; NCDs = non-communicable diseases.
Of the US1.4–6.7 billion were from cardiovascular diseases (52%), US0.2–1.1 billion were from diabetes (8%), and US$97–476 million were from mental disorders (4%). Differences between NCD subcategories were due to prevalence, age-standardized mortality rates and the impact of PHC in reducing mortality (Table 1).
Differences across countries
Out of the total economic cost of the PHC shock scenarios in the LAC, the largest share of costs was US1.8–9.4 billion from Mexico (25%), US0.5–2.6 billion from Argentina (7%), largely driven by population size (Fig. 3). The impact of each shock scenario as a proportion of GDP were more similar across countries (Fig. 4 and Supplementary Material, Appendix Figure F5), with the short and low magnitude scenario costing between 0.03 and 0.18% of countries' GDPs, the short and high magnitude scenario costing between 0.05 and 0.38% of countries' GDPs, the long and low magnitude scenario costing between 0.06 and 0.45% of countries' GDPs, and the long and high magnitude scenario costing between 0.12 and 0.92% of countries’ GDPs. The economic cost of PHC shocks was the highest as a percentage of GDP in Haiti (0.18%–0.92%) followed by Honduras (0.14%–0.75%).Fig. 4Economic cost of primary health care shocks as a percentage of the national GDP. 2023 GDP values were used; the economic cost in some countries may appear small relative to population size as not all intervention categories could be included for some of the smaller countries (Supplementary Material, Appendix A). The economic costs of the shocks are spread over many years but totals are shown as a percentage of annual GDP for contextualisation.
Sensitivity analyses
When additional stillbirths and neonatal deaths were considered as a result of the additional pregnancies (using country-specific stillbirth and neonatal mortality rates), this increased total stillbirths in the PHC shock scenarios from 600–3100 to 20,000–105,000 and neonatal deaths from 300–1400 to 23,000–122,000 (Supplementary Material, Appendix Figure F2). This increased the economic cost of the PHC shock scenarios from US15.0–76.8 billion (Appendix Figure F3). Including an assumed 5% reduction in disutility when NCD conditions are controlled increased the economic cost of the shock scenarios from US12.6–63.5billion over 2026–2030 (Appendix Figure F4).
Discussion
This study estimated the health and economic cost of potential future public health emergencies or large-scale shocks to PHC in the LAC region, as a proxy for the cost of inaction to strengthen PHC. The results suggest that events occurring between 2026 and 2030 that result in 25–50% relative reductions in PHC coverage, with recovery time ranging from one to five years, could lead to an additional 35,000–174,000 deaths (stillbirths, neonatal deaths, child deaths, maternal deaths and deaths due to NCDs), and 2.7–14.1 million unintended pregnancies across the 33 countries in the LAC region. These health impacts translate to cumulative societal economic costs of US$7.2–37.0 billion due to years of life lost and reduced workforce participation.
It is unknown when or what type of health system shocks will occur in the future, and so the range of scenarios considered have been designed to reflect a range of potential shocks. To put these in context, the large magnitude PHC shock scenarios are roughly consistent with observations reported in the LAC region during the COVID-19 pandemic. For example, in Brazil, which represents nearly one third of the population in the region, there was a 42.5% reduction in appointments with physicians55 and in Mexico and Argentina there were 59–63% and 46–69% reductions in consultations with children, respectively.10 In Mexico, family planning services fell by more than half during the first months of the pandemic,61 and in Chile, sexual and reproductive health consultations dropped by 47.3% in 2020 compared with the 2015–2019 average.6 Natural disasters or mass population movements could also have large effects; in 2018, the government of Colombia granted nearly 477,000 special stay permits to Venezuelan citizens in response to a mass migration.62 Some events could cross territorial borders: during economic and political crises in Venezuela, malaria cases resurged and neighbouring countries, such as Brazil, reported an increasing trend of imported cases.63 It is also possible that multiple health system shocks could occur together and in sequence, which would put further strain on the health system if proper planning and strengthening has not occurred.
The estimated societal economic costs of the PHC shock scenarios represent a lower bound, as they are based on a selection of services delivered through PHC only, and many additional impacts were not accounted for. First, the NCD model only captures mortality and not morbidity. This is because while disutility weights are available for different NCDs, there is limited evidence on the relative reduction in these disutility weights when PHC is accessed and/or the conditions are controlled. In a sensitivity analysis, the total economic cost of the PHC shock scenarios increased to US7.2–37.0 billion to US$15.0–76.8; Supplementary Material, Appendix Figure F3).
Most of the total impact came from countries with the largest population sizes; however, as a proportion of GDP the relative impacts were similar in each country. For example, Brazil, Mexico, Venezuela and Colombia represent 64% of the population from the 33 countries and accounted for 73% of the total economic costs of the PHC shock scenarios. As a proportion of GDP, the societal cost of these shock scenarios ranged from 0.03 to 0.18% in the short and low magnitude scenario to 0.12–0.92% in the long and high magnitude scenario. It is difficult to benchmark these estimates against data from COVID-19, where for example during the first year of COVID-19 pandemic aggregate GDP contracted by 7% in the LAC region,10 since this observed 7% includes the direct impacts of COVID-19, shocks to health services beyond PHC, and shocks to all other sectors.
Some components of this work can be compared against estimates relating service disruptions from COVID-19 to health outcomes. For example, Lara et al.11 estimated that a 28% reduction in non-COVID-19-related hospitalisations in Brazil, Ecuador, Mexico, and Peru could lead to a 15% increase in mortality rates compared with pre-pandemic years, with 89% of the mortality increase due to NCDs. When considering our short and low magnitude PHC shock scenario (25% reduction in PHC for one year) in just these four countries, and only considering maternal, newborn and NCD-related deaths to align with Lara et al.,11 our model estimates an excess ∼20,000 deaths (an ∼0.25% increase compared to no shock). However, it should be noted that Lara et al. consider hospitalisations for which health system shocks are more likely to have an immediate impact of mortality, whereas this study is considering PHC-delivered interventions only. In another study, UNFPA estimated that across 33 countries in the LAC region, a six-month moderate reduction to public sector utilization of modern contraceptives services could have led to 1.7 million additional unintended pregnancies, 2900 maternal deaths and 39,000 infant deaths.64 This is aligned with our modelled estimates of PHC shocks over a one to five year time frame leading to 2.7–14.1 million unintended pregnancies and 2100–11,300 maternal deaths.
This study did not consider actions required to strengthen PHC, but investment in PHC resilience will be necessary to reduce the impact of external shocks in the future. While it is possible that some crisis may lead to service disruptions even with increased PHC resilience, investments are likely to reduce the impact of disruptions and would additionally enhance health services even in the absence of these events. It has been recommended that to strengthen health system resilience overall investment is needed in health workforce, prevention, and key infrastructure.65 Policy interventions to expand fiscal space, improve revenue collection, enhance budgeting practices, optimize pooling funds and resource allocations, and establish efficient purchasing and payment systems for providers will be critical.10^,^65 Programmatically, system fragmentation will need to be reduced, and the benefits packages offered by PHC clearly defined. Infrastructure will also be required, including to strengthen the capacity of supply chains.8^,^65 This will take coordinated efforts across various government levels and sectors. Finally, accountability, transparency, and equitable resource allocations will be vital to ensure the long-term sustainability of PHC.
There are several limitations to this study. First, demographic and epidemiological data to parametrize the models for each country and service area were taken from a variety of sources, each with their own bias. Where possible, primary sources such as Demographic and Health Services or other large surveys were used, but in many cases model inputs were taken from the LiST model or Institute of Health Metrics and Evaluation databases (Appendix D), which are imputed or are the outputs of other models. For example, cause-specific mortality rates used for each country in the NCD model were estimates extracted from the Institute of Health Metrics and Evaluation rather than primary data, and are subject to limitations of their data processing methods. In addition, the relative Universal Health Coverage service index50 for each country was used as a proxy for both PHC coverage and the percentage of people with each NCD who had their disease “controlled” (Appendix Table D.6); it is unclear whether this is likely to be an underestimate or overestimate. Second, not all countries had all service domains considered in the analysis. For example, there was not enough data to model shocks to family planning, ANC, and vaccination services for 4/33 countries (12%), child health services for 21/33 countries (64%), and other pregnancy-related services for 18/33 countries (55%) (Appendix A); however, the missing data was mostly from countries with small populations and so is unlikely to have major impacts to the aggregate outcomes. Third, national models were used for each country, however there are likely to be geographical areas or population groups with limited baseline coverages (which would lead to overestimation of the impact of a shock), as well as increased fragility and limited capacities to recover from shocks (which would lead to underestimation of the impact of a shock). Fourth, the cause, timing and magnitude of future shocks is unknown, and so the PHC shock scenarios are theoretical and meant to reflect a range of possibilities rather than being specific to any type of event. We also modelled the shocks to begin in 2026 because the most recent data for each country is more reflective of 2026 than of future years, however in the absence of major changes to epidemiological indicators and interventions, the shocks are likely to have similar impacts if they occurred in future years. Fifth, the cost of strengthening PHC were not included in this modelling because they are currently unknown but should be a subject of further work.
Conclusion
The COVID-19 pandemic led to reductions in health service coverage and highlighted weaknesses in PHC systems in the LAC region. If another health system shock occurred that led to a 25–50% relative reduction in PHC service coverage with recovery time ranging from one to five years, then across the 33 countries in the LAC region this could lead to an additional 35,000–174,000 deaths (stillbirths, neonatal deaths, child deaths, maternal deaths and deaths due to NCDs) and 2.7–14.1 million unintended pregnancies, corresponding to US$7.2–37.0 billion in societal economic costs. Therefore, substantive investment in PHC resilience would be warranted if it could limit or eliminate the impact of shocks on service coverage.
Contributors
All authors conceived the study. TW and NS designed the model with inputs from PAVD, RMGS, MVU. TW implemented model scenarios. TW and NS analysed model outputs. PAVD, RMGS, MVU validated data inputs. TW and NS drafted the manuscript. All authors contributed to the final version of the manuscript. TW and NS have access to and have verified all data.
Data sharing statement
All model parameters used for this study are available in the manuscript and Supplementary Material, extracted from the sources as cited.
Editor's note
The Lancet Group takes a neutral position with respect to territorial claims in published maps and institutional affiliations.
Declaration of interests
The authors declare no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lim J.Broughan J.Crowley D.COVID-19's impact on primary care and related mitigation strategies: a scoping review Eur J Gen Pract 27120211661753428269510.1080/13814788.2021.1946681 PMC 8293960 · doi ↗ · pubmed ↗
- 2Chmielewska B.Barratt I.Townsend R.Effects of the COVID-19 pandemic on maternal and perinatal outcomes: a systematic review and meta-analysis Lancet Glob Health 202192021 e 759e 77210.1016/S 2214-109X(21)00079-6PMC 801205233811827 · doi ↗ · pubmed ↗
- 3Alabi Q.K.Oyedeji A.S.Kayode O.O.Kajewole-Alabi D.I.Impact of COVID-19 pandemic on mother and child health in Sub-Saharan Africa – a review Pediatr Res 942023127812833720252910.1038/s 41390-023-02651-w PMC 10193350 · doi ↗ · pubmed ↗
- 4World Health Organization (WHO)In WHO global pulse survey, 90% of countries report disruptions to essential health services since COVID-19 pandemic 2020 WHO Geneva Available from:https://www.who.int/news/item/31-08-2020-in-who-global-pulse-survey-90-of-countries-report-disruptions-to-essential-health-services-since-covid-19-pandemic
- 5Langlois E.V.Mc Kenzie A.Schneider H.Mecaskey J.W.Measures to strengthen primary health-care systems in low- and middle-income countries Bull World Health Organ 98202078191|3317777510.2471/BLT.20.252742 PMC 7607465 · doi ↗ · pubmed ↗
- 6Savedoff W.Bernal P.Distrutti M.Goyeneche L.Bernal C.Going beyond normal: challenges for health and healthcare in Latin America and the Caribbean exposed by COVID-192022
- 7Herrera C.A.Kerr A.C.Dayton J.M.Kakietek J.J.Healthcare service disruption in 14 Latin American and Caribbean countries during the COVID-19 pandemic: analysis of household phone surveys, 2020-2021 J Glob Health 136023202310.7189/jogh.13.06023 PMC 1035975937469284 · doi ↗ · pubmed ↗
- 8OECD Primary health care for resilient health systems in Latin America. OECD health policy studies 2022 OECD Publishing Paris