Integrated imaging in rare eyelid lesions: a case report of palpebral dirofilariosis
Luca Tinunin, Filippo Ugolini, Dario Giattini, Nicola Santoro

TL;DR
A rare eyelid infection caused by Dirofilaria repens was diagnosed using combined clinical, imaging, and histological methods in a 64-year-old man.
Contribution
The paper highlights the diagnostic value of integrating clinical, radiologic, and histologic data in diagnosing rare zoonotic infections like Dirofilaria repens.
Findings
Integrated imaging and histology confirmed Dirofilaria repens infestation in a subcutaneous eyelid nodule.
Digitalized imaging access improves diagnostic accuracy and reduces delays in ophthalmic care.
Dirofilaria repens is an emerging zoonosis with increasing incidence in Mediterranean regions.
Abstract
Integrated evaluation of clinical records, radiologic imaging, and histologic slides was key in the diagnosis of a rare ophthalmic infection such as Dirofilaria repens, an emerging zoonosis in many Mediterranean regions, where it is endemic in cats and dogs and can spread to humans through mosquitos of the genera Anopheles, Aedex and Culex. We present the case of a 64-year-old male with a subcutaneous nodule at the right medial canthus. Surgical excision was performed under the clinical suspicion of a sebaceous cyst, and the specimen was submitted for pathological examination. Histological analysis revealed a partially necrotic abscess with numerous eosinophils and multiple cross-sections of the body of a parasite. The integrated evaluation of CT, MRI and histologic sections were consistent with the diagnosis of infestation by a female Dirofilaria repens. In this report we discussed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
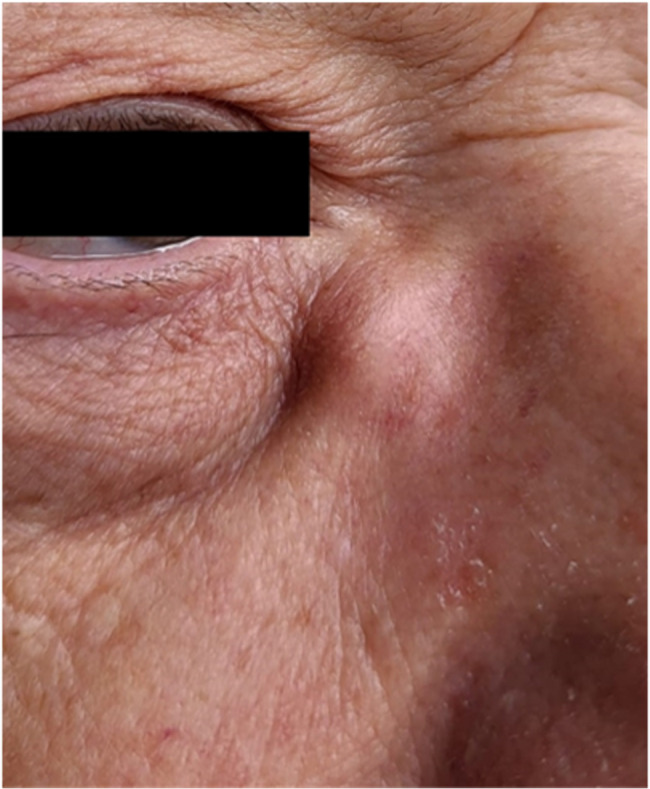 Figure 1
Figure 1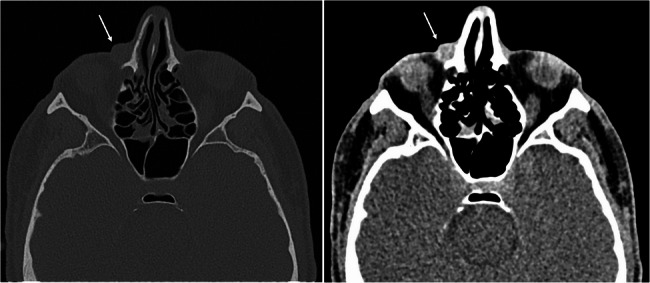 Figure 2
Figure 2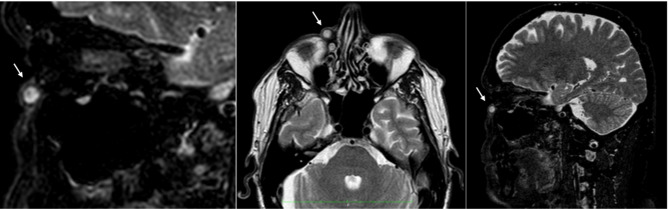 Figure 3
Figure 3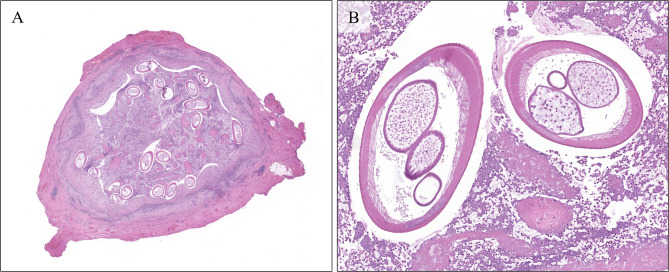 Figure 4
Figure 4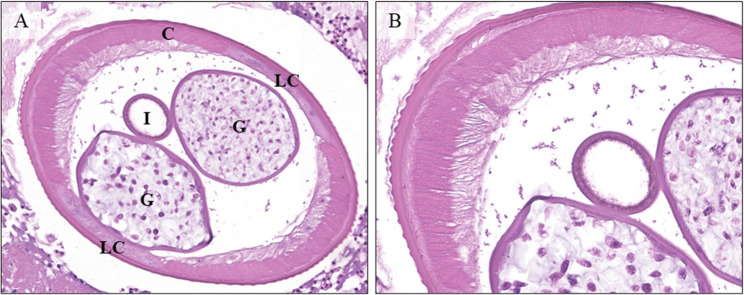 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasitic Diseases Research and Treatment · Mosquito-borne diseases and control · Retinal and Optic Conditions
Introduction
As imaging tools advance in resolution and accessibility, the opportunity for image integration becomes increasingly available and useful. This approach is particularly valuable in high complexity disciplines such as ophthalmology that employ multiple imaging modalities [10], allowing for all involved in the care of patients to always access relevant imaging and clinical records, thus reducing delays and preventing mistakes [4].
Furthermore, integrated systems enable more convenient consultations by facilitating real-time collaboration between specialists, regardless of their physical location, thus breaking down barriers to expert insights and improving diagnostic accuracy [15].
This report aims to illustrate an illustrative case of a rare disease in ophthalmic pathology, in which the collaboration between surgeon and pathologist was key to reaching the correct diagnosis.
Ophthalmic parasitosis caused by helminths in the genus Dirofilaria are exceedingly rare in humans, yet, growing evidence suggests that these infections are on the rise in southern and eastern Europe, as well as in southern Asia, and the USA [18, 19]. Worldwide there have been 1782 cases reported [16]. The mediterranean basin is the area with the highest incidence in Europe, with Italy (336 cases) and France (91 cases) at the forefront [16].
Dirofilaria repens infections often present as subcutaneous eyelid nodules [2, 5], but a few recent reports have started documenting microfilaremia in humans [20]. Histological examination and description of the parasite’s distinctive morphological features is usually sufficient for a diagnosis [13]. If blood tests are conducted, specific serum IgGs can be documented by ELISA, PCR can confirm the identification of the parasite as D.repens, and microfilaremia can be documented using a modified Knott’s test [20, 22].
Case report
A 64-year-old male veterinary surgeon was referred to our Oculoplastic Service (Careggi University Hospital, Florence, Italy) in September 2023, for the evaluation of a painless nodule at the medial canthus of the right eye (RE). The lesion appeared 4 months prior and was initially treated as dacryocystitis with oral antibiotics, with no benefit.
He did not report any recent travels to Africa or Asia, but he was on a trip to Rimini (Emilia Romagna, Italy) the month before the onset of the lesion, during which he experienced a tingling sensation at the upper eyelid of the RE, as well as itching and redness.
A complete ophthalmological and adnexal examination revealed a swelling lesion at the medial canthus of the RE, without signs of inflammation. The nodule was adherent to deep planes and the overlying skin was not erythematous or ulcerated (Fig. 1).
Fig. 1A subcutaneous non-mobile nodule at the right medial canthus. The clinical findings supported the initial diagnosis of dacryocystits
No other alterations of the eye or the lacrimal apparatus were documented. A facial computed tomography (CT) scan showed a slightly hyperintense preseptal nodule (Fig. 2).
Fig. 2. Facial computed tomography (CT) scan, showing a slightly hyperintense preseptal nodule (arrow) overlying the right medial canthal tendon, and slight air entrapment in the controlateral (left) lacrimal sac
Subsequently, Magnetic resonance imaging (MRI) was also obtained to further characterize the lesion (Fig. 3).
Fig. 3MRI (T2-weighted axial image) round lesion measuring 8 × 8 × 9 millimeters, located in the right inferomedial periorbital area (white arrow), adjacent to the frontal process of the maxillary bone. The lesion was characterized by well-defined and encapsulated margins (thickness of about 2 millimeters), hyperintense signal in T2 with marked enhancement after contrast administration, and a slight faded alteration of the perilesional soft tissue signal, consistent with perilesional edema
These clinical and imaging findings of an inflammatory-infectious lesion, located in the right periorbital area, overlying the medial canthal tendon, were deemed insufficient for a conclusive diagnosis and could not completely exclude from the differential diagnosis a neoplastic lesion. Therefore, we elected to perform an excisional biopsy.
The excised nodule, measuring 1.2 cm at its greatest dimension, was sent to the department of pathology for examination. The surgical fragment measured 1.1 × 0.8 × 0.5 cm; the nodule was then divided in half but showed no salient macroscopic features. Stained tissue sections were digitally scanned at ×400 magnification with a microscope slide scanner, Aperio AT2 platform (Leica Biosystems, Germany), into whole slide digital images (WSI).
Histopathological examination revealed an abscess with abundant necrotic debris, globular fibrin masses and numerous inflammatory cells, namely eosinophil and neutrophil granulocytes, with accompanying histiocytes, plasma cells and lymphocytes, surrounding multiple cross sections of the body of a parasite (Fig. 4).
Fig. 4A Low magnification view of the subcutaneous nodule, showing an abscess surrounded by fibrotic reaction with plasma cells and histiocytes, and containing multiple cross-sections of the parasite. H&E. B 10X magnification showing the contents of the abscess. Two cross-sections, one transversal and the other at an angle, of the body of the worm. The parasite is surrounded by necrotic debris, with fibrin deposits and numerous inflammatory cells, chiefly eosinophil, and neutrophil granulocytes. H&E
The morphological features, as illustrated in the previous sections, were highly specific, representing one of the most common microscopic findings of this condition *(*Pampiglione et al., [12] and the diagnosis of subcutaneous infection by Dirofilaria repens was made.
We counted 19 cross sections of the body of the worm, with a maximum transversal diameter of 456 μm (Fig. 5).
Fig. 5A Higher magnification (20X) showing the detail of the multilayered cuticle, the pseudocoelomatic cavity with the intestine and the genital tubules with numerous ovocytes. The main structures of the worm’s body are clearly visible in this image: The cuticle (C) with parallel ridges of muscle fibers, the lateral cords (LC), the intestine (I) and the two genital tubules (G). Several eosinophils surround but do not infiltrate the nematode’s tissues. H&E. B: 40X Detail of the cuticle, one of the most diagnostic features of a nematode, allowing the diagnosis of the genus Dirofilaria. Together with the description of the genital tubules and the size, these morphologic features allow for the diagnosis of Dirofilaria repens infection. H&E.
The morphological features were mostly intact, a sign that the worm was either alive or recently dead at the time of excision [13].
Following the diagnosis the patient underwent further laboratory testing, including PCR and specific IgG dosing on serum for Dirofilaria and for Trichinella, which were negative. Other blood parameters and IgE dosing were within the norm for the age of the patient.
The postoperative course was uneventful, with no complications or recurrences observed during follow-up.
Discussion
Dirofilaria infections are endemic in cats and dogs of the Mediterranean region [21], trasmission to humans occurs via arthropod vectors, primarly mosquitos in the genera Anopheles, *Aedex and Culex *[6]. However, humans are an accidental host, and the nematodes do not reach sexual maturity [24]. The most frequent presentation of Dirofilaria repens infection is that of a subcutaneous nodule of the ocular adnexa, which is often painful and inflamed[2, 5, 12], but other Dirofilaria species can affect different districts, such as the pulmonary vascular tree or the epididymis, or even cause systemic disease [2, 5, 11]. Indeed, emerging data, as previously stated, prove that microfilaremia can occur in humans. Interestingly, data gathered in dogs has shown a possible link between the severity of microfilaremia and overall clinical condition of the infected host [22].
Histological examination and description of the parasite by morphology is usually sufficient for a diagnosis, and clinical suspicion is not generally high enough to warrant specific laboratory workup before surgery, which would include PCR on fresh bioptic samples and serum specific antibody titer, although both could be unsuccessful in the case of older lesions, since these contain only parasitic remains *(*Pampiglione et al., [13]. When preserved the features include a distinctive layered cuticle with thick parallel ridges, in bands perpendicular to the body axis. The two bands of parallel ridges (representing the smooth cell musculature) are separated by lateral cords characterized by an amorphous material and few nuclei [11]. The pseudocoelomatic cavity contains a single small tube representing the esophagus and intestine and larger ones representing the reproductive system: a double one for females and a single one for males [5].
Infections with parasites from the genus Dirofilaria are rare, but some regions in the mediterranean basin, such as Italy and southern France, have a relatively higher number of cases [14], Although rare, there is evidence that infection’s incidence is increasing. Potential causes are the climate change which predisposes to the spread of the vector, closer contact with canine and feline pets, and higher awareness by physicians of this disease [12, 19].
Differential diagnosis is therefore crucial to exclude neoplastic or cystic lesions, as in our case, or infection by the more dangerous species of the genus.
Integrated and digitalized imaging in ophthalmic pathology is crucial in the diagnostic process of such challenging and rare cases. This approach could aid in the more accurate diagnosis of zoonoses, as they increasingly pose a challenge for care providers in the age of advancing climate change and increasing mobility of populations.
Furthermore, as radiologic clues are subtle and aspecific in these diseases, close collaboration and consultation of expert opinions is all the more relevant [9]
Clinicians and pathologists operating in this field increasingly approach the workflow in an integrated way in many key areas, such as cancer margin status evaluation [7] and initial assessment of peri-ocular lesions [1].
A more widespread use of digital imaging in ocular pathology not only would allow for these beneficial collaborations between radiologists, surgeons, and pathologists, but would ensure more expedite and accurate diagnoses in rare disease, such as the one presented here, facilitating consultation of experts [15].
Integrated approaches have been proven useful not on only in ophthalmology, but in many other contexts of care, such as the grading of prostate cancer, thus allowing more accurate and less impactful prognostication [8], They also allow for the implementation of powerful computational pathology tools, aiding, for example, in the evaluation of lymph node involvement in gastric cancer [23].
Additionally, in the specific case of this emerging zoonosis, when diagnostic suspicion is low, the chance to obtain adequate material for molecular evaluation is often lost when the parasite is not isolated live, as in our case, and submitted entirely for evaluation, since, as already stated, fresh bioptic samples are generally required for DNA extraction [13].
The aim of this report was to describe a typical case of a rare ophthalmic lesion, accompanied with radiological imaging, clinical data and digitalized slides, with a summary of the diagnostic features necessary to identify this parasite, and to distinguish it from its potentially more dangerous close relatives, in the context of the rising incidence and spread of the vector for this zoonosis, which is increasingly considered an emerging condition [3, 17].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Blaizot R, Receveur MC, Millet P, Otranto D, Malvy DJM (2018) Systemic Infection With Dirofilaria repens in Southwestern France. In Annals of Internal Medicine (Vol. 168, Issue 3, pp. 228–229). American College of Physicians. 10.7326/L 17-042610.7326/L 17-042629086799 · doi ↗ · pubmed ↗
- 2Capelli G, Genchi C, Baneth G, Bourdeau P, Brianti E, Cardoso L, Danesi P, Fuehrer HP, Giannelli A, Ionicǎ AM, Maia C, Modrý D, Montarsi F, Krücken J, Papadopoulos E, Petrić D, Pfeffer M, Savić S, Otranto D, Silaghi C (2018) Recent advances on dirofilaria repens in dogs and humans in europe. In Parasites and vectors. Bio Med Cent Ltd 11(1). 10.1186/s 13071-018-3205-x 10.1186/s 13071-018-3205-x PMC 629998330567586 · doi ↗ · pubmed ↗
- 3Jelinek T, Schulte-Hillen J, Loscher AT (1996) HUMAN DIROFILARIASIS. In International journal of Dermatology (Vol. 35, Issue 12 , page 872-875)10.1111/j.1365-4362.1996.tb 05054.x 8970844 · doi ↗ · pubmed ↗
- 4Kraft DC, Naeem M, Mansour J, Beal MA, Bailey TC, Bhalla S (2023) Body Imaging of Bacterial and Parasitic Zoonoses: Keys to Diagnosis. In Radiographics (Vol. 43, Issue 3). Radiological Society of North America Inc. 10.1148/rg.22009210.1148/rg.22009236729948 · doi ↗ · pubmed ↗
- 5Rouhette H, Marty P, Zur C, Bain O, Fenollar S, Gastaud P (1999) Case Report W Description de cas W Fallbericht Ocular Filariasis: Not Strictly Tropical. In Ophthalmologica (Vol. 213)10.1159/00002742110202297 · doi ↗ · pubmed ↗
- 6Simón F, Siles-Lucas M, Morchón R, González-Miguel J, Mellado I, Carretón E, and Jose Alberto Montoya-Alonso (2012). Human Animal Dirofilariasis: the Emergence of a Zoonotic Mosaic. Clinical Microbiology Reviews, 25(3), 507–544. 10.1128/CMR.00012-1210.1128/CMR.00012-12PMC 341648822763636 · doi ↗ · pubmed ↗
- 7Strianese D, Martini A, Molfino G, Falabella, Tranfa F (1998) Orbital dirofilariasis. European journal of ophthalmology. 8 (4), 258–262. 10.1046/j.1442-9071.2002.00562.x 10.1177/1120672198008004109891899 · doi ↗ · pubmed ↗
- 8Tasić-Otasevic S, Golubović M, Trichei S, Zdravkovic D, Jordan R, Gabrielli S (2023) Emerging Infectious Diseases. 29(12), 2548–2550. 10.3201/eid 2912.23079610.3201/eid 2912.230796 PMC 1068381737987593 · doi ↗ · pubmed ↗