Mid-term Outcomes in Primary Roux-en-Y Gastric Bypass Procedures with Short or Long Biliopancreatic Limb
Julian Süsstrunk, Svenja Erne, Alexander Wilhelm, Thomas Köstler, Diana Mattiello, Urs Zingg

TL;DR
This study compares mid-term outcomes of gastric bypass surgery with short or long biliopancreatic limbs, finding similar weight loss but better blood sugar control with longer limbs.
Contribution
The study provides new mid-term clinical evidence comparing short and long biliopancreatic limb lengths in Roux-en-Y gastric bypass surgery.
Findings
Long-BPL RYGB showed accelerated weight loss in the first year but no significant difference after two years.
Short-BPL RYGB had a slightly higher T2D remission rate, though not statistically significant.
Long-BPL RYGB resulted in greater HbA1c reduction after two years.
Abstract
This study reports mid-term results on weight loss and T2D remission in patients undergoing Roux-en-Y gastric bypass (RYGB) with short versus long biliopancreatic limb (BPL). All patients with obesity undergoing RYGB procedures with long BPL (150 cm) versus short BPL (60 cm) between 2016 and 2021 at a tertiary reference center for bariatric surgery were compared using propensity score matching to assess for T2D remission, HbA1c evolution, weight loss and nutritional deficiencies. A total of 165 patients were included, 69 patients (71% female, mean age 43.9 ± 14 years, mean baseline BMI 42.4 ± 4.3 kg/m2, mean HbA1c 6.75 ± 1.9%) underwent long-BPL RYGB and 96 patients (76% female, mean age 43.1 ± 12 years, mean baseline BMI 41.7 ± 3.5 kg/m2, mean HbA1c 5.97 ± 1.1%) had a short-BPL. In long-BPL RYGB weight loss was more accelerated after 1 year, but did not differ after 2 years compared…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
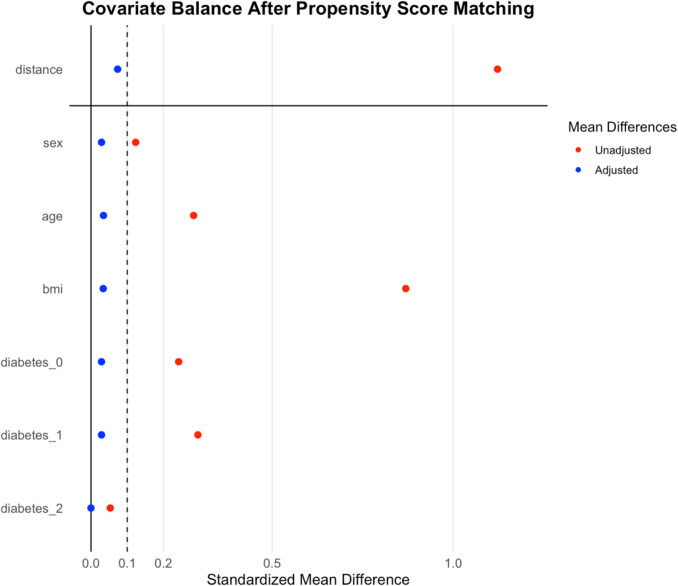 Figure 1
Figure 1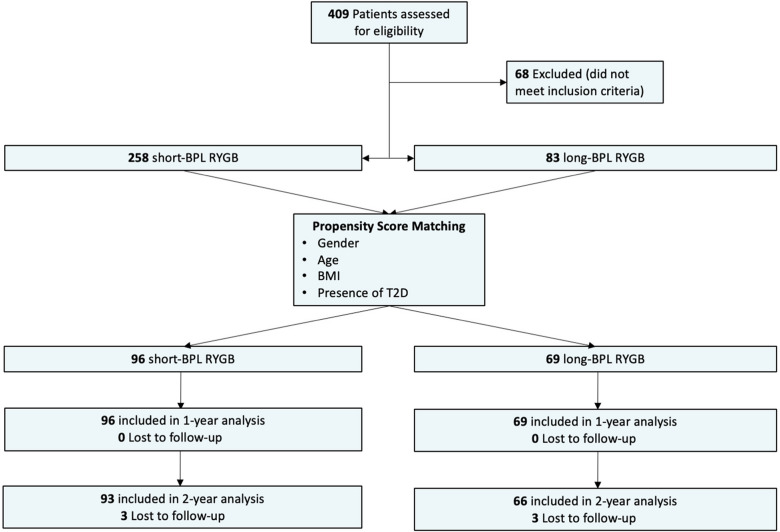 Figure 2
Figure 2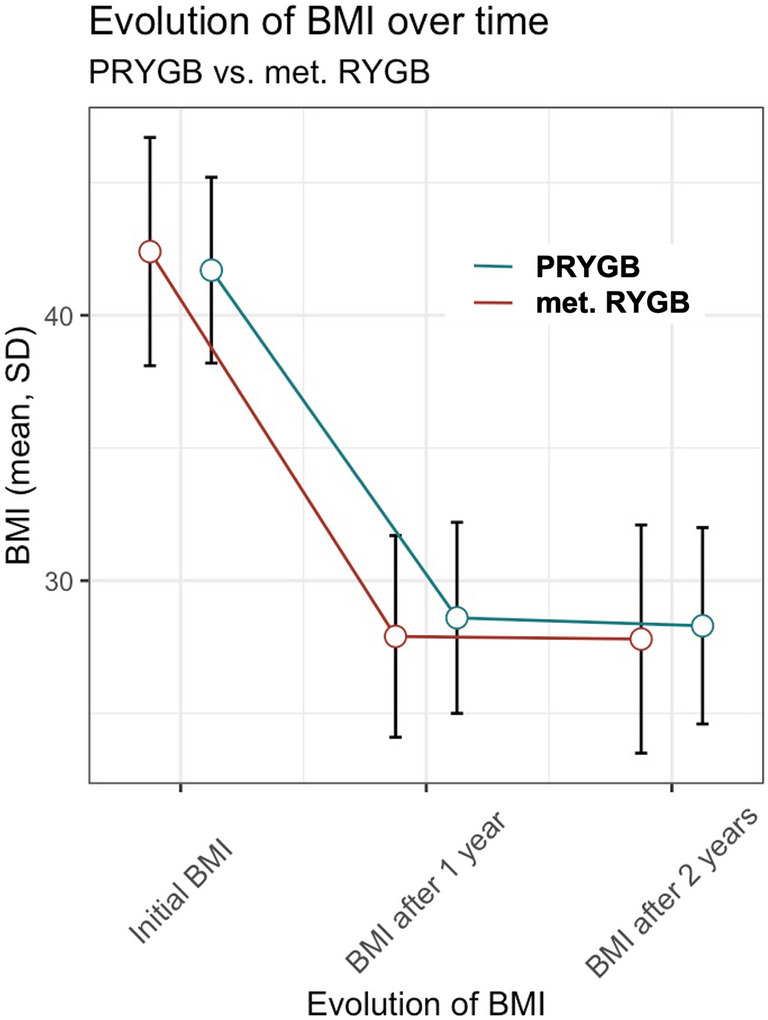 Figure 3
Figure 3- —University of Basel
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBariatric Surgery and Outcomes · Esophageal and GI Pathology · Diabetes Treatment and Management
Introduction
The prevalence of obesity has dramatically increased over the last decades, affecting individuals across all age groups [1]. Sleeve gastrectomy (SG) is the most frequently performed bariatric procedure, followed by Roux-en-Y gastric bypass (RYGB) and one anastomosis gastric bypass (OAGB) [2]. In the context of obesity, type 2 diabetes mellitus (T2D) is a relevant associated medical condition due to its associated long-term complications. Its prevalence is increasing in correlation with the prevalence of obesity [3]. A landmark study comparing metabolic bariatric surgery (MBS) with conventional medical treatment demonstrated that RYGB and biliopancreatic diversion (BPD) were more effective in achieving long-term control of T2D compared to best medical treatment [4]. When looking at the most commonly performed procedure SG, a randomized trial by Svanevik et al. reported inferior outcomes regarding weight loss and remission of T2D three years after SG compared to RYGB [5]. Moreover, SG seems not only inferior in terms of weight loss and HbA1c reduction, but also in the reduction of associated cardio-vascular conditions and remission of dyslipidemia in patients with T2D [6, 7].
Although RYGB is the preferred procedure in patients with obesity and T2D, the limb lengths in RYGB regarding optimal control of T2D and weight loss remain controversial [8]. Increased length of the biliopancreatic limb (BPL) in RYGB improved the anti-diabetic effect and resulted in enhanced weight loss. The rationale for lengthening the BPL instead of the Roux limb (RL) is based on findings, that bypassing more proximal small bowel leads to enhanced secretion of incretin hormones, such as glucagon-like-peptide 1 (GLP-1) and peptide tyrosine tyrosine (PYY) [9]. These changes, in conjunction with increased circulating bile acid concentrations, are considered key mechanisms contributing to improved glycemic control and weight loss after RYGB [10–12]. However, most previous studies reported only short-term outcomes and had variable definitions for the length of the BPL [13–16]. The lengthening of the BPL is desirable concerning the weight loss and T2D resolution. However, it may come at the cost of potential nutritional side effects.
The optimal limb lengths for patients with T2D have not been determined yet and the investigation on BPL length for optimal weight loss and improvement of obesity-related conditions is of importance. Thus, the aim of this study was to report on mid-term weight loss outcomes and T2D evolution of patients undergoing RYGB with a standard versus a long BPL.
Methods
Design and Patients
Data of all patients undergoing a bariatric procedure at the XXX (blinded), is entered into a prospective database. For this retrospective, non-randomized, matched case cohort study, all patients undergoing laparoscopic RYGB between January 2016 and December 2021 were analyzed. Patients with previous bariatric procedures such as adjustable gastric banding or SG were excluded. To assess the effect of variable BPL lengths, patients were divided into two groups: Short-BPL RYGB consisted of a BPL of 60 cm and a Roux limb of 150–200 cm. Long-BPL RYGB consisted of a BPL of 150 cm and a RL of 100–150 cm.
Preoperative Assessment, Surgical Technique, and Perioperative Care
All patients were assessed preoperatively by a multidisciplinary team according to the guidelines of the Swiss Multidisciplinary Obesity Society (SMOB). Preoperative evaluation included upper endoscopy with biopsy, abdominal ultrasound and assessments by dieticians, endocrinologists, cardiologists, psychologists and pulmonologists, respectively.
Selection of the procedure was dependent on the outcome of the bariatric multidisciplinary team discussion as well as the expectations and wishes of the patients. All patients with T2D, regardless of preoperative BMI, were evaluated for a long-BPL RYGB.
Both short and long-BPL RYGB were performed using a six-port technique. A small gastric pouch (approx. 40–50 cc) was created and an antecolic circular or linear stapled gastro-enterostomy was formed. In short-BPL RYGB the RL measured 150–200 cm and in long-BPL RYGB 100–150 cm. Intraoperative measurement of the limb lengths was performed using the length of the gaspers’ end (approx. 30 mm) as a reference for laparoscopic measuring. With a side-to-side, linear stapled entero-enterostomy, a BPL of 60 cm in short-BPL RYGB and 150 cm in long-BPL RYGB was fashioned. Total bowel length or common channel length was not measured routinely. Mesenteric defects were closed with non-resorbable sutures in all procedures.
Independent of the procedure choice, the patients received equal postoperative multivitamin, calcium and vitamin D supplementation in the beginning, adjusting the dose according to blood tests during the follow-up visits. These regular postoperative follow-up visits were scheduled after 6 weeks, 6 months, 12 months and yearly thereafter.
Outcome Measures
The primary outcome was weight loss expressed as percentage total weight loss (%TWL) calculated as follows: [(initial weight) − (postoperative weight)]/[(initial weight)].
Secondary outcomes were weight loss expressed as reduction of BMI, T2D remission, defined as HbA1c value of 5.6% or less, without the use of any antidiabetic medication, a stricter definition as the one proposed by the American Diabetes Association [17]. For the current study, we differentiated between prediabetes with a HbA1c value ranging from 5.7% up to 6.4% and T2D, defined by a HbA1c value of 6.5% or higher. Further secondary outcomes were percentage reduction of HbA1 value (ΔHbA1c; (initial HbA1c − postoperative HbA1c) in %), malnutrition (serum albumin < 35 g/L), vitamin and substrate deficiencies. Additionally, presence of obesity-related conditions such as arterial hypertension (AT) (systolic blood pressure > 140 mmHg with/without use of antihypertensive medication), sleep apnea confirmed by a pulmonologists examination, coronary heart disease confirmed by a cardiologist’s examination, peripheral artery disease (PAD) confirmed by a vascular specialists examination and hyperlipidemia (Cholesterol > 6.2 mmol/L, triglycerides > 1.2 mmol/L) were assessed. Analysis of vitamin and substrate deficiencies included vitamin A (< 0.3 mg/L), Vitamin D (< 31 \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mu$$\end{document} g/L), Vitamin B1 (< 33.1 \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mu$$\end{document} g/L), B6 (< 12.6 \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mu$$\end{document} g/L) and B12 (< 145 pmol/L), holotranscobalamin (< 37.5 pmol/L), zinc (< 9 \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mu$$\end{document} mol/L), albumin corrected calcium (< 2.15 mmol/L), hypoproteinemia (serum prealbumin < 200 mg/L), ferritin (< 13 \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mu$$\end{document} g/L) and folic acid in erythrocytes (< 523 \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\mu$$\end{document} g/L). Moreover, use of vitamin and/or substrate supplementation preoperatively and use of supplementation exceeding the routinely administered supplementation dosage postoperatively also counted as a deficiency.
Statistical Analysis
Data are presented either as mean ± standard deviation or, in the case of proportions, as numbers (%). Differences between groups were compared using the two sample t test for continuous data and Pearson’s Chi-square test for categorical data. No formal corrections for multiple comparisons were applied, consistent with recommendations for exploratory analyses. Normality of continuous variables was visually assessed using histograms and Q–Q plots.
To account for differences between groups, patients underwent propensity score matching using the following matching criteria: sex, age, body mass index (BMI) and presence of Type 2 Diabetes. Propensity scores were estimated via logistic regression, and 1:2 nearest-neighbor matching without replacement was applied using a caliper width of 0.2 standard deviations of the logit of the propensity score. Since this study is a retrospective analysis of a prospectively maintained clinical database, a complete-case-analysis approach was used ensuring that only complete datasets were included in the analysis.
A p value of 0.05 was considered significant. A formal power calculation was not performed, and the sample size was determined by the number of patients meeting the inclusion criteria during the study period. All statistical analyses were performed using R Programming language (version 4.4.1, R Core Team 2024).
Results
Patient Characteristics
To maximize comparability, a 1:2 matching ratio was used, resulting in 69 long-BPL RYGB patients (71% female, mean age 43.9 ± 14 years, mean baseline BMI 42.4 ± 4.3 kg/m^2^) being matched to 96 short-BPL RYGB patients (76% female, mean age 43.2 ± 12 years, mean baseline BMI 41.7 ± 3.5 kg/m^2^). The remaining unmatched patients were excluded from the matched analysis. Balance diagnostics demonstrated standardized mean differences <0.1 for all matched covariates, indicating excellent covariate balance (Figure 1). The propensity score itself (“distance”) showed a post-matching standardized mean difference of 0.074, further supporting the adequacy of the matching procedure. Short-BPL RYGB consisted of a BPL of 60 cm and a Roux limb (RL) of 150–200 cm. Long-BPL RYGB consisted of a BPL of 150 cm and a RL of 100–150 cm. Therefore, total bypassed limb length was comparable in both groups (210–260 cm versus 250–300 cm respectively). There were no significant differences between the groups concerning gender, age or preoperative BMI. Figure 2 displays the cohort after matching and provides information on follow-up data. All 165 operations were performed laparoscopically; no conversion to open surgery occurred. In the short-BPL RYGB group, 34% had a T2D and 16% had a prediabetes, compared to 45% and 14% in the long-BPL group (p = 0.38). Forty-three percent of patients used antidiabetic drugs in the long-BPL group compared to 27% in the short-BPL group (p = <0.001). Baseline HbA1c levels were 6.75 ± 1.9 and 5.97 ± 1.1 in the long- and short-BPL group, respectively (p = 0.001). Detailed information on comorbidities and baseline laboratory results are shown in Table 1.Fig. 1. Covariate balance after propensity score matchingFig. 2Flow chart describing patient selectionTable 1Baseline characteristicsShort-BPL RYGB (n = 96)Long-BPL RYGB (n = 69)p valuePatient sex0.47 Female73 (76%)49 (71%) Male23 (24%)20 (29%)Age at operation, year, mean (SD)43.15 (12.14)43.88 (13.71)0.72Baseline weight, kg, mean (SD)114.83 (15.12)119.249 (17.29)0.083Baseline BMI, kg/m^2^, mean (SD)41.68 (3.50)42.43 (4.33)0.22Excess weight, kg, mean (SD)45.84 (10.46)48.93 (12.74)0.090Baseline albumin deficiency0 (0%)0 (0%)Baseline ferritin deficiency2 (2%)2 (3%)0.74Baseline hypo- vs. hyperthyroidism0.35 Hypothyroidism1 (1%)0 (0%) Hyperthyroidism0 (0%)1 (1%)Baseline folic acid in erythrocytes deficiency3 (3%)4 (6%)0.38Baseline calcium deficiency8 (8%)4 (6%)0.54Baseline zinc deficiency3 (3%)2 (3%)0.92Baseline vitamin B12 deficiency0 (0%)0 (0%)Baseline holotranscobalamin deficiency6 (7%)6 (9%)0.54Baseline vitamin A deficiency1 (1%)1 (2%)0.80Baseline vitamin D3 deficiency89 (95%)67 (97%)0.45Baseline vitamin B1 deficiency0 (0%)0 (0%)Baseline vitamin B6 deficiency49 (55%)34 (54%)0.89Baseline Diabetes0.38 Prediabetes33 (34%)31 (45%) Diabetes15 (16%)10 (14%)Baseline HbA1c, mean (SD)5.97 (1.09) %6.75 (1.89) %0.001Baseline diabetes drugs < 0.001 OAD23 (24%)12 (17%) OAD + insulin1 (1%)5 (7%)Insulin2 (2%)13 (19%)Baseline hypertension41 (43%)40 (59%)0.042Baseline hypertension drugs35 (36%)32 (46%)0.20Baseline coronary heart disease6 (6%)5 (7%)0.80Baseline PAD1 (1%)1 (1%)0.81Baseline hyperlipidemia34 (35%)31 (45%)0.22Baseline hyperlipidemia drugs16 (17%)14 (20%)0.55Baseline OSAS44 (46%)40 (58%)0.12Baseline CPAP therapy14 (15%)16 (23%)0.16() = % if not otherwise statedRYGB Roux-en-Y gastric bypass, BMI body mass index, OAD oral antidiabetics, PAD peripheral artery disease, OSAS obstructive sleep apnea syndrome, CPAP continuous positive airway pressure. SD standard deviation
BMI Changes and Total Weight Loss
Data on postoperative weight loss are shown in Table 2. After 1 year, %TWL was 31.57 ± 7.66% in the short-BPL RYGB group and 33.86 ± 9.43% in the long-BPL RYGB group (p = 0.088), and after 2 years 32.04 ± 8.83% in the short-BPL RYGB group and 33.78 ± 9.75% in the long-BPL RYGB group (p = 0.242). At 1-year follow-up, the mean weight loss was significantly higher in the long-BPL group with 44.8 ± 33.1 kg compared to 36.4 ± 10.5 kg in the short-BPL RYGB group (p = 0.021). After 2 years, this difference was not significant anymore (36.9 ± 11.5 kg in the short-BPL RYGB group and 40.3 ± 13.3 kg in the long-BPL RYGB group, p = 0.092). Figure 3 illustrates the evolution of the BMI over time in the two groups, demonstrating an accelerated BMI reduction in the long-BPL RYGB group. Table 2. Weight loss parameters over the study periodShort-BPL RYGB (n = *96)*Long-BPL RYGB (n = 69)p valueWeight loss/BMI changes at 1 year BMI (kg/m^2^)28.57 (3.58)27.86 (3.81)0.22 Weight (kg)78.48 (12.9)78.83 (15.99)0.87 Weight loss (kg)36.42 (10.53)44.85 (33.14)0.021 BMI reduction (kg/m^2^)13.12 (3.85)14.58 (4.58)0.028 TWL (%)31.57 (7.66)33.86 (9.43)0.088Weight loss/BMI changes at 2 years BMI (kg/m^2^)28.3 (3.7)27.82 (4.3)0.46 Weight (kg)77.96 (13.74)78.86 (16.88)0.71 Weight loss (kg)36.9 (11.51)40.25 (13.32)0.092 BMI reduction (kg/m^2^)13.42 (4.06)14.49 (4.95)0.139 TWL (%)32.04 (8.83)33.78 (9.75)0.242Values are shown as median (standard deviation)BMI body mass index, %TWL total weight lossFig. 3Evolution of BMI over time; p value 1 year postoperative = 0.028, p value 2 years postoperative = 0.139; sample size 1 year postoperative: short-BPL n = 96, long-BPL n = 69; sample size 2 years postoperative: short-BPL n = 93, long-BPL n = 66
Remission of Type 2 Diabetes and Evolution of Hba1c Levels
Data on postoperative T2D are shown in Table 3. At 1-year follow-up, T2D was present in 7% and in 17% in the short-BPL and long-BPL groups, respectively. Prediabetes occurred in 8% of patients in the short-BPL RYGB group compared to 3% in the long-BPL RYGB group. After 2 years follow up, 5% of patients still had a T2D and 9% a prediabetes after short-BPL RYGB compared to 14% and 9% in the long-BPL RYGB group. This corresponds to a remission rate of 61.3% in the short-BPL RYGB group and 53.3% in the long-BPL RYGB group, respectively (p = 0.53). Discontinuation of antidiabetic drugs at 1 year follow up was observed in 88.5% in the short-BPL RYGB and in 70% in the long-BPL RYGB group (p = 0.092). At the 2-year follow-up, the discontinuation rates were 91.7% and 72.4 %, respectively (p = 0.075). Table 3. Diabetes parameters over the study periodShort-BPL RYGB (n = *96)*Long-BPL RYGB (n = *69)*p valueDiabetes changes at 1 yearDiabetes/prediabetes0.06 Diabetes (%)7 (7%)12 (17%) Prediabetes (%)8 (8%)2 (3%)HbA1c (%)5.16 (0.71)5.25 (0.7)0.43ΔHbA1c (%)0.79 (1.05)1.5 (1.69)0.001Diabetes drugs0.086 OAD (%)2 (2%)7 (10%) Insulin (%)1 (1%)2 (3%)Diabetes changes at 2 yearsDiabetes/prediabetes0.19 Diabetes (%)5 (5%)9 (14%) Prediabetes (%)8 (9%)6 (9%) HbA1c (%)5.22 (0.5)5.28 (0.82)0.60 ΔHbA1c (%)0.72 (0.92)1.51 (1.73) < 0.001Diabetes drugs0.031 OAD (%)2 (2%)6 (9%) Insulin (%)0 (0%)2 (3%)Values are shown as mean (standard deviation)OAD oral antidiabetic drugs
Considering that the preoperative HbA1c levels were significantly higher in the long-BPL RYGB group compared to the short-BPL RYGB group, ΔHbA1c was additionally analyzed postoperatively. At 1-year follow-up, ΔHbA1c was significantly lower in the short-BPL RYGB group (0.79 ± 1%) compared to the long-BPL RYGB group (1.5 ± 1.7%, p = 0.001). This significant difference persisted at 2-year follow-up with a short-BPL RYGB ΔHbA1c of 0.71 ± 0.9% and long-BPL RYGB ΔHbA1c of 1.5 ± 1.7% (p < 0.001). However, mean HbA1c levels at 1-year follow up were 5.16 ± 0.71% in the short-BPL group and 5.25 ± 0.7% in the long-BPL group (p = 0.43). HbA1c levels at the 2-year follow up were 5.22 ± 0.5% and 5.28 ± 0.82% (p = 0.60) respectively. This indicates no significant difference in glycemic control despite a greater reduction in the long-BPL group.
Resolution of Obesity-Related Medical Conditions and Nutritional Deficiencies
No difference in the resolution of the various obesity-related medical conditions was detected between the groups. Resolution of arterial hypertension (AT) occurred in 71% in the short-BPL RYGB group and in 68.4% in the long-BPL RYGB group (p = 0.8). Resolution of hyperlipidemia was observed in 81.3% in the short-BPL RYGB group and in 80% in the long-BPL RYGB group (p = 0.9). Obstructive sleep apnea syndrome (OSAS) was eliminated in 92.9% of the short-BPL RYGB patients and in 87.2% of the long-BPL RYGB patients (p = 0.392).
Malnutrition occurred in two patients at 2-year follow-up, both with a long-BPL RYGB. With an albumin of 31 g/L and 33 g/L respectively, neither patient required inpatient treatment (p = 0.091).
An overview of the comparison of vitamin and substrate deficiencies at the 2-year follow-up is demonstrated in Table 4. There was a significant difference in the incidence of zinc deficiency with 22% of patients following short-BPL RYGB and in 41% of patients after long-BPL RYGB, respectively (p = 0.009). There was no significant difference among all other vitamin and substrate deficiencies between groups. Table 4. Nutritional parameters at 2-year follow-upShort-BPL RYGB (n = *96)*Long-BPL RYGB (n = *69)*p valueAlbumin deficiency0 (0%)2 (3%)0.091Ferritin deficiency34 (37%)25 (38%)0.87Hypo- vs. hyperthyroidism0.23 Hypothyroidism4 (4%)6 (9%) Hyperthyroidism0 (0%)1 (2%)Deficiency of folic acid in erythrocytes5 (5%)3 (5%)0.81Calcium deficiency13 (14%)13 (20%)0.34Zinc deficiency20 (22%)26 (41%)0.009Holotranscobalamin deficiency27 (30%)21 (32%)0.72Vitamin A deficiency4 (5%)6 (10%)0.22Vitamin D3 deficiency64 (69%)53 (80%)0.11Vitamin B1 deficiency2 (2%)1 (2%)0.79Vitamin B6 deficiency16 (17%)11 (17%)0.99() = %
Length of Hospital Stay and Complications
No death related to bariatric surgery occurred during the entire follow-up. One patient died 2 years and 9 months postoperative due to hepatocellular carcinoma unrelated to surgery. In most cases hospital stay ranged from 2 to 4 days. Longest hospital stay was 44 days due to complications including bleeding from the entero-enterostomy, backlog of the BPL, aspiration pneumonia, and pulmonary embolism necessitating 18 days of ICU care. An overview of the postoperative complications classified by Clavien-Dindo of at least grade IIIa is shown in Table 5. Fifteen patients (15.6%) had a grade 3a or higher complication after short-BPL RYGB and 19 patients (27.5%) after long-BPL RYGB (p = 0.095). Table 5. Overview of postoperative complications classified by Clavien-DindoComplicationClavien-Dindo gradeNotesPatients (n)Short-BPL (n)Long-BPL (n)Time frame < 30 days Abdominal pain with preoperative diagnosis of cholecystolithiasis and intraoperative diagnosis of an adhesive bandIIIbLaparoscopic adhesiolysis and laparoscopic cholecystectomy11 Douglas abscessIIIbLaparoscopic abscess drainage11 Leak of the entero-enterostomyIIIbLaparoscopic revision of the entero-enterostomy11 Wound abscessIIIaTreated with antibiotics and CT-guided drainage11 Bleeding from the stapler line on the residual stomachIIIbLaparoscopic hemostasis11 Entero-enterostomy bleeding with backlog in the BPL leading to perforation of the residual stomachIVaLaparoscopic hemigastrectomy, enterostomy, revision of the entero-enterostomy and abdominal lavage11 Bleeding of the entero-enterostomy with backlog of the BPL followed by aspiration pneumonia and pulmonary embolism necessitating ICU-CareIVbLaparoscopic revision of the entero-enterostomy and intraoperative Gastroscopy11Time frame > 30 days Chronic/recurrent anastomotic ulcerIIIbLaparoscopic revision of the gastro-enterostomy633 Ulcer bleedingIIIbLaparoscopic formation of an esophago-jejunostomy11 Bleeding in the residual stomach caused by recurrent ulcers in the antrumIIIbLaparoscopic assisted gastroscopy and gastrectomy of the residual stomach11 Stenosis of the gastro-enterostomyIIIaManaged endoscopically by bougienage11 Gastro-gastric fistulaIIIbLaparoscopic revision of the gastro-enterostomy with partial resection of the gastric pouch and resection of the gastric fundus11 Jejunal ulcer distal to the gastro-enterostomyIIIbLaparoscopic revision of the gastro-enterostomy11 Symptomatic cholecystolithiasisIIIbLaparoscopic cholecystectomy22 Internal hernia of Petersen’s space with/without incarcerationIIIbReposition of the bowel and closure of the hernia with/without segmental resection of the small bowel615 Diffuse abdominal pain due to (partially) open intermesenteric defectsIIIbClosure of the intermesenteric defects33 Diffuse abdominal pain related to cholecystolithiasis and adhesive bandsIIIbLaparoscopic adhesiolysis and cholecystectomy11 Diffuse abdominal pain related to kinking and dilation of the entero-enterostomyIIIbLaparoscopic revision of the entero-enterostomy11 Perforation of the entero-enterostomy related to a bezoarIIIbOpen revision of the entero-enterostomy11 Incisional herniaIIIbOpen hernia reposition and sublay mesh repair with partial component separation11 Adhesive small bowel obstructionIIIbLaparoscopic adhesiolysis11 Total (n)34 (20.6)15 (15.6)19 (27.5)() = %; p = 0.095
Discussion
Our study revealed no significant difference in weight loss outcomes between short-BPL RYGB and long-BPL RYGB at 2 years with a %TWL of 32.04 ± 8.83% and 33.78 ± 9.75%, respectively. However, in the long-BPL group, the weight loss was more accelerated in the first year. Regarding T2D remission, we observed no significant difference at 2 years in both groups despite more patients with insulin-dependent T2D and higher HbA1c levels preoperatively in the long-BPL group. Nevertheless, the long-BPL RYGB was associated with an improved metabolic response, reflected in a greater decrease in ΔHbA1c. Hence, a longer BPL facilitates a greater drop in blood sugar levels in patients with poorer initial glycemic control. However, no significant difference was observed in HbA1c levels at 1 and 2 years.
These findings suggest that the BPL may be elongated even more to increase the weight loss and improve the resolution of obesity-related medical conditions especially T2D. However, before changing limb lengths arbitrarily it is crucial to understand the altered gastrointestinal physiology after bariatric surgery. The RYGB is widely known to induce weight loss and remission of obesity-related medical conditions through a combination of gastric restriction and intestinal bypass that alters nutrient absorption and gut signaling. More recent literature evaluates different mechanisms in gastrointestinal physiology leading to these effects. Among other factors, elevated bile acid levels and altered release of gut hormones are identified as contributors to an increased effectiveness of bariatric surgery [18, 19]. The gut hormone glucagon-like-peptide 1 (GLP-1), which is released postprandially by L-cells in the ileum, is assumed to play a key role in improved postoperative glucose tolerance via the incretin effect [10]. Furthermore, by different pathways, GLP-1 superiorly acts as a satiety hormone, hence leading to weight loss [20]. The same effects are seen in GLP-1 receptor agonists administration in treatment of obesity and T2D [21, 22]. GLP-1 secretion and also peptide tyrosine tyrosine (PYY) secretion, another incretin, are elevated in any situation of accelerated gastric emptying and rapid transport of undigested nutrients to a more distal part of the small intestine, such as it is the case in RYGB patients [9]. Further data from a rat model highlighted the essential contribution of PYY-release on GLP-1 secretion [23]. In regard to serum bile acids, their levels are also elevated following RYGB [24]. It is hypothesized that elevated bile acid levels lead to an improved glycemic control. However, the exact underlying mechanisms are poorly understood [11]. By elongating the BPL, a rise in GLP-1 levels could be demonstrated in humans and rat models [25, 26]. Furthermore, concentrations of serum bile acids also seem to be increased with a longer biliopancreatic limb [11].
Taking our results in light of the current aforementioned literature, the long BPL achieves faster weight loss, even though the total bypassed bowel length (BPL + Roux limb) stayed more or less the same in both groups at approximately 250–260 cm. Furthermore, a better outcome with regard to the reduction of the HbA1c level could be observed. However, no significant difference in the T2D remission rate was observed between the two groups. To gain a higher percentage of T2D remission, a further lengthening of the BPL needs to be considered. In a study conducted by Zerrweck et al. the BPL was lengthened up to 200 cm. In the short-term follow up of 12 months, weight loss (% EWL) and reduction of HbA1c levels were increased in comparison to a short BPL of 50 cm [14]. However, similar to our results, the clinical remission rate of T2D was comparable between groups, and the effect was only seen in the significantly higher decrease of HbA1c levels. Unfortunately, the study lacked long-term results. Another analysis of a 200 cm BPL demonstrated improved metabolic outcomes compared to BPL with a length of 84 ± 2 cm, reflected by higher T2D remission and lower antidiabetic drug requirement [27].
A potential factor influencing T2D remission rate is the duration of the disease at the time of bariatric surgery, and the time of its onset. In a short-term follow-up, a better glycemic control was achieved with gastric bypass procedures in patients with an early-onset T2D (<40 years of age) compared to patients with a late-onset T2D (≥40 years of age) [28]. Factors predicting a poorer postoperative T2D outcome are age over 40 to 50 years, higher HbA1-levels and insulin-use. Also, a higher BMI indicates a higher probability of T2D remission [29]. Moreover, longer T2D duration is a poor predictor for remission. However, it remains unclear at what level the threshold for a better postoperative outcome should be set at [30, 31]. Unfortunately, our data set did not allow to analyze the time frame of T2D onset and duration.
According to the American Society of Metabolic and Bariatric Surgery (ASMBS) and the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO), MBS is generally recommended in patients with a BMI ≥ 35kg/m^2^, whereas in patients with T2D it’s already recommended with a BMI of ≥30kg/m^2^ [32]. Based on our results and the actual literature, the conclusion that a longer BPL induces accelerated weight loss and improved T2D control without relevantly triggering malnutrition is sound. From a clinical perspective, the accelerated initial weight loss observed after long-BPL RYGB may be relevant in selected patient groups. Patients with poorly controlled T2D, a high insulin dose requirement, advanced cardiovascular risk or severe obesity could benefit from more rapid metabolic improvement. Furthermore, Silveira et al. demonstrated, that TWL of <10% at 3 months is associated with suboptimal weight loss at 1 year [33]. Despite the absence of a significant difference in weight loss in our study population at the 2-year follow-up, these early advantages may justify the use of a longer BPL in carefully chosen patients. However, long-term RCTs are required to confirm whether such patient stratification should be systematically implemented in daily practice.
The adverse effects like diarrhea did not differ between the two BPL groups. Malnutrition was rare. Zinc deficiency was the only nutritional deficiency that was significantly higher in the long-BPL RYGB group compared to the short-BPL group. Zinc absorption occurs in the proximal small bowel by zinc transporters, which are regulated by multiple factors [34]. Lengthening of the BPL leads to a longer bypass of the proximal small bowel, which explains this higher rate of zinc deficiency in long-BPL RYGB. A study conducted by Thereaux et al. demonstrated increased late adverse events such as higher nutritional disorders in RYGB and SG compared to a control group, however in favor of a decreased 7-year overall mortality [35]. Data on nutritional deficiencies in patients with different lengths of the BPL are scarce and partially contradicting. Zerrweck et al. found no difference in hemoglobin or albumin levels as indirect parameters for malnutrition [14]. In contrast, Nergaard et al. reported significantly higher requirements for supplementation of vitamin D, iron and calcium citrate in a long BPL of 200cm compared to a short BPL of 60 cm with a follow-up up to 7 years [36]. Given that nutritional deficiencies can be monitored and supplemented, bariatric surgery is associated with better long-term outcomes than medical treatment for obesity. A longer BPL in RYGB should be considered as it may further improve outcomes concerning weight loss and resolution of obesity-related conditions. However, it should be recognized that the follow-up and nutritional monitoring of RYGB patients, especially if a longer BPL is used, must be performed over a long-time if not life-long.
Limitations of this study consist of the retrospective nature and the mid-term follow-up of 2 years. However, all data were collected prospectively and, due to the propensity score matching, the two groups were comparable at baseline. The sample size of 165 patients may have been insufficient to detect smaller but clinically relevant differences, such as in the T2D remission rate. Since no a priori power calculation was performed and sample size was determined by patient availability, the risk of type II errors must be considered. Therefore, non-significant findings should not be interpreted as equivalence. The values and findings remained stable between the 1 and 2-year follow-up. Unfortunately, onset and duration of T2D were not assessed in the study population. The 2-year follow-up of the present study is longer than in most other reports discussing different BPL lengths. Furthermore, the rate of patients lost to follow-up was exceptionally low. However, studies with long-term follow-up over several years are of interest because differences in weight loss, diabetes remission and nutritional deficiencies are assumed to occur only over a longer time period. The systematic review and meta-analysis by Rizvi et al. emphasize this point [37]. As this is not a randomized study, a certain selection bias could affect the results. Patients with a higher HbA1c level and insulin-dependency were more likely selected for a long-BPL RYGB. Although propensity score matching accounted for the presence of T2D and prediabetes, it did not include HbA1c levels or insulin dependency. These remaining differences may have influenced glycemic outcomes. Therefore, one needs to interpret postoperative results on HbA1c changes with caution. Furthermore, we did not specifically analyze outcomes within subgroups due to the matched cohort design and limited sample size. Other limitations include that the total bowel length was not measured, so anatomical differences were not accounted for. Additionally, there was no difference in diarrhea between the two groups. However, no formal Quality of Life (QoL) or gastrointestinal symptom analysis was performed. Finally, as this was a single-center study, the results may not be generalizable to all populations or surgical settings. Nevertheless, our findings align with those of other published studies, suggesting broader applicability. However, bariatric surgery warrants tailoring to the individual patient’s characteristics and the present cohort represents the clinical daily life in bariatric surgery. Still, further studies, in particular those of a prospective randomized controlled nature, are of importance such as the announced SLIM trial, of which the results are expected to be published in the future [38].
In conclusion, implementation of a long-BPL RYGB with a BPL of 150 cm and an RL of 100–150 cm is safe. It provides accelerated weight loss and improved metabolic response as reflected by HbA1c reduction with low overall morbidity and manageable nutritional deficiencies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Phelps NH, Singleton RK, Zhou B, et al. Worldwide trends in underweight and obesity from 1990 to 2022: a pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults. The Lancet [Internet]. 2024;403(10431):1027–50. Available from: 10.1016/S 0140-6736(23)02750-210.1016/S 0140-6736(23)02750-2PMC 761576938432237 · doi ↗ · pubmed ↗
- 2Ong KL, Stafford LK, Mc Laughlin SA, et al. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2023;402(10397):203–34. 10.1016/S 0140-6736(23)01301-6.10.1016/S 0140-6736(23)01301-6PMC 1036458137356446 · doi ↗ · pubmed ↗
- 3Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric-metabolic surgery versus conventional medical treatment in obese patients with type 2 diabetes: 5 year follow-up of an open-label, single-centre, randomised controlled trial. Lancet. 2015;386(9997):964–73. 10.1016/S 0140-6736(15)00075-6.10.1016/S 0140-6736(15)00075-626369473 · doi ↗ · pubmed ↗
- 4Svanevik M, Lorentzen J, Borgeraas H, et al. Patient-reported outcomes, weight loss, and remission of type 2 diabetes 3 years after gastric bypass and sleeve gastrectomy (Oseberg); a single-centre, randomised controlled trial. Lancet Diabetes Endocrinol. 2023;11(8):555–66. 10.1016/S 2213-8587(23)00127-4.10.1016/S 2213-8587(23)00127-437414071 · doi ↗ · pubmed ↗
- 5Aminian A, Wilson R, Zajichek A, et al. Cardiovascular outcomes in patients with type 2 diabetes and obesity: comparison of gastric bypass, sleeve gastrectomy, and usual care. Diabetes Care. 2021;44(11):2552–63. 10.2337/dc 20-3023.10.2337/dc 20-302334503954 · doi ↗ · pubmed ↗
- 6Closs C, Ackerman M, Masson W, et al. Effectiveness of Roux-en-Y gastric bypass vs sleeve gastrectomy on lipid levels in type 2 diabetes: a meta-analysis. J Gastrointest Surg. 2022;26(8):1575–84. 10.1007/s 11605-022-05338-5.10.1007/s 11605-022-05338-535513608 · doi ↗ · pubmed ↗
- 7Ruiz-Tovar J, Vorwald P, Gonzalez-Ramirez G, et al. Impact of biliopancreatic limb length (70 cm vs 120 cm), with constant 150 cm alimentary limb, on long-term weight loss, remission of comorbidities and supplementation needs after Roux-en-Y gastric bypass: a prospective randomized clinical trial. Obes Surg. 2019;29(8):2367–72. 10.1007/s 11695-019-03717-7.10.1007/s 11695-019-03717-731104282 · doi ↗ · pubmed ↗
- 8Steenackers N, Vanuytsel T, Augustijns P, et al. Adaptations in gastrointestinal physiology after sleeve gastrectomy and Roux-en-Y gastric bypass. Lancet Gastroenterol Hepatol. 2021;6(3):225–37.10.1016/S 2468-1253(20)30302-233581761 · doi ↗ · pubmed ↗