First steps in the development of an ovine proximal phalanx fracture and bone defect model: a study of animal welfare and bone healing
Nanett Kvist Nikolaisen, Thomas Colding-Rasmussen, Peter F. Horstmann, Anna V. Müller, José Joaquín Cerón, Michael Mørk Petersen, Christian Nai En Tierp-Wong, Stine Jacobsen

TL;DR
A new sheep model for studying small bone fractures allows natural movement and better animal welfare while investigating bone healing.
Contribution
A novel ovine proximal phalanx fracture model that enables natural movement and social housing while assessing bone healing and animal welfare.
Findings
The osteotomy group showed better stability and healing compared to the ostectomy group.
Pain scores were generally low and peaked only after surgery and analgesia withdrawal.
Implant failure was frequent in 6 mm ostectomies with limited healing.
Abstract
There is a need for large-animal fracture models focusing on small tubular bones, as existing models typically involve major weight-bearing bones and often rely on restrictive suspension systems that raise significant animal welfare concerns. This study presents a novel in vivo sheep model targeting the proximal phalanx, designed to enable natural movement and social housing whilst supporting the investigation of fracture fixation and bone healing. Eleven skeletally mature Texel sheep were included; four underwent bilateral ostectomies with 3 mm or 6 mm defects, and seven received an osteotomy. A hoof block was used to offload the affected digit, enabling the sheep to move freely and to be housed in pairs. Bone healing was assessed using standardised radiographic scoring based on images obtained intraoperatively, at week 1 and 2, and hereafter every second week. Hard callus thickness…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
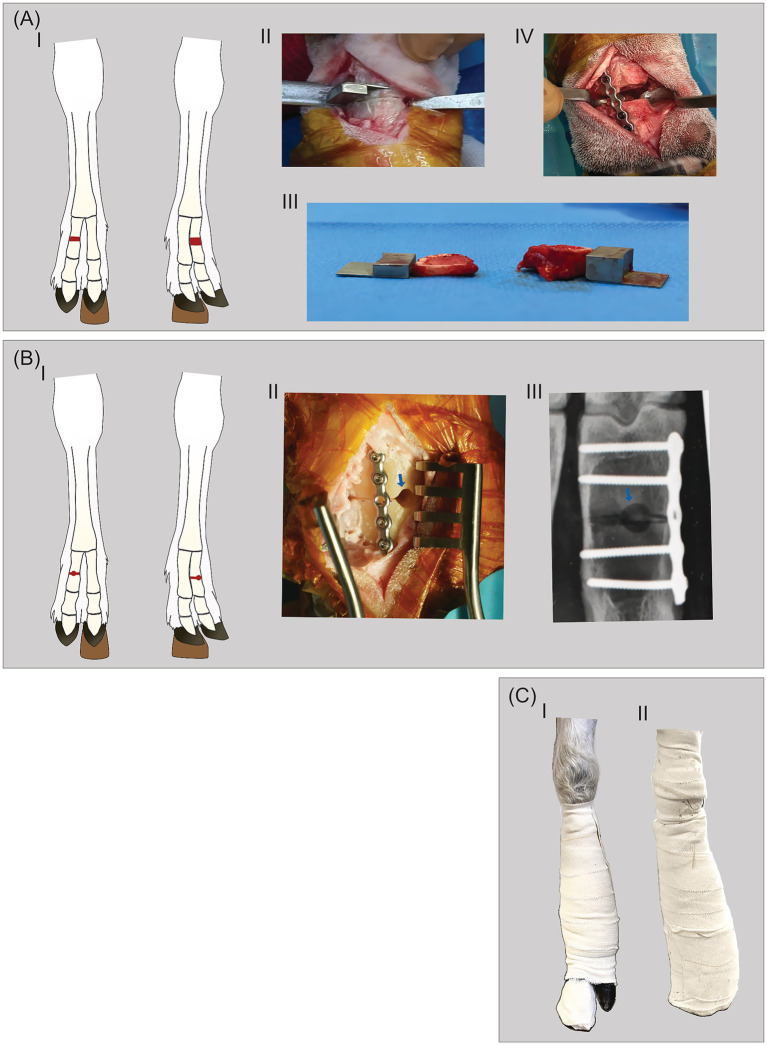 Figure 1
Figure 1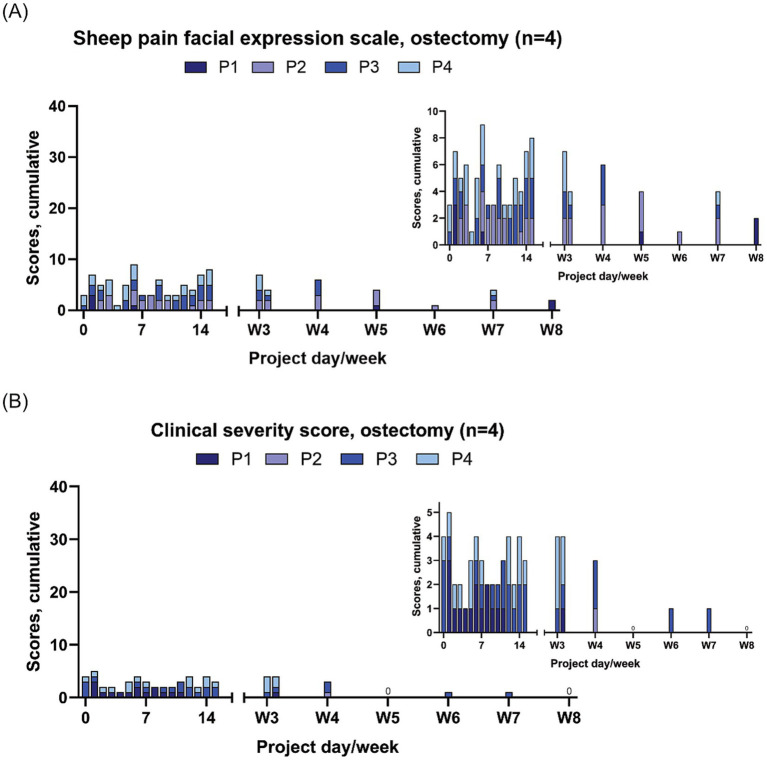 Figure 2
Figure 2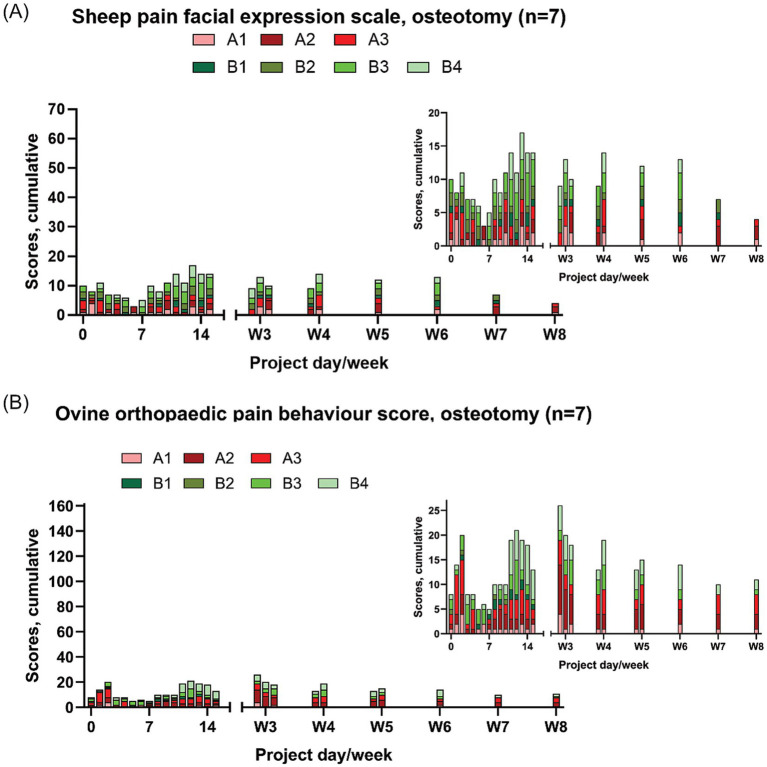 Figure 3
Figure 3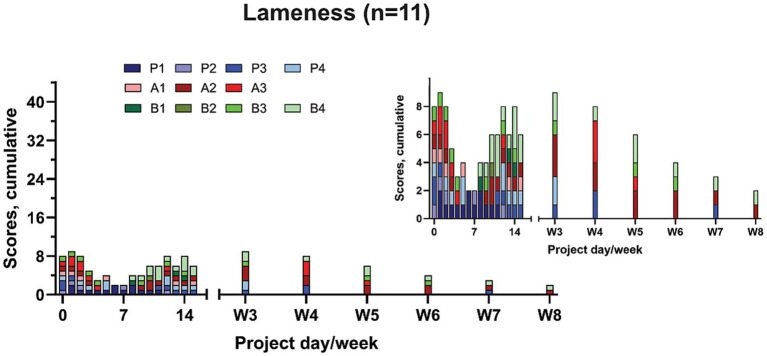 Figure 4
Figure 4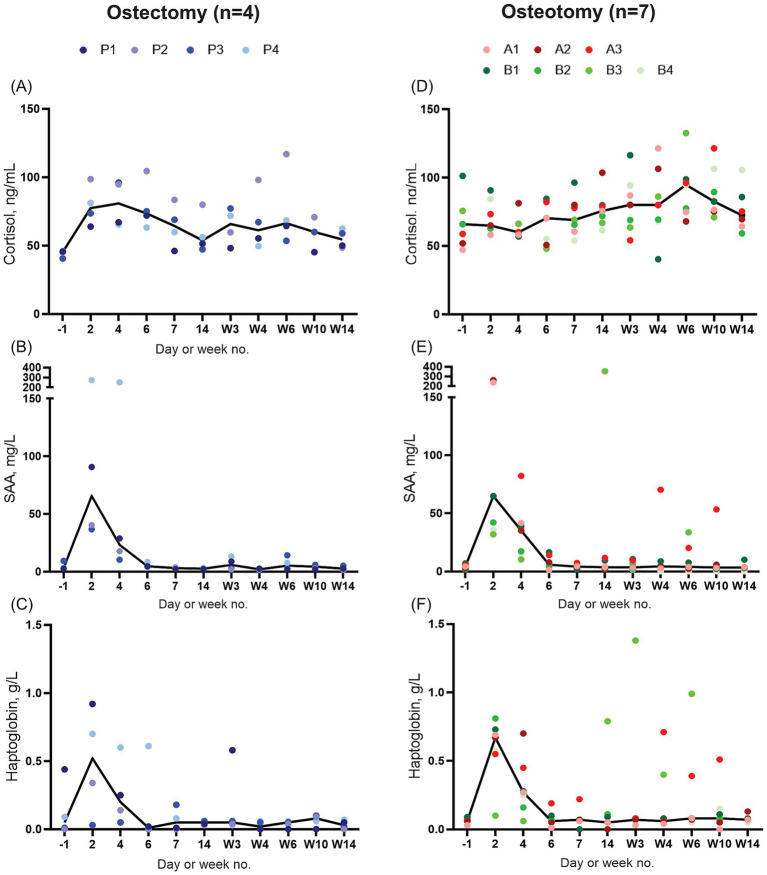 Figure 5
Figure 5| Sheep ID (limb) and group | Osteosynthesis | Aftercare | Implant stability (week no.)* | Alignment (degrees) | Time of first signs of callus formation in the gap | Healing status at week 16 | Callus thickness (mm) | |
|---|---|---|---|---|---|---|---|---|
| Block | Cast/bandage | |||||||
| P1 (LF) | 6-hole locking plate, unicortical screws | Week 0–10 | Bandage week 0–8 | Screw loosening (1, 3, 10); plate dislodgement (10) | 6.8 | No callus | No bone formation in gap; rounding of fracture edges | NA |
| P2 (RF) | 6-hole locking plate, unicortical screws | Week 0–10 | Bandage week 0–8 | Screw loosening (10, 14); plate dislodgement (14) | 6.3 | Week 12 | Moderate bone formation in gap | 1.55 |
| P3 (RF) | 6-hole locking plate, unicortical screws | Week 0–10 | Bandage week 0–8 | Screw loosening (1); screw breakage (4, 6); plate dislodgement (6) | 7.6 | Week 8 | Moderate bone formation in gap | 1.3 |
| P4 (LF) | 6-hole locking plate, unicortical screws | Week 0–10 | Bandage week 0–8 | Screw breakage (8, 12) | 0.2 | Week 10 | Moderate bone formation in gap | 2.55 |
| P1 (RF) | 6-hole locking plate, unicortical screws | Week 0–10 | Bandage week 0–8 | Screw breakage (8, 16); plate dislodgement (16) | 11.5 | No callus | No bone formation in gap; rounding of fracture edges | NA |
| P2 (LF) | 6-hole locking plate, unicortical screws | Week 0–10 | Bandage week 0–8 | Plate dislodgement (10) | 4.5 | No callus | No bone formation in gap; rounding of fracture edges | 1.9 |
| P3 (LF) | 6-hole locking plate, unicortical screws | Week 0–10 | Bandage week 0–8 | Screw loosening (8); screw breakage (14) | 3.1 | No callus | No bone formation in gap; rounding of fracture edges | 0.85 |
| P4 (RF) | 6-hole locking plate, unicortical screws | Week 0–10 | Bandage weeks 0–8 | Screw loosening (4); screw breakage (8, 16) | 0.3 | No callus | No bone formation in gap; rounding of fracture edges | 2.175 |
| A1 (LF) | 5-hole locking plate, unicortical screws | Week 6–10 | Cast week 0–6, bandage week 6–8 | Screw loosening (4) | 6 | Week 8 | Clearly visible fracture line | 2.95 |
| A2 (RF) | 5-hole locking plate, unicortical screws | Week 3–10 | Cast week 0–3, bandage week 3–8 | Intact | 0.3 | Week 8 | Barely visible fracture line | 2.08 |
| A3 (RF) | 5-hole locking plate, unicortical screws | Week 4–16 | Cast week 0–4, bandage week 4–8 | Screw loosening (1) | 4.7 | Week 12 | Clearly visible fracture line | 1.28 |
| B1 (LF) | 5-hole locking plate, bicortical screws | Week 0–10 | Bandage week 0–8 | Intact | 2 | Week 6 | Barely visible fracture line | 0.785 |
| B2 (RF) | 5-hole locking plate, bicortical screws | Week 0–10 | Bandage week 0–8 | Screw breakage (6, 12, 14) | 4.6 | Week 6 | Clearly visible fracture line | 2.35 |
| B3 (RF) | 5-hole locking plate, bicortical screws | Week 0–10 | Bandage week 0–8 | Screw breakage (6) | 1.6 | Week 6 | Clearly visible fracture line, week 10** | NA |
| B4 (LF) | 5-hole locking plate, bicortical screws | Week 0–10 | Bandage week 0–8 | Intact | 0.5 | Week 6 | Barely visible fracture line | 0.525 |
| Total score, SPFES | Total score, OOPBS | Action |
|---|---|---|
| ≤3 | <7 | No action |
| 4–5 | 7–12 or lameness 3, 4 or on knees 3 | Treatment criterion 1: Analgesic medication changed/increased, increased monitoring |
| ≥6 | >12 | Treatment criterion 2: Analgesic medication changed/increased – if no effect, euthanasia |
| Parameter | Description | Score |
|---|---|---|
| Feed* | Normal, interested, been eating | 0 |
| Reduced interest | 1 | |
| Inappetence (no interest, not eating) | 2 | |
| General demeanour | Bright, alert, responsive | 0 |
| Quiet, alert, responsive | 1 | |
| Moderately depressed and inactive | 3 | |
| Depressed, inactive and nonresponsive | 4 | |
| Vocalisation | None | 0 |
| None, teeth grinding | 1 | |
| Occasionally vocalising or teeth grinding | 2 | |
| Frequently vocalising or teeth grinding | 4 | |
| Activity | Normal, resting and sleeping | 0 |
| Frequent change of position | 1 | |
| Restless | 2 | |
| Lameness | Normal standing and walking | 0 |
| Normal standing, minimal lameness in the walk | 1 | |
| Normal standing, lameness in the walk | 2 | |
| Relief of the affected leg, high lameness in the walk | 3 | |
| No usage of the affected leg, predominantly in suspension | 4 | |
| On knees | Not on knees | 0 |
| Occasionally on knees, e.g., when eating | 1 | |
| Frequently on knees when eating and walking | 2 | |
| Constantly on knees | 3 | |
| Other | None | 0, 0 |
| Flehmen | 2 | |
| Wool picking | 2 | |
|
|
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVeterinary Orthopedics and Neurology · Veterinary Pharmacology and Anesthesia · Surgical Sutures and Adhesives
Introduction
1
Fractures of non-weight bearing, small tubular bones, such as the phalanges and metacarpals, are common traumatic injuries (1, 2). These injuries often affect younger, working-age individuals and are associated with significant functional impairment and high healthcare costs (3, 4). The treatment can be challenging and associated with a high risk of complications, including stiffness, malunion, and non-union, and reoperations to remove implants are frequent (5, 6). In addition to trauma, other pathologies affecting these bones, such as infections, tumours and segmental bone defects of various causes, also present significant clinical challenges (7–9). Accordingly, there is a need to optimise the treatment of fractures, pathologies and defects in low load bearing small tubular bones.
To study and improve the treatment of bone fractures and bone pathologies in general, large animal models play an essential role. They enable preclinical evaluations of novel materials and techniques as well as advancements in treatment strategies (10, 11). Sheep are widely used due to their similarities to human bone in size, structure, biomechanics, and remodelling behaviour (10). Several fracture and defect models have been established and applied in sheep involving larger load bearing tubular bones such as the femur and tibia (12, 13). The translational relevance of these models to small tubular bones such as the phalanges and metacarpals is limited. This is due to fundamental differences in bone size, biomechanical loading conditions, and healing mechanics, as well as differences in soft tissue coverage and vascularity, with phalanges having minimal muscle coverage. Moreover, fractures in phalanges and metacarpal bones demand rapid rehabilitation to preserve fine motor function and prevent stiffness, which requires a fundamentally different treatment approach compared to long bone injury (14, 15).
Existing ovine fracture models require the protection of the fractured long bone. This is achieved through casts (12, 16–18) and/or by the use of restrictive devices such as slings, where the sheep are suspended for several (up to 9) weeks postoperatively (12, 16, 17, 19–25). This severely limits natural movement and behaviour and raises animal welfare concerns. There is a constant drive towards improving experimental animal welfare (26–28), and the development of fracture models that exert less strain on the experimental animals is highly needed. Measures aimed at minimising model severity and invasiveness, as well as methods improving postoperative welfare monitoring and care, we find are key in making fracture model research more ethically acceptable and valid.
A major societal concern pertains to the use of experimental animals in medical research, including research on fracture healing and repair. In the ARRIVE (Animal Research: Reporting of In Vivo Experiments) guidelines 2.0, which is an overview of information to include in publications describing animal research, the recommended set of items to be reported in the scientific paper includes housing and husbandry, care, monitoring, and analgesia (27). Some studies involving sheep in orthopaedic research have assessed pain-related welfare; Häger et al. (21) presented quantitative results from an assessment of pain-related facial expressions and clinical severity scores. Other studies have utilised gait evaluation and/or assessing pain-related behaviour, albeit without reporting quantitative results (16, 25, 29, 30).
To our knowledge, no large animal low load bearing small tubular bone model exists. Accordingly, the aim of this study was to develop an ovine phalanx fracture model. The welfare of the experimental animals was addressed by adopting an armamentarium of methods for monitoring pain and abnormal behaviours and applying them rigorously throughout the study period. Here we report the first steps towards development of a bilateral proximal phalanx fracture model in sheep.
Methods
2
Study overview
2.1
This study represents our initial approach to development of a novel ovine bilateral proximal phalanx fracture model. Twelve sheep were included; and the lateral proximal phalanges of both front limbs underwent fracture surgery. In 8 sheep a novel fracture repair modality was tested in one of the two phalanges, these results are reported elsewhere (31), whilst the remaining 16 phalanges were repaired using metallic implants as described below. The bilateral approach enables within-subject comparisons, reducing animal use in line with the 3Rs of animal experimentation (Replacement, Reduction, and Refinement) (32). With one sheep euthanized on day six due to systemic illness, the final sample was 15 phalanges. The fracture models investigated were transverse proximal phalanx midline ostectomy with 3 mm (n = 4 phalanges) or 6 mm (n = 4 phalanges) gaps, and midline osteotomy with central 4.5 mm drill hole (n = 7 phalanges) (Figures 1A,B). Fractures were fixated with one dorsolaterally placed stainless-steel locking plate. The sheep had either a walking cast or a custom-made offloading hoof block combined with bandages as coaptation (Figure 1C). By the end of the study period (16 weeks), the sheep were lightly sedated with xylazine (0.08 mg/kg BW, IV, Xysol Vet., ScanVet Animal Health A/S, Denmark) and butorphanol tartrate (0.04 mg/kg BW, IV, Dolorex, MSD Animal Health A/S, Denmark) and euthanised by pentobarbital (140 mg/kg BW, IV, Euthasol vet., Dechra Veterinary Products A/S, Denmark). Bone healing was evaluated by repeated radiographs throughout the 16-week study period and by post-euthanasia computed tomography (CT) scans. Animal welfare was analysed by repeated clinical examinations, lameness, pain face analysis, and by implementing a modified pain behaviour score as detailed below.
Overview of the ovine thoracic limb bilateral single toe (OBST) fracture model. (A) The ostectomy group showing (I) a schematic drawing of the bilateral intervention, (II) the application of the cutting guide, (III) the ostectomized bone segment of 3 mm and 6 mm and (IV) the ostectomized proximal phalanx osteosynthesized with 6-hole locking plate. (B) The osteotomy group showing (I) a schematic drawing of the bilateral intervention, (II) the osteotomized proximal phalanx osteosynthesized with 5-hole locking plate, the 4.5 mm drill-hole evident (blue arrow), and (III) radiograph depicturing the osteotomy line, drill-hole (blue arrow), metal-plate and bicortical screws. (C) Coaptation modalities of a left thoracic limb; (I) hoof block and elastic bandage, and (II) a half limb walking cast with no hoof block.
Animals
2.2
Eleven skeletally mature Texel ewes (5.5 years ± 3 months, 73 kg ± 7.6 kg) were included. The animals were kept in pairs indoors in 6 m^2^ pens with wood shavings as bedding. Their diet was adjusted according to nutritional requirements, and straw and water were provided ad libitum. During a 3–10 weeks acclimatization period prior to surgery, clinical health assessments were conducted following the European Animal Welfare Indicators (AWIN) protocol for sheep (33). Additionally, the sheep were trained by positive reinforcement to undergo clinical procedures, including sample collection, clinical examinations, and lameness assessment when led by a leash, so that these procedures could be conducted with minimal stress. In this acclimatization period, routine blood and faecal analyses were performed to ensure enrolment of only healthy animals, and the sheep were treated with Albendazole (4 mg/kg BW, Valbazen Vet., Zoetis Animal Health ApS, Denmark). To facilitate repeated monitoring of core temperature, a temperature-sensitive chip was inserted intramuscularly in Musculus omotransversarius, by identifying the fascial border between Musculus cleidooccipitalis and the cervical part of Musculi trapezii at the dorsal third of the neck (Global-Ident Bio-Thermo, Allflex, France).
Pre-surgical preparation and anaesthetic protocol
2.3
The sheep were initially fasted for 36 h preoperatively (n = 8) (34) but based on the frequent occurrence of moderate–severe diarrhoea in the immediate postoperative period, fasting duration was reduced to 24 h (n = 4) with no adverse effects during surgery and improved gastrointestinal health post-surgically (35). Water was withheld for 4 h before the scheduled surgery time. Premedication for anaesthesia included intravenous (IV) administration of xylazine hydrochloride (0.05 mg/kg, Xysol Vet., ScanVet Animal Health A/S, Denmark) and butorphanol tartrate (0.05 mg/kg, IV, Dolorex, MSD Animal Health A/S, Denmark). General anaesthesia was induced using diazepam (0.5 mg/kg, IV, Diazedor Vet., Salfarm Danmark A/S, Denmark) and ketamine hydrochloride (2.5 mg/kg, IV, Ketador Vet., Salfarm Danmark A/S, Denmark). Inhalation anaesthesia was maintained with isoflurane (1.5%, Vetflurane, Virbac Danmark A/S, Denmark). Tetanus antitoxin (1,500 units/animal SC, Tetanus antitoxin Equine Origin, Colorado Serum Company, Colorado) and antibiotics were administered prior to surgery. Antibiotic therapy included gentamicin sulphate (6.6 mg/kg BW, IV, Gentavet, ScanVet Animal Health A/S, Denmark) and benzylpenicillin sodium (22,500 IU/kg BW, IV, Benzylpenicillin, Panpharma Nordic AS, Norway), with the latter re-dosed every 80 min during surgery. Intraoperative analgesia consisted of flunixin meglumine (2.2 mg/kg BW, IV, Wellicox, Ceva Animal Health A/S, Denmark), and a SC ring block on each forelimb using bupivacaine hydrochloride (0.1 mg/kg BW, SC, Bupivacaine Baxter, Baxter A/S, Denmark) and mepivacaine hydrochloride (0.4 mg/kg BW, SC, Mepidor Vet, Salfarm Danmark A/S, Denmark).
Surgical protocol
2.4
The sheep were placed in dorsal recumbency with flexed, stabilised forelimbs. A tourniquet was applied mid-metacarpally. A dorsolateral curved incision was made, and the bone was exposed by blunt dissection and periosteal elevation. The extensor and flexor tendons were retracted and protected. In the ostectomy group removal of the bone section was conducted by first approximating the middle of the phalanges from an intraoperative radiograph. Then a conical 0.6 mm sawblade (DePuy Synthes) was applied to cut the bone halfway through, after which a custom made 3- or 6-mm cutting guide was inserted to guide the saw blade and make a standardised ostectomy size (Figure 1A; Supplementary Figures 1a,b). Each sheep in the ostectomy group received both a 3 mm and a 6 mm ostectomy, randomly assigned to either the left or right front limb proximal phalanx (Table 1).
In the osteotomy group (n = 7) a dorsal midshaft 4.5 mm unicortical defect was created using a 4.5 mm drill bit, followed by a midline osteotomy performed with a conical 0.6 mm sawblade (46/25 × 6 × 0.6/0.4 mm (519.230S), DePuy Synthes, Johnson & Johnson MedTech, Massachusetts, USA). After ostectomy or osteotomy, metal implant fixation was performed (Table 1).
The 3- and 6-mm ostectomies were fixated with a 6-hole cuttable stainless-steel locking plate (1.5 mm, Straight (02.114.005S), DePuy Synthes, Johnson & Johnson MedTech, Massachusetts, USA) using four unicortical locking screws (cortex stardrive, Ø 1.5 mm, L 10 mm (02.214.110S), DePuy Synthes, Johnson & Johnson MedTech, Massachusetts, USA), two in each fragment (Figure 1A). The osteotomies were fixated with a five-hole cuttable stainless-steel locking plate (shorter version of plate used for ostectomies) with either four unicortical screws (n = 3 phalanges, subgroup A, same screw types as described for ostectomies) or four bicortical screws (n = 4 phalanges, subgroup B, Ø 1.5 mm, L 16 mm (VS106.018), DePuy Synthes, Johnson & Johnson MedTech, Massachusetts, USA) (Figure 1B; Supplementary Figure 1c,d).
After the osteosyntheses were completed, the soft tissues were closed by simple continuous pattern (fascia) (Novosyn 2/0, B Braun Medical Inc., USA) and simple interrupted pattern (skin) (Optilene 2/0, B Braun Medical Inc., USA).
Post-surgical coaptation
2.5
To find the most useful coaptation, two different approaches were adopted. In the osteotomy sheep (n = 4) a hoof block adjusted to fit an ovine digit was applied. This had a height of 20 mm (Hoof block, standard, Klovshoppen, Denmark), and it was glued (Mini Moo Gloo, MooGloo, Durham, USA) under the medial digit on both front limbs for offloading of the osteosynthesized digit. Additionally, a supportive and protective elastic bandage was applied over the surgical site (Figure 1C). In osteotomy subgroup A (n = 3 sheep), a half-limb walking cast was applied for approximately 4 weeks post-surgery (Figure 1C), hereafter elastic bandages and hoof blocks were applied until week 8 (Figure 1C). In subgroup B (n = 4 sheep), we opted to use hoof block offloading and bandages as described for the ostectomy group. All sheep were permitted to ambulate unrestrictedly post-surgery. In all sheep, the elastic bandages were removed at week 8 and the hoof blocks were removed at week 10 after surgery. In the osteotomy group, one sheep was euthanized on day 70 due to hoof trauma.
Radiography and computed tomography
2.6
Radiographs were obtained throughout the 16-week study period, i.e., intra-operatively and at 1, 2, 4, 6, 8, 10, 12, 14, and 16 weeks. For the post-surgery radiography, the sheep were lightly sedated with xylazine (0.08 mg/kg BW, IV, Xysol Vet., ScanVet Animal Health A/S, Denmark) and butorphanol tartrate (0.04 mg/kg BW, IV, Dolorex, MSD Animal Health A/S, Denmark). At week 16, radiography and CT were acquired immediately after euthanasia. Each radiographic study entailed three projections: dorsopalmar, dorsomedial-palmerolateral oblique, and lateromedial. A portable Gierth TR80/20 system was used, set to 60 kV and 3 mAs, along with Fujifilm FDR D-EVO console software. For CT, a Siemens Somatom Emotion (46,213, 14o kV) was used.
From the radiographs, the following parameters were recorded to investigate fracture fixation stability and bone healing:
Implant component stability was classified based on occurrences of screw loosening and/or plate dislodgment.Fragment alignment was defined as the difference in angle degrees between the proximal and distal fragment in anterior–posterior projection at the intraoperative radiographs vs. radiographs at week 12. Week 12 was chosen to allow for an evaluation of the effect of removing the offloading hoof-block in relation to fragment alignment, which was performed at week 10.First signs of callus formation in the fracture gap were recorded and the corresponding week was noted (Table 1).Healing status at week 16 was categorised by using parameters from two individual healing scoring systems: radiographic union scale in tibial fractures (RUST) and Lane and Sandhu scoring system (36, 37). The RUST system scores each cortex (anterior, posterior, medial, and lateral) based on two criteria: presence of callus and visibility of the fracture line. A cortex receives 1 point if no callus is present and the fracture line is visible, 2 points if callus is present but the fracture line remains visible, and 3 points if callus is present and the fracture line is no longer visible. The Lane and Sandhu system evaluates bone healing based on three parameters: bone formation at the fracture gap (none, moderate, or complete), visibility of the fracture line (clearly visible, blurred, or not visible), and degree of remodelling (none, beginning signs, or complete remodelling). ‘Presence of bone formation in the fracture gap’ (Yes/No), was applied in the ostectomy group only, whilst ‘fracture line visibility (clearly visible, blurred or not visible)’ was applied in the osteotomy group. Clearly visible fracture lines were defined as uninterrupted and sharply delineated lines, corresponding to the lowest score in the Lane and Sandhu system. Additionally, the presence of rounding at the fracture edges was recorded, as an indication of potential non-healing (Table 1).
Callus thickness was measured from CT images, assessing the radiographically dense (mineralised) hard callus visible on the scans (Supplementary Figure 2). Callus thickness was measured in two designated areas on each fragment, yielding four measurements per sheep. The mean value was reported. The first measurement was taken at the subjectively identified thickest region of callus on transverse CT images. From this point, a line was drawn towards the centre of the bone, and a second line was drawn from the centre at a 45° angle relative to the first line, towards the cortex, directed away from the plate. Callus thickness was then measured along this second line (Supplementary Figure 2).
Post-surgery care and welfare monitoring
2.7
Following surgery, all sheep received antimicrobial and analgesic treatment. Gentamicin sulphate was administered once daily (6.6 mg/kg, IV, Gentavet, ScanVet Animal Health A/S, Denmark), and benzylpenicillin sodium was given intravenously every 6 h (22,500 IU/kg, IV, Benzylpenicillin, Panpharma Nordic AS, Denmark) – the ostectomy groups received antimicrobial treatment for a duration of 7 days, this was downregulated for the osteotomy group for a duration of 3 days.
For pain management, flunixin meglumine (2.2 mg/kg, IV; Wellicox, Ceva Animal Health A/S, Denmark) was administered twice daily for the first 3 days, followed by once-daily dosing until day eight.
The sheep were closely monitored throughout the study period. Throughout the study period they were observed by technical staff twice daily, where appetite, general well-being and intactness of the coaptation was assessed. During the first 2 weeks after surgery, clinical assessments were conducted by veterinarians two to five times daily, with frequency decreasing over time. In weeks 3–5 veterinary assessment occurred twice a week, and for the rest of the study period once a week. The clinical assessment included temperature (by scanning the temperature-sensitive chip), heart rate, respiratory rate, rumen contractions, lameness and two pain scores. The weight of the animals and their body condition score were evaluated several times during the study period.
The hoof block was continuously monitored and adjusted as needed to optimise the sheep’s ambulation, including increasing the weight-bearing surface by adding composite material on the edges of the hoof block (Supplementary Figure 3). A detached hoof block was immediately replaced. Adjustments or replacements were performed under light sedation, as described above.
The sheep pain facial expression scale (SPFES)
2.8
Pain facial expressions were assessed using the SPFES developed by McLennan et al. (2016) (38). Five facial regions were scored based on the presence of pain-related expressions: (1) tightening of muscles surrounding eyes, closing of the eye, (2) tightening of the muscles of the cheek and in area of the zygomatic arch, (3) ear position, (4) lip and jaw profile, and (5) shape of nostrils and philtrum. The sheep were observed for 2 min from a distance to avoid interference with their potential pain-related facial expression. The SPFES has a maximum total score of ten. Three levels of treatment criteria were defined based on the SPFES (Table 2).
The ovine orthopaedic pain behaviour score (OOPBS)
2.9
Initially, the clinical severity score (CSS) described by Häger et al. (21) was utilised for the ostectomy group. The CSS includes assessments of food/water consumption, lameness, activity and presence of vocalisation. Based on the CSS and experience from the ostectomy group, the novel a priori weighted composite OOPBS was developed to create a more refined and sensitive pain scoring system, tailored to the behavioural signs relevant in orthopaedic research. By incorporating specific indicators such as posture and general demeanour, the new a priori weighted composite OOPBS aimed to provide a more sensitive and accurate assessment of pain. The OOPBS included assessment of appetite, general demeanour, vocalisation/teeth grinding, general activity, lameness, kneeling, and other adverse behaviours (such as flehmen and wool picking) (Table 3). The sheep were observed for 2 min from a distance. The maximum attainable score was 23, with varying weights assigned to different parameters, reflecting their proposed significance, similar to what has been done in horses (39). Three levels of treatment criteria were defined (Table 2).
If a sheep reached a treatment criterion in either the OOPBS and/or the SPFES, increased monitoring was initiated, and actions such as adaptation of the coaptation and/or additional analgesic treatment were taken. Available options for supplementary analgesia included flunixin meglumine (2.2 mg/kg, IV, Wellicox, Ceva Animal Health A/S, Denmark), butorphanol tartrate (0.2 mg/kg, IM, Dolorex, MSD Animal Health A/S, Denmark), meloxicam (1 mg/kg, SC, Metacam, Boehringer Ingelheim Vetmedica GmbH, Germany), transdermal fentanyl patches (100 μg/h transdermal, Fentanyl Sandoz, Sandoz A/S, Denmark), buprenorphine hydrochloride (0.01 mg/kg, IM, Bupaq Multidose Vet., Salfarm Danmark A/S, Denmark), or regional nerve blocks mid-metacarpal using bupivacaine hydrochloride (0.3 mg/kg BW, SC, Bupivacaine Baxter, Baxter A/S, Denmark) and mepivacaine hydrochloride (1.0 mg/kg BW, SC, Mepidor Vet, Salfarm Danmark A/S, Denmark) (40).
Biomarkers
2.10
Blood and saliva samples were collected preoperatively (day −1) and on days 2, 4, 6, 7, and 14, and hereafter week 3, 4, 6, 10, and 14. All samples were collected at the same time a day, to avoid diurnal influences.
Prior to saliva collection, the sheep’s mouth was rinsed with 30 mL of tap water using a syringe. Saliva samples were collected using Salivette® tubes (Sarstedt Aps, Bording, Denmark), which consists of an absorbent component and a centrifuge tube designed for non-invasive saliva collection. The original absorbent component in the Salivette® was replaced with sponges (Esponja Marina, La Griega E. Koronis, Madrid, Spain). A sponge was held with forceps inside the sheep’s mouth for 30–60 s. The saliva-saturated sponge was transferred to a Salivette® tube. This procedure was repeated with one or two additional sponges until an adequate volume of saliva was collected. The Salivette® tube was centrifuged within 30 min after collection at 3000 × g for 10 min at 4 °C and saliva transferred to a cryotube (Maxxline Cryo Tubes, non-sterile, Dacos, Hvidovre, Denmark). Collecting saliva was a non-invasive and cheap procedure to which the sheep quickly adapted.
Blood was collected by an indwelling intravenous catheter (Long-Term MILACATH® – Large Animal Kits – Seldinger Technique, Mila International, Inc., Kentucky, USA) or by venipuncture of v. jugularis. The blood samples were collected in BD Vacutainer® 4 mL tubes coated with lithium heparin (Becton Dickinson Vacutainer Systems Europe) for plasma. The samples were centrifuged within 30 min of collection at 1,800 × g for 10 min at 4 °C and plasma transferred to cryotubes (Maxxline Cryo Tubes, Dacos, Hvidovre, Denmark).
All samples were stored at −80 °C until analysis. Cortisol levels in saliva were measured by alphaLISA technology according to López-Arjona et al. (41). Serum amyloid A (SAA) and haptoglobin concentrations were obtained with commercially available kits as described by Franco-Martínez et al. (42) (VETSAA; EIKEN Chemical Co., LTD; Tokyo, Japan) and Schmidt et al. (43) (kit haptoglobin Tridelta phase range, Tridelta Development Ltd., Bray, Ireland), respectively. The serum kits showed an intra- and inter-assay imprecision lower than 15% and were linear (r > 0.91) after serial sample dilutions.
Digital circumference
2.11
The circumference of the proximal phalanges was measured using a string, which was placed at the height of the distal aspect coronary band of the dewclaws. The length of the string was then measured with a ruler to obtain the circumference. The same investigator undertook the measurements each time. Circumference was measured regularly. The first measurement was taken on the day of surgery and at regular intervals post-surgery, except in osteotomy subgroup A, where the initial casting prohibited assessment of circumference.
Statistics
2.12
Descriptive statistics was performed by applying Excel® (Microsoft Excel software version 2,504, Microsoft Corporation, Redmond, WA, USA) and GraphPad Prism (version 10.4.2 for Windows, GraphPad Software, Boston, Massachusetts USA).1
Results
3
Results are reported for implant integration and fracture fixation stability, as well as healing progression, assessed through imaging techniques (radiographs and CT). Clinical assessments, pain evaluation via facial expression and behavioural scoring systems, as well as biomarkers of stress and inflammation, were applied to provide a comprehensive evaluation of treatment efficacy and animal welfare.
Imaging assessment of fracture fixation stability and healing
3.1
Radiographic evaluation
3.1.1
Implant stability (Table 1; Supplementary Figures 4a–d): In the ostectomy 3 mm gaps, four out of four phalanges had screw loosening or breakage, and two experienced plate dislodgement. In the ostectomy 6 mm gaps, all four phalanges had screw breakage or plate dislodgement at varying time points, starting from week 4. In the osteotomies, plate dislodgment was not observed. Screw loosening or breakage occurred in 2 out of 3 phalanges in subgroup A and 2 out 4 phalanges in subgroup B.
Healing status (week 16) (Table 1; Supplementary Figures 4e–h): At week 16, three of the four digits with 3 mm gaps showed moderate bone formation, with the last showing no bridging and rounding of the fracture edges. In the digits with 6 mm gaps, none had bone formation within the gap, and all had evident rounding at the fracture edges, indicating potential non-union. In the osteotomy subgroup A, two digits retained clearly visible fracture lines, whilst one showed a barely visible line. In the osteotomy subgroup B, 2 phalanges had barely visible fracture lines, the other two had osteotomy lines that remained clearly visible.
Alignment (Table 1): In the 3 mm ostectomies, the mean change in alignment from intraoperative measurements to week 12 was 5.2° (range 0.2–7.6°) whilst the 6 mm ostectomies showed a mean change of 4.9° (0.3–11.5°). Osteotomy subgroup A and B had an average change of 3.7° (0.3–6.0) and 2.2° (0.5–4.6°), respectively.
First signs of callus (Table 1): In the ostectomy 6 mm gaps, no callus formation across the fracture gap was observed within the study period. In the ostectomy 3 mm gaps, however, callus formation was observed in 3 out 4 sheep, at week 8, 10 and 12, respectively. In contrast, in the osteotomy subgroup A and B, callus formation across the fracture area was observed in all cases, after a mean time of 9.3 weeks and 6 weeks in the subgroup A subgroup B, respectively.
Computed tomography evaluation
3.1.2
Callus thickness (Table 1): A mean callus thickness of 1.8 mm (range 1.3–2.55 mm) and 1.6 mm (range 0.85–2.18 mm) was found in the 3- and 6-mm ostectomies that showed new bone formation, respectively. In the osteotomy subgroups A and B, mean callus thickness was 2.1 mm (1.28–2.95 mm) and 1.2 mm (0.53–2.35 mm), respectively.
Clinical monitoring
3.2
First week after surgery
3.2.1
Within the first week after surgery (days 1–7), the majority of the 11 included sheep were classified as bright, alert, and responsive (130 observations out of a total of 152). The sheep generally had a good appetite during this period (143 observations of good/normal appetite out of 152). One sheep (A3) stood out as more affected after surgery with diarrhoea (days 1–8), pigmented urine (days 1 to 3), decreased general demeanour (days 1 and 2), and decreased appetite (days 1–3), all of which responded to treatment within the first week. Within the first week, six of the 11 sheep exhibited soft or watery faeces, which resolved within one to 4 days.
Within the first week after surgery, two sheep had body temperature >40 °C twice. The temperature returned to the normal range [39–40 °C, (44)] after 12–24 h and remained with reference level for the duration of the study in all sheep. Within this week, the mean heart rate was 77 beats per minute [with a range of 44 to 120 beats per minute, normal range: 70–80 (44)]. Ten sheep had heart rate >84 beats per minute (75% percentile) 1–5 times within the first week after surgery. Mean respiratory rate was 41 breaths per minute [with a range of 16–84 breaths per minute, normal range: 12–20 (44)]. Six of the sheep had a respiratory rate of >60 breaths per minute (75% percentile), measured between one and four times during this one-week period.
Body condition score and weight changes during the study period
3.2.2
According to the AWIN welfare assessment protocol for sheep (33), the body condition score of all eleven sheep ranged from 2.0 to 4.0 in the classification “Good,” throughout the study period (33). The weight changed from −4.5 kg to +3.5 kg from the starting weight. However, there were no significant difference from start to final body weight (paired t-test, p = 0.78).
Hoof block maintenance
3.2.3
The average wear life of the hoof blocks was 25 days (median: 23.5 days, interquartile range: 12–39 days), at which point they spontaneously detached from the hooves and had to be replaced.
Pain scores
3.2.4
Throughout the study period, the sheep in the ostectomy group individually scored from 0 to 3 on the CSS and individually scored from 0–3 on the SPFES (Figure 2). The sheep included in the osteotomy group individually scored from 0 to 8 on the OOPBS and individually scored from 0 to 5 on the SPFES (Figure 3).
Pain score results from the sheep with ostectomies (n = 4). The results are presented as cumulative scores, with the y-axis representing the highest attainable score (4 x the maximum score), insert graphs visualising results in detail. Note that these graphs represent only 4 animals (important for comparison with cumulative data from 7 sheep in Figure 3). (A) Sheep pain facial expression scale [SPFES; (38)] and (B) clinical severity score [CCS; (21)]. 0: All sheep scored 0.
Pain score results from the sheep with osteotomies (n = 7). The results are presented as cumulative scores, with the y-axis representing the highest attainable score (7 x the maximum score), insert graphs visualising results in detail. Note that this graph represent data from 7 sheep (in comparison to the 4 sheep in Figure 2) (A) sheep pain facial expression scale [SPFES; (38)] and (B) the ovine orthopaedic pain behaviour score (OOPBS).
The pain scores (CSS, OOPBS, SPFES) exhibited similar patterns of change over the study period, with an initial peak on days 1–2 post-surgery, then a gradual decline, and a second peak appearing 2–3 weeks after surgery (Figures 2, 3). The OOPBS provided a more detailed scoring system than the CSS.
From week eight until the end of the study period there were minimal pain scores. Occasionally a sheep scored one or two on the SPFES but with no apparent pattern (data not shown).
Lameness
3.2.5
Lameness scores were extracted from the CSS and OOPBS (Figure 4). Only one (A3) of the eleven sheep scored 3 (Figure 4); apart from this one case, the maximum lameness score was two. After week four, the lameness score declined.
Lameness scores extracted from the clinical severity score from the sheep with ostectomies (n = 4) and the ovine orthopaedic pain behaviour score from the sheep with osteotomies (n = 7). The results are presented as cumulative scores, with the y-axis representing the highest attainable score, insert graphs visualising the results in detail.
Treatment criteria
3.2.6
In the ostectomy group, SPFES treatment criterion 1, defined as a total SPFES score of 4–5 (Table 2), was reached 3 out of 448 days (4 × 112 days). In the osteotomy group, SPFES and/or OOPBS treatment criterion 1, defined as either a total SPFES sore of 4–5, a total OOPBS score of 7–12, a lameness score of 3–4, or an ‘on knees’ score of 3 (Table 2), was reached on 32 out of 742 days ((6 × 112) + (1 × 70) days). When a sheep reached treatment criterion 1, increased monitoring was initiated, and actions such as adaptation of the coaptation and/or additional analgesic treatment were taken. No sheep reached treatment criterion 2 during the study period (Table 2).
Biomarkers
3.3
Cortisol
3.3.1
In both groups, saliva cortisol baseline levels from the days prior to surgery ranged from 40.54 to 101.59 ng/mL with seemingly higher levels in osteotomy subgroup B (65.9–101.6 ng/mL) (Figures 5A,D). In the ostectomy group, cortisol levels peaked within the first week post-surgery and then declined gradually towards baseline (Figure 5A). In the osteotomy group, cortisol levels increased more slowly, with a peak at week 6, before gradually decreasing (Figure 5D).
Biomarkers measured from the sheep (n = 4) included in the ostectomy group (A–C) and from the sheep (n = 7) included in the osteotomy group (D–F). Saliva cortisol (A,D) and plasma SSA (B,E) and haptoglobin (C,F). Solid line: median. SAA, Serum amyloid A.
Acute phase proteins
3.3.2
The acute phase proteins SAA and haptoglobin exhibited an initial peak within the first few days post-surgery (Figures 5B,C,E,F), consistent with post-surgical inflammatory response. Thereafter, median levels remained low throughout the study period. In the osteotomy group, outliers were primarily represented by two animals, A3 and B3. These occasional concentration increases coincided with a bout of fever of unknow origin, lameness from loosening of hoof blocks/poorly fitting bandages, and a loose screw.
Circumference
3.4
Post-surgery, the circumference of the phalanges peaked at week 2 in the ostectomy group, followed by a decrease. From week 8 onwards, no consistent change in circumference was observed in this group (Supplementary Figures 5a,b). No obvious differences in circumference were identified between the 3- and 6- mm ostectomies. There were no consistent changes in circumference in the osteotomy group (Supplementary Figure 5).
Discussion
4
To our knowledge, this is the first large-animal fracture model specifically designed for assessing healing in small tubular bones in freely ambulating sheep. It enables the evaluation of fracture fixation and defect reconstruction strategies in a translational context, using a novel coaptation method that avoids restrictive slings to support animal welfare. The model was surgically feasible, allowed the sheep to move unrestrictedly after surgery, and enabled within animal comparisons. Implant failures occurred, demonstrating inadequate fracture fixation. However, when comparing implant stability, alignment, callus formation, and healing status at week 16, the osteotomy group showed signs of healing despite the mechanical instability. In contrast, the ostectomies were predominantly unstable, particularly the 6 mm ostectomies. Whilst the 3 mm ostectomies demonstrated moderate healing in three out of four phalanges, the 6 mm ostectomies consistently demonstrated non-healing with no callus bridging the defect. The consistent indications of non-union suggests a critical-size defect. None of the combinations of surgical approaches and coaptation methods ensured reliable healing, and these need to be refined to achieve a model with consistent healing outcomes. Use of sturdier implants and/or double plating could potentially yield more stable fixation and should be explored in future studies. Failure of repair is a common complication in large animal fracture models, with other studies main complication reported being implant failure/failure of fixation/osteotomy instability, additional one study reports spiral fracture in relation to the metal implant (16–18, 21, 24, 25, 30, 45, 46).
The overall welfare outcomes of this study were favourable, with low pain scores, limited stress responses, and acceptable recovery. In the light of increasing societal and scientific concerns regarding ethics, animal welfare, and validity of fracture research involving sheep and other experimental animals, we propose that phalangeal ostectomy and/or osteotomy could become a future welfare-oriented large animal fracture model. With further development and validation of this novel fracture model, it can provide a platform to investigate novel fracture fixation and bone healing materials and techniques to optimise treatment of small tubular bone fractures and defects.
The most effective coaptation method was not clearly identified. Offloading a diseased digit with a hoof block under the healthy digit to elevate the diseased digit is common in veterinary clinical practise in even-toed ungulates such as cattle, sheep, and goats (47) (Figure 1C; Supplementary Figure 3). In ostectomy subgroup B this led to healing in 2/4 phalanges and negated potential cast complications. However, maintaining hoof blocks proved time-consuming, as they were prone to detachment and required thorough surveillance accordingly.
Bone healing was evaluated using selected parameters from the RUST and Lane and Sandhu scoring systems, supplemented by CT-based callus measurements (36, 37). This approach was an attempt to standardise and quantify healing progression. However, due to implant failure—especially in the ostectomy 6 mm gap—bridging and callus formation were inconsistent and difficult to interpret. These scoring methods will become more applicable in future studies with enhanced mechanical stability in the model.
Surgical trauma, inflammation, pain and stress can cause changes in the biomarkers assessed in this study (48, 49). The cortisol levels peaking within the first weeks after surgery in the ostectomy group (a 1.8-fold peak on day 4, relative to baseline) might be a response to the surgical trauma. It is not clear why cortisol levels peaked later in the osteotomy group (a 1.4-fold peak in week 6, relative to baseline). The increase in cortisol experienced in the sheep in our study ranged between that found in sheep after minor stressors such as facing a dog (0.5-fold change), shearing (1.4 fold increase), or handling (1.6-fold increase) (50, 51) and major stressors such as orthopaedic surgery with tibial osteotomy (4-fold increase) (21) or mulesing, i.e., cutting crescent-shaped flaps of skin from around the breech and tail with sharp shears in the unanaesthetised animal (3-fold increase) (50).
The acute phase proteins, SAA and haptoglobin, increased rapidly in response to the surgical trauma (Figures 5B,C,E,F) (48, 49). Notably, the magnitude and pattern of this increase were comparable between the two groups, suggesting similar surgical trauma in the two groups. This is in contrast to our subjective impression that the surgical procedure in the ostectomy group was more invasive than in the osteotomy group. The phalangeal circumference increased more in the ostectomy group (Supplementary Figure 5), which could reflect the extent of surgical trauma, or a less stable osteosynthesis, with more oedema and haematoma formation the first weeks after surgery. Yet none of this was reflected in the concentrations of SAA and haptoglobin. Taken together, the biomarkers and phalangeal circumference suggest that the sheep experienced a minor-moderate surgical trauma.
The sheep recovered rapidly from anaesthesia and resumed eating within 30 min, additionally they able to ambulate freely after surgery. They had very limited expressions of pain, as this was scored as mild throughout the study period. Immediately after surgery, pain scores increased, peaked at day 2–3, and declined quickly again (Figures 2, 3). The mild pain was probably caused by the surgical trauma and/or discomfort related to post-fasting diarrhoea. A second peak in pain scores was observed around day 14 (Figures 2, 3). This may relate to the withdrawal of post-surgical NSAID treatment (administered until day 8) and underscores the importance of providing appropriate analgesia after surgery, even if it may affect bone healing (52). Use of pain scoring may thus assist in tailoring analgesic regimen post-surgically. Post-surgery pain management varies considerably in ovine orthopaedic models. One study used transdermal fentanyl for the entire duration of its 12-week study period (17), and other studies have used 10–13 days of analgesic treatments (NSAIDs, Fentanyl) (12, 21). However, the risk of gastric ulceration is a significant consideration when administering NSAIDs for a prolonged period. The majority of studies provide 3–5 days of analgesia, primarily NSAIDs and/or buprenorphine (16, 20, 23, 30, 45, 46, 53–55). It is not uncommon for studies to have no description of the analgesic treatment at all (22, 52–54). Our results suggest that 8 or more days of analgesia is needed, even with a smaller procedure such as the surgeries performed in our sheep.
Adopting strict treatment criteria (Table 2) ensured that the sheep received additional attention and pain medication if needed, and that no sheep experienced moderate or severe pain. Especially the a priori weighted composite OOPBS was of great benefit, as it entailed sensitive scoring system and treatment criteria (Tables 2, 3; Figures 2B, 3B), ensuring that even few expressions of pain prompted additional attention to the sheep and/or pain medication. Using an a priori weighted composite pain score such as the OOPBS offers the advantage of reduced subjectivity, as each category is clearly defined and pre-weighted. This enhances reproducibility and establishes the score as a valid tool for longitudinal pain assessment (56) and for comparison across studies or animals evaluated using the same scoring system.
For animal experiments to retain social licence to operate it is of the utmost importance that experimental animal welfare is high and pain is kept to a minimum and reporting is transparent (28) – and that there is appropriate reporting on these aspects of the experiment. In fracture and bone healing research there is an appalling paucity of reporting on the experimental animals’ clinical status, welfare, and pain manifestations. One fairly recent study on tibial osteotomy directly reports these data, including stress biomarkers, which were part of the study’s stated objectives (21), but otherwise welfare-related data are usually not described at all or only with few sentences (17–20, 45, 46, 53–55, 57–59). Some papers describe methods for pain assessment in the materials and methods section of the paper but fail to report the results (16, 25). A recent review of large animal models in articular cartilage repair similarly observed a void of information on pain management and monitoring in most published papers (26). Although the ARRIVE guidelines2 are available, there seems to be a need for journals reinforcing standardised and consistent reporting of pain and welfare of sheep and other large animals in orthopaedic research. Inadequate or incomplete reporting on experimental animal health and welfare is not only an ethical issue but may also lead to issues with reliability of the obtained data. Long-term stress, sustained pain, disease, or injuries can affect healing (60) and interpretation of the results, with potential negative impact on reliability and outcome measures of the study.
Pain recognition in animals through behavioural and facial expressions, has been a subject of scientific attention in several species for decades, building on foundational work by Darwin in 1872 (61). Thorough observation is necessary, as many prey animal species will do their utmost to hide pain, disease and weakness (62). Using facial expressions to recognise pain is common in veterinary practise and experimental animal research, and tools has been developed for numeral species (63). Methods for assessing welfare and pain in sheep have been reported and refined for several decades (21, 38, 56). The SPFES was validated by McLennan et al. (38) in sheep suffering from mastitis or footrot, and we found that the SPFES was easy to use and applicable in sheep in orthopaedic research. In future pain assessment of animals, artificial intelligence (AI) will most likely play a considerable role, as a recent study reports, that an AI tool significantly outperformed experienced veterinarians in recognising pain in sheep using the SPFES (38, 63).
Taken together, it is our impression that the OOPBS and the SPFES were easy to apply, and, when combined with the treatment criteria, they served as valuable clinical tools for assessing acute pain, documenting accumulated pain over time, gauging model severity, and for identification of animals in need of extra attention and/or pain medication. It is, however, important to acknowledge that confirmation bias may have affected the pain scores. Pain scoring was performed by direct observation of the sheep, and the principal investigators were therefore not blinded and were directly involved in implementing the therapeutic plan. Video-based pain scoring would minimise the influence by human presence on animal behaviour and allow for blinded assessments.
Conclusively, this study represents a first step towards developing a bilateral ovine proximal phalanx fracture and defect model with a comprehensive welfare monitoring plan. Ostectomy with 3–6 mm gaps lead to minimal or no healing, whilst osteotomy in combination with a 4.5 mm drill hole healed in some instances after repair with 1.5 mm 5-hole locking plates. To obtain consistent healing adjustments to the model are needed to fully accommodate the dynamic loading of the fracture site. However, the model concept is promising, and a modified model may provide translational insights into fracture healing and orthopaedic implant performance in smaller tubular bones. Importantly, pain scores remained low and the sheep moved freely in their pens, supporting the model’s feasibility from an animal welfare perspective. Moreover, the bilateral design allows paired comparisons, and from an experimental animal ethical standpoint it is desirable that the model allows reduced animal numbers and that welfare outcomes were favourable.
Additionally, with this study we challenge the current approach to animal welfare monitoring in sheep used in orthopaedic research. We have shown that qualitative and quantitative data on pain, stress, and welfare can and should be reported alongside parameters such as bone healing. Ensuring proper welfare monitoring and reporting are essential for both scientific integrity and societal acceptance of research involving animals.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wu AM Bisignano C James SL Abady GG Abedi A Abu-Gharbieh E. Global, regional, and national burden of bone fractures in 204 countries and territories, 1990–2019: a systematic analysis from the global burden of disease study 2019. Lancet Healthy Longev. (2021) 2:e 580–92. doi: 10.1016/S 2666-7568(21)00172-0, PMID: 34723233 PMC 8547262 · doi ↗ · pubmed ↗
- 2van Leerdam RH Krijnen P Panneman MJ Schipper IB. Incidence and treatment of hand and wrist injuries in Dutch emergency departments. Eur J Trauma Emerg Surg. (2022) 48:4327–32. doi: 10.1007/S 00068-021-01732-X, PMID: 34196727 PMC 9712291 · doi ↗ · pubmed ↗
- 3De Putter CE Selles RW Polinder S Panneman MJM Hovius SER Van Beeck EF. Economic impact of hand and wrist injuries: health-care costs and productivity costs in a population-based study. J Bone Joint Surg. (2012) 94:e 56. doi: 10.2106/JBJS.K.00561, PMID: 22552678 · doi ↗ · pubmed ↗
- 4de Haas LE Mvan Lücht VAP Hoorn BT Salentijn DA Groenwold RHH Schep NWL. Patient-reported outcomes three months after treatment of metacarpal and phalangeal fractures or dislocations: a multicentre snapshot study. Bone Jt Open. (2025) 6:227–36. doi: 10.1302/2633-1462.62.BJO-2024-0146.R 1, PMID: 40008527 PMC 11863288 · doi ↗ · pubmed ↗
- 5Roennegaard AB Jensen SS Tengberg PT Gundtoft PH Viberg B. Risk of secondary surgery following surgical treatment of fractures: a nationwide register study on 9, 719 adult patients. Acta Orthop. (2025) 96:304–9. doi: 10.2340/17453674.2025.43446, PMID: 40223675 PMC 11995429 · doi ↗ · pubmed ↗
- 6Wellborn PK Allen AD Draeger RW. Current outcomes and treatments of complex phalangeal and metacarpal fractures. Hand Clin. (2023) 39:251–63. doi: 10.1016/j.hcl.2023.02.002, PMID: 37453755 · doi ↗ · pubmed ↗
- 7Dargan D Wyman M Bhoora M Ronan D Baker M Partridge D. Hand osteomyelitis: a systematic review of the literature and recommendations for diagnosis and management. Hand. (2024). doi: 10.1177/15589447241284408, PMID: 39462293 PMC 11559780 · doi ↗ · pubmed ↗
- 8Lazerges C Degeorge B Coulet B Chammas M. Diagnosis and treatment of hand tumors. Orthop Traumatol Surg Res. (2022) 108:103153. doi: 10.1016/J.OTSR.2021.103153, PMID: 34838755 · doi ↗ · pubmed ↗