Arterialized oxygen tension and unfavorable clinical outcomes in pediatric cystic fibrosis
René Gaupmann, Saskia Gruber, Klara Schmidthaler, Bianca Pauger, Brigitte Mersi, Alexandra Graf, Zsolt Szépfalusi, Sabine Renner, Eleonora Dehlink

TL;DR
Low oxygen levels in young cystic fibrosis patients predict faster lung function decline and more complications, suggesting a need for early monitoring.
Contribution
Arterialized oxygen tension at age 5 is shown to predict future lung function decline and CF-related complications beyond spirometry.
Findings
Low pO2 at age 5 correlates with accelerated FEV1 decline in CF patients.
Early low pO2 increases the risk of allergic bronchopulmonary aspergillosis and other CF-related complications.
pO2 is inversely related to lung clearance index and positively to FEV1.
Abstract
Maintaining good lung function is a primary goal in managing Cystic Fibrosis (CF). As spirometry lacks sensitivity for detecting mild lung disease, early progression often remains unrecognized. To overcome this limitation, more sensitive monitoring tools are needed. We evaluated arterialized oxygen tension (pO2) as an easily accessible, and widely applicable surveillance method. In this retrospective observational single-center cohort study, arterialized gas exchange was assessed in 103 young people with CF (47 females, 56 males, aged 5–18 years). Trends from baseline (age 5 years) to early adulthood and performance relative to annual best pulmonary function (FEV1) and lung clearance index were examined, along with baseline oxygen tension's predictive value on future FEV1 decline and the occurrence of CF-related complications. pO2 correlated significantly with FEV1 (p < 0.001) and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
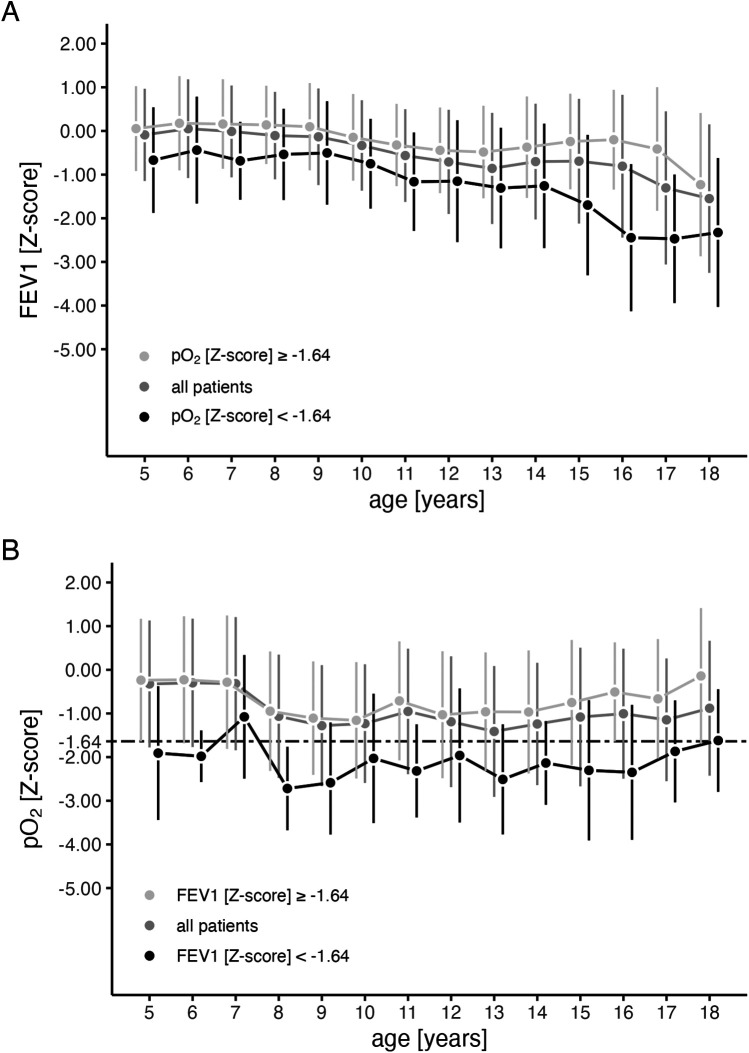 Figure 1
Figure 1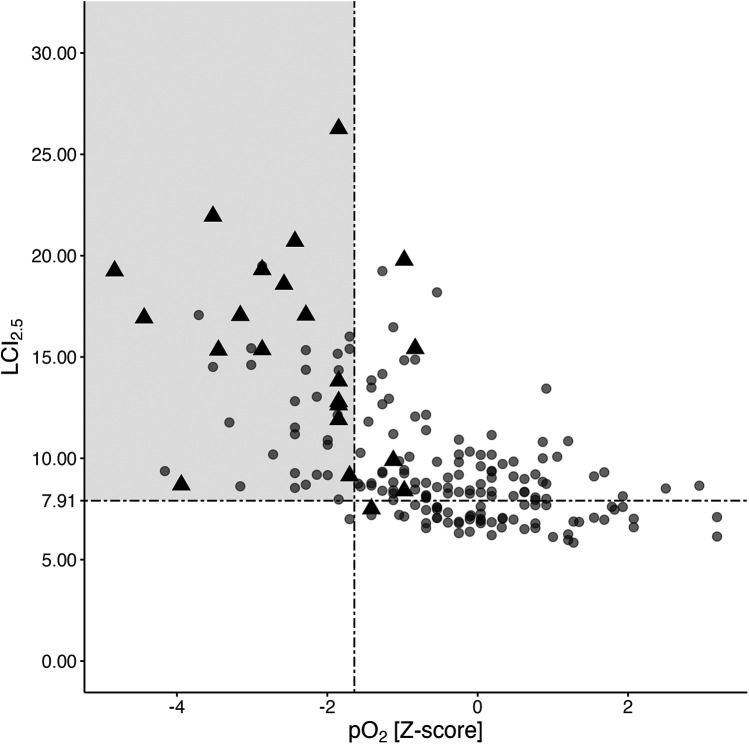 Figure 2
Figure 2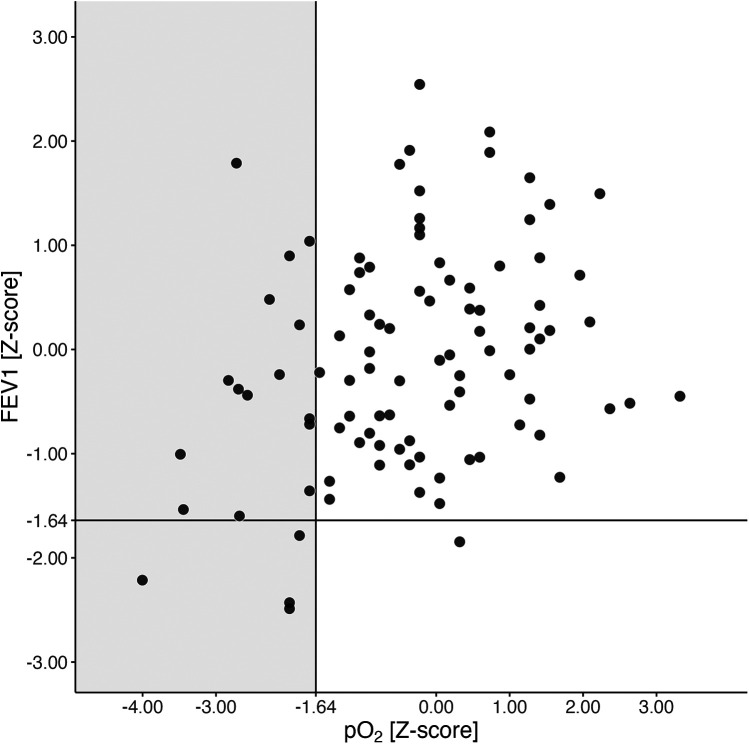 Figure 3
Figure 3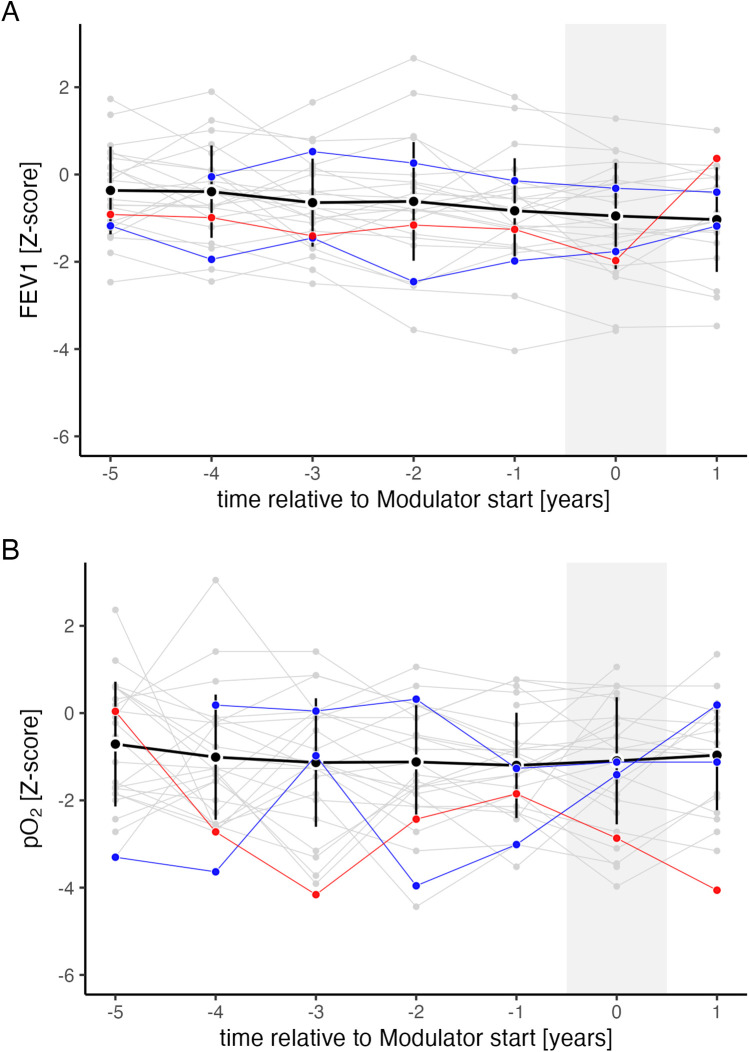 Figure 4
Figure 4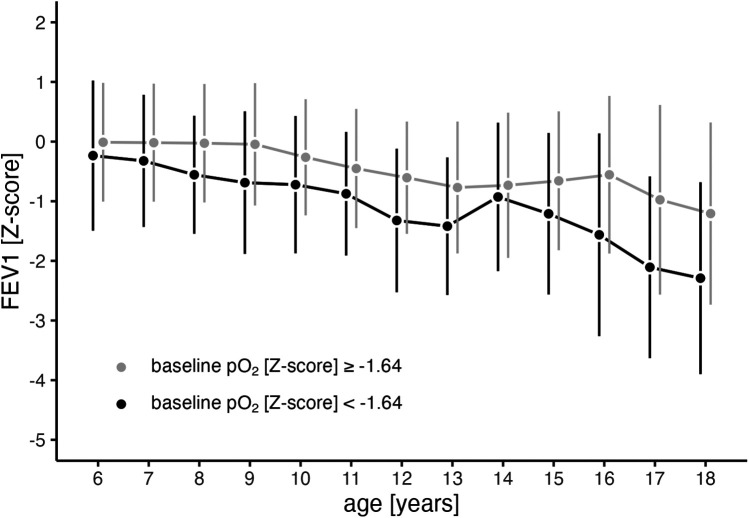 Figure 5
Figure 5| Patients under observation (N) | 103 |
| Blood gas samples in total (N) | 923 |
| Blood gas samples per patient | 9 (1–14) |
| SaO2 ≥ 93% at sampling timepoint (N) | 923 (100%) |
| Observational period [years] | 8.1 (4.0) |
| Sex | |
| Female | 47 (45.6%) |
| Male | 56 (54.4%) |
| Genotype | |
| high-risk | 86 (83.5%) |
| low-risk | 10 (9.7%) |
| Unknown | 7 (6.8%) |
| Pancreas insufficiency | 87 (84.5%) |
| CFTR modulator therapy at any time during the observation | 29 (28.1%) |
| Dual CFTR modulator therapy | 26/29 (89.7%) |
| HEMT | 3/29 (10.3%) |
| chronic PsA infection ≤5 years | 10 (9.7%) |
| ABPA ≤ 5 years | 1 (0.97%) |
| CFRD ≤ 5 years | 0 (0%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCystic Fibrosis Research Advances · Neonatal Respiratory Health Research · Tracheal and airway disorders
Introduction
1
Cystic Fibrosis (CF) is an autosomal recessive disorder affecting approximately 1 in 3,500 Caucasian newborns (1). It results from a dysfunction in the CF transmembrane conductance regulator (CFTR) protein, causing thickened mucus and impaired airway clearance (2). Structural lung changes begin early, even in infancy, well before clinical symptoms appear or spirometry can detect them (3, 4). Early diagnosis and intervention are crucial to interrupt the cycle of inflammation, infection, and lung damage, thereby mitigating disease progression (3–5). Early identification of high-risk individuals allows early intervention to optimize long-term outcomes (5).
Spirometry is the preferred method for monitoring CF-related lung disease progression (6, 7). However, spirometry has certain limitations. Firstly, it can only be performed from a certain age, typically school age and older, as it relies on adequate cooperation (8). Secondly, spirometry lacks sensitivity in detecting very early or mild lung disease (3). Alternative techniques, such as computed tomography or magnetic resonance imaging of the chest or multiple breath washout, may identify structural or functional lung changes earlier in the disease course than spirometry. However, these alternatives have associated concerns, including radiation exposure, the need for anesthesia to prevent motion artifacts, and limitations in availability and costs (9). Thus, the optimal methods for detecting early lung parenchymal and functional changes remain unclear (3).
As the lungs' primary role is oxygen uptake, measuring arterial oxygen tension appears to be a viable option for further exploration (10). While pulse oximetry is non-invasive, its correlation with arterial oxygen tension is poor (11). In pediatric settings, arterial puncture is impractical, but arterialized capillary blood sampling is a reliable alternative. Arterialized capillary oxygen tension (pO_2_) offers a highly accurate estimation, as a suitable substitute for true arterial oxygen levels (11–13). Kraemer et al. investigated longitudinal pO_2_ progression in young people with CF (PwCF) and found that pO_2_ trends paralleled those of FEV1, with both showing a decline until early adulthood (14, 15). Since low FEV1 at a young age is associated with a more severe clinical course in PwCF, we hypothesized that pO_2_ might follow a similar pattern (5).
This retrospective observational study evaluated the role of pO_2_ as an additional marker for pediatric CF lung disease and its potential for risk stratification, focusing on whether low pO_2_ at a young age is associated with a worse clinical course.
Methods
2
Study design and population
2.1
This retrospective observational single-center cohort study included individuals newly diagnosed with CF after the nationwide newborn screening program's implementation in October 1997, until the analysis in December 2020. Eligible PwCF were under the care of the pediatric CF center at the Medical University of Vienna.
PwCF had to be over 5 years of age at enrolment, with their annual best pulmonary function tests (best FEV1), concurrently sampled arterialized capillary blood gases and multiple breath washout maneuvers (MBW) reviewed up to the age of 18. PwCF under 5 years of age who might be unable to perform spirometry accurately, and those after solid organ transplantation were excluded from analysis. Associations were analyzed for pO_2_, FEV1, and LCI_2.5_ when available (introduced in 2015). To evaluate the potential for risk stratification and prediction of future clinical outcomes, we analyzed the longitudinal progression of FEV1 and the time to onset of CF-related complications—previously shown to be associated with an unfavorable disease course—stratified by dichotomized pO₂ at age 5 (normal vs. abnormal). All necessary data were extracted from medical records. An explanatory flowchart is shown in Supplementary Figure 1 in the online supplement.
The study protocol was approved by the local ethics committee, adhering to the Declaration of Helsinki and Good Clinical Practice. Due to the retrospective study design, no informed consent was required before the medical records were reviewed.
Pulmonary function tests
2.2
Spirometry followed the European Respiratory Society guidelines using the MasterScreen Body (Vyaire Medical, Mettawa, Illinois, USA, Software: Sentry Suite) (16). Forced expiratory volume in the first second (FEV1) was reported in Z-scores using the Global Lung Initiative normative dataset (17).
The lung clearance index (LCI_2.5_) was derived from nitrogen multiple breath washout using the ExhalyzerD system (EcoMedics, Duernten, Switzerland, Software: Spiroware Version 3.2.2), adhering to the standardized protocol outlined in the consensus statement (18). LCI_2.5_ has been routinely obtained at our CF center since 2015. As introduced by Anagnostopoulou et al., 7.91 was considered the upper limit of normal (19, 20).
Capillary blood sampling and blood gas analysis
2.3
Blood gas sampling from the earlobe preceded pulmonary function tests at every outpatient visit starting from the third spirometry, typically around the age of 5 years. Local capillary blood circulation was increased using topical nonyl vanillamide and nicotinic acid-β-butoxyethyl ester containing ointment (Finalgon®, Sanofi, Paris, France). After 15 min incubation time, capillary blood was collected in heparinized plastic capillaries and immediately analyzed for oxygen tension (pO_2_) in mmHg at room temperature using an ABL800 FLEX blood gas analyzer (Radiometer Medical ApS, Copenhagen, Denmark). The analyzer was located in the same room, ensuring a short transfer time. pO_2_ values were converted into Z-scores based on pediatric normative data from Gaultier et al. (13). The lower limit of normal (LLN) for pO_2_ was defined as the 5th percentile of a healthy pediatric population, corresponding to a Z-score of −1.64 (5–8 years: 80 mmHg; ≥8 years: 84.3 mmHg).
The sampling technique was highly accepted, with a 100% acceptance rate among all 5-year-olds included in the study.
Definition of CF-related complications
2.4
The modified Leeds criteria were applied to define chronic Pseudomonas aeruginosa (PsA) airway infection using surveillance microbiology airway samples (21). CF-related diabetes (CFRD) was defined by a pathological oral glucose tolerance test (OGTT), routinely performed annually from the age of 10 during routine follow-ups when patients were in a stable health condition (6). Allergic bronchopulmonary Aspergillosis (ABPA) episodes were diagnosed based on the Cystic Fibrosis Foundation Consensus, as described elsewhere (22).
Statistics
2.5
Data analysis was conducted using R software, version 4.3.2 (The R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics included absolute numbers and percentages for categorical data, while quantitative parameters (ages 5–18) were presented as mean ± SD. Linear mixed models with a random patient effect were used to assess differences and the progression of serial measured variables. To evaluate CFTR modulator effects, a binary factor was included to compare measurements before vs. after modulator initiation.
To assess the impact of pO_2_ at age 5 on the future clinical course, the dataset was split into two groups: pO_2_ Z-score ≤1.64 vs. pO_2_ Z-score ≥−1.64. Baseline data were compared using t-tests for continuous variables and Fisher's exact tests for categorical data. The future FEV1 time course was analyzed using a two-step approach: (1) simple linear mixed-effect models with random patient effects for our baseline grouping variable and potential confounders [age, year of birth, sex, pancreatic insufficiency, genotype, baseline FEV1, body mass index (BMI) at age 5, first and chronic PsA infection before age 5, chronic Staphylococcus aureus infection before age 5 and CFTR modulator therapy], followed by (2) a multivariable linear mixed-effect model, including all significant factors from the simple models (more detailed in the online supplements' statistics section) (5). To investigate the impact of early hypoxemic states on the probability for CF-related diseases (ABPA, CFRD, chronic PsA infection), Kaplan–Meier and univariable Cox regression models were employed. The level of significance was set to <0.05.
Results
3
Study population
3.1
Among 150 eligible young PwCF, 47 were excluded. Of the remaining 103 (47 females and 56 males) aged 5–18, 923 arterialized blood gases were reviewed. Patient numbers and examinations by age group are detailed in Supplementary Table 1 in the online supplement. The mean observational period was 8.1 ± 4.0 years. Of the 103 patients, 87 (84.5%) were pancreatic-insufficient, 29 (28.1%) received CFTR modulator therapy at some point during the observational period; none received modulators before the age of 6 years. 10/103 (9.7%) patients were considered chronically infected with PsA and one patient was diagnosed with ABPA as early as age 5. A detailed overview of patients' characteristics at baseline is provided in Table 1 (23).
Pulmonary function and gas exchange during childhood and adolescence
3.2
Within the study cohort, pulmonary function (FEV1) showed a significant decline from early childhood to adulthood (p < 0.001, Figure 1A). While the mean arterialized pO_2_ remained stable above the lower limit of normal (Z-score of −1.64) across all age groups, lower pO_2_ values were observed in PwCF with lower FEV1 values (p < 0.001, Figure 1B). For further analysis, PwCF with pO_2_ below a Z-score of −1.64 were classified as “hypoxemic”, while those with values equal to or above −1.64 were classified as “normoxemic”.
Progression of arterialized oxygen tension (pO2) and FEV1 during childhood and adolescence. Mean values (points) and standard deviations (vertical lines) for FEV1 (A), and pO2 (B) are shown across age groups for all patients (grey) and stratified by whether the corresponding pO2 (A) or FEV1 (B) falls above (light grey) or below (black) −1.64 Z-scores. Mean values were calculated based on the actual number of patients in each age group. The number of patients is detailed in Supplementary Table 1 in the online supplement.
Pancreatic sufficient PwCF tended to have higher average pO₂ values across all age groups (p = 0.069), while levels did not differ by sex or chronic PsA airway infection (defined for each age group in Supplementary Table 1, online supplement), as illustrated in Supplementary Figure 2 (online supplement).
pO2 in relation to LCI2.5 and FEV1
3.3
A total of 188 nitrogen multiple breath washout maneuvers from 85 young PwCF, spanning ages 6–18 years and obtained concurrently with blood gas sampling and spirometry, were analyzed (more detailed in Supplementary Table 1 in the online supplement). Lower pO_2_ values were associated with higher LCI_2.5_ across all ages (Figure 2, linear mixed model: estimate −1.09, 95%−CI: −1.38 to −0.81, p < 0.001). LCI_2.5_ was pathologically high in 133 out of 188 measurements, with 45 (33.8%) showing hypoxemia in arterialized blood gases, while FEV1 Z-score being below −1.64 in only 21 (15.8%) cases (Figure 2). Forty-four out of 45 PwCF (98%) with hypoxemia had an LCI_2.5_ exceeding 7.91, while only one individual hat a normal LCI_2.5_ (2%).
Association of corresponding LCI2.5, pO2, and FEV1 values. Distribution of LCI2.5 and pO2 values from a total of 188 N2BMW maneuvers and corresponding blood gas analyses from 85 PwCF aged 6 to 18 years (see Supplementary Table 1 in the online supplement for age distribution). Black triangles represent individuals with poor pulmonary function (FEV1 Z-scores <−1.64), whereas the grey circles indicate individuals with normal FEV1 at the time of assessment. The grey rectangle indicates a pathologically high LCI2.5 (>7.91) combined with a concurrently low pO2 Z-score (<−1.64). FEV1, forced expiratory volume in the first second; LCI2.5, lung clearance index; N2MBW, nitrogen multiple breath washout; pO2, arterialized oxygen tension; PwCF, people with CF.
pO2 at the age of 5 years
3.4
Seven out of the total cohort of 103 PwCF lacked sufficient data before the age of 5 years, either due to late diagnosis or because they transferred to our center at later ages. Among the remaining 96 patients at 5 years of age, the mean FEV1 Z-score was −0.09 ± 1.056 (SD), corresponding to 98.8 ± 13.5% predicted. Supplementary Table 2 in the online data supplement provides a more detailed overview of patients' characteristics at the age of 5 years.
Five of 96 (5.2%) had FEV1 values below the lower limit of normal, while 19 of 96 (19.8%) were already hypoxemic at this early age (as depicted in Figure 3). Compared to normoxemic PwCF, the hypoxemic group tended to be female, with 12 out of 19 (63.2%, p = 0.091), and had significantly lower FEV1 values (p = 0.021, see Supplementary Table 2 in the online data supplement).
FEV1 and pO2 at the age of 5 years. pO2 and FEV1 Z-scores at the age of 5 years are shown. The black lines represent the lower limits of normal (LLN) for both pO2 and FEV1 Z-scores. The grey rectangle indicates hypoxemic 5-year-olds (pO2 Z-score <−1.64, equivalent to 80 mmHg). Abbreviations used: FEV1 (forced expiratory volume in the first second), N (number of patients), pO2 (arterialized oxygen tension), PwCF (people with CF).
Impact of CFTR modulator therapy on FEV1 and pO2 trend
3.5
The proportion of PwCF receiving CFTR modulator therapy increased with age, ranging from 7% to 25% among patients aged 10–18 years (Supplementary Table 1, online supplement). Figure 4 shows FEV1 and pO₂ trends before and after CFTR modulator initiation. Among individuals on dual CFTR modulators (ivacaftor/lumacaftor or ivacaftor/tezacaftor), no significant change in FEV1 was observed (estimate: −0.56; 95% CI: −4.23 to 3.11; n.s.), whereas pO₂ showed a slight improvement (estimate: 0.46; 95% CI: 0.01–0.91; p = 0.044). For the three PwCF on Highly Effective Modulator Therapy (HEMT), statistical analysis was not performed due to the small sample size; these patients were followed only until modulator initiation in the prediction model.
FEV1 and pO2 trend relative to CFTR modulator introduction. Progression of FEV1 (A) and pO₂ (B) relative to CFTR modulator introduction, expressed in years before (−) and after () initiation. Shown are mean values (black points) and standard deviations (black vertical lines) for all individuals on ivacaftor/lumacaftor or ivacaftor/tezacaftor. Individual trajectories are shown separately for each person with CF (PwCF) on ivacaftor/lumacaftor or ivacaftor/tezacaftor (grey, n = 26), ivacaftor monotherapy (blue, n = 2), and the triple combination of elexacaftor/tezacaftor/ivacaftor (red, n = 1).
Association between early low pO2 and clinical course
3.6
Being hypoxemic at the age of 5 years was significantly associated with future FEV1 loss within our study. Compared to individuals with normal pO_2_, Z-scores below −1.64 (equivalent to 80 mmHg) at this early stage were associated with a subsequent steeper decline in FEV1 (p < 0.001, estimate = −0.06, 95%−CI: −0.09 to −0.02, Figure 5). This association remained significant even in the multivariable model, adjusted for other significant influencing factors on the FEV1 course from the simple models, such as genotype, pancreatic insufficiency, chronic PsA infection before age 5, FEV1 at baseline, year of birth, and CFTR modulator use (calculations and estimates are provided in the statistics part of the online supplement and Supplementary Table 4).
Trajectory of FEV1 in relation to pO2 at 5 years (baseline). Mean values (points) and standard deviations (vertical lines) for FEV1 progression from ages 6 to 18 years are shown separately for individuals with abnormal pO2 Z-score (<−1.64, black line) and those with normal pO2 Z-score (≥−1.64, grey line) at baseline (age 5). At age 5, a pO2 Z-score of −1.64 corresponds to 80 mmHg. FEV1 (forced expiratory volume in the first second), pO2 (arterialized oxygen tension).
The number of observed CF-related complications during the observational period is provided in Supplementary Table 3 in the online supplement. Five-year-olds with hypoxemia in arterialized blood gases were significantly more likely to experience an ABPA episode compared to those with normoxemia [HR: 7.69, 95% CI: 2.22–25, p = 0.001; see Supplementary Figure 3A in the online supplement]. A similar trend was observed for the onset of CFRD and the acquisition of chronic PsA infections in hypoxemic states at age 5 [CFRD: HR: 2.78, 95%−CI: 0.96–7.69, p = 0.06; PsA: HR: 2.38, 95%−CI: 0.87–6.67, p = 0.09; see Supplementary Figures 3B, C in the online supplement].
Discussion
4
In this study, we assessed pO_2_ in arterialized blood as an easily accessible, and widely applicable method for monitoring lung disease and identifying patients at risk of a more severe disease course. In the analyzed CF cohort, pO_2_ remained stable from 5 to 18 years, which contrasts with the longitudinal decline in FEV1 observed in young PwCF. Dual CFTR modulators positively influenced the pO₂ trajectory, whereas its levels were independent of pancreatic function, sex, and chronic Pseudomonas aeruginosa infection. While most children (94.8%) had normal lung function at age 5, 19.8% already showed abnormally low pO_2_. These children experienced a greater decline in FEV1 during childhood and adolescence and faced a higher risk of CF-related complications such as ABPA, CFRD, and chronic PsA infections.
The longitudinal pO_2_ progression in our study diverges from previously published data on pO_2_ (14, 15). In the study of pediatric PwCF by Kraemer and colleagues, pO_2_ values were notably lower and exhibited a linear decline during childhood, starting at 80.7 ± 1.9 mmHg at 5 years of age and decreasing to a mean of 69.9 ± 1.6 mmHg at age 18 years (14). This discrepancy may be attributed mainly to the inclusion of pre-symptomatic children through newborn screening in the present study, the generally improved overall health of individuals with CF in recent years, and the use of CFTR modulators. The latter may also partially explain the slightly increasing pO₂ trend observed in our older adolescents. To our knowledge, this is the first study to evaluate the impact of any generation of CFTR modulator therapy on pO₂.
In pediatrics, hypoxemia is rarely defined by arterial or arterialized pO_2_; instead, it is more commonly characterized as transcutaneous oxygen saturation falling below 90% or 93%, depending on the child's age (24). Notably, within our cohort, even PwCF having hypoxemic pO_2_ values exhibited arterialized oxygen saturation above 93%. We did not measure transcutaneously, but there is a strong correlation between arterial oxygen saturation and transcutaneous oxygen saturation (25). Abnormal pO₂ despite normal oxygen saturation aligns with the physiology of the oxygen-hemoglobin dissociation curve, which flattens at higher pO₂ levels. Even when pO₂ falls below the lower limit of normal (5th percentile), oxygen saturation may remain within the normal range (26, 27). We therefore propose arterialized pO₂ as a more accurate surrogate marker of oxygenation than oxygen saturation.
Predicting disease progression is crucial for identifying PwCF who may benefit from more aggressive surveillance strategies or therapeutic interventions (5, 28). FEV1 remains the most significant predictor of mortality and early CF lung disease progression (5). However, especially in the era of highly potent CFTR modulators, the proportion of patients with pulmonary function within the normal range is increasing (29). FEV1 alone may not provide a comprehensive assessment of lung damage, particularly in cases of milder CF lung disease or during the subclinical period from birth to school age, when disease progression can occur without noticeable symptoms and spirometry is unreliable (3, 4, 30, 31). While we cannot draw conclusions for the subclinical period of infancy as children under 5 years were excluded from this study, pO₂ may offer significant advantages as an adjunct to traditional spirometry, particularly in mild CF lung disease.
Blood oxygen tension primarily depends on oxygen uptake and the lung's ability to transfer oxygen into the bloodstream independent of factors such as sex, age, anthropometrics and ethnicity (10, 32). Ventilatory inhomogeneity and the simultaneous increase in dead space ventilation may play a significant role in gas exchange abnormalities among pediatric PwCF (14, 31). Over the last decade, multiple breath washout, serving as a marker for ventilatory inhomogeneity, has emerged as a promising method for monitoring early or mild CF lung disease (33). Not only does it serve as a more sensitive marker for early structural lung damage compared to FEV1, but abnormal LCI_2.5_ in early childhood have also been demonstrated to predict poor pulmonary function during school years (3, 34, 35). In our study, low pO_2_ was associated with high LCI_2.5_, suggesting a potential indication of poor oxygenation due to ventilatory inhomogeneity. Moreover, low pO_2_ showed greater sensitivity in detecting LCI_2.5_ values above 7.9 compared to low FEV1, with sensitivity increasing from 0.18 for FEV1 to 0.45 for pO_2_. This suggests that blood gas analysis could be a more sensitive method for detecting mild CF lung disease than spirometry.
Limitations of our study are the limited generalizability of our results due to the retrospective design of the study. Additionally, outcomes may have been influenced by the evolving landscape of new treatment approaches, particularly the widespread availability of Highly Effective Modulator Therapy over the last years, especially among young children. Our findings must be confirmed in prospective studies involving PwCF on triple CFTR modulator therapy. This is particularly relevant as most PwCF on triple therapy have normal FEV1 (29).
While we do not advocate the use of pO_2_ as a direct substitute for LCI_2.5_ or spirometry, it is worth noting that multiple breath washouts can be laborious and resource-intensive, particularly in very young children (35). Our data suggest that pO_2_ is a more sensitive marker than FEV1 for mild CF lung disease and, hence, could serve as an easily accessible, and widely applicable addition to established monitoring tools to identify young PwCF at increased risk of a more severe disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Frischer T Eber E Ellemunter H Zacharasiewicz A Kaluza I Riedler J Cystic fibrosis in Austria. Wien Klin Wochenschr. (2017) 129(15–16):527–32. 10.1007/s 00508-017-1179-x 28236043 · doi ↗ · pubmed ↗
- 2Brown SD White R Tobin P. Keep them breathing: cystic fibrosis pathophysiology, diagnosis, and treatment. JAAPA. (2017) 30(5):23–7. 10.1097/01.JAA.0000515540.36581.9228441669 · doi ↗ · pubmed ↗
- 3Grasemann H Ratjen F. Early lung disease in cystic fibrosis. Lancet Respir Med. (2013) 1(2):148–57. 10.1016/S 2213-2600(13)70026-224429095 · doi ↗ · pubmed ↗
- 4Ramsey KA Ranganathan S Park J Skoric B Adams AM Simpson SJ Early respiratory infection is associated with reduced spirometry in children with cystic fibrosis. Am J Respir Crit Care Med. (2014) 190(10):1111–6. 10.1164/rccm.201407-1277 OC 25321321 · doi ↗ · pubmed ↗
- 5Breuer O Caudri D Stick S Turkovic L. Predicting disease progression in cystic fibrosis. Expert Rev Respir Med. (2018) 12(11):905–17. 10.1080/17476348.2018.151940030173593 · doi ↗ · pubmed ↗
- 6Castellani C Duff AJA Bell SC Heijerman HGM Munck A Ratjen F ECFS best practice guidelines: the 2018 revision. J Cyst Fibros. (2018) 17(2):153–78. 10.1016/j.jcf.2018.02.00629506920 · doi ↗ · pubmed ↗
- 7Burgel PR Southern KW Addy C Battezzati A Berry C Bouchara JP Standards for the care of people with cystic fibrosis (CF); recognising and addressing CF health issues. J Cyst Fibros. (2024) 23(2):187–202. 10.1016/j.jcf.2024.01.00538233247 · doi ↗ · pubmed ↗
- 8Ranganathan S Linnane B Nolan G Gangell C Hall G. Early detection of lung disease in children with cystic fibrosis using lung function. Paediatr Respir Rev. (2008) 9(3):160–7. 10.1016/j.prrv.2008.05.00218694707 · doi ↗ · pubmed ↗