A 9 year retrospective review of motorcycle accidents at a level 1 trauma center in Riyadh
Hussam Alhathlol, Khalid Alsikhan, Turki Alharbi, Ibrahim Alsamaani, Ali Alhathloul, Rifan Alyami

TL;DR
This study examines motorcycle accident patterns and outcomes at a Saudi trauma center, highlighting the risks faced by young male riders and the need for improved safety measures.
Contribution
A 9-year retrospective analysis of motorcycle accident injuries and outcomes in Saudi Arabia, focusing on demographics and injury patterns.
Findings
Young males aged 18–35 were the most affected group in motorcycle accidents.
Fractures and brain injuries were the most common injuries, with high rates of surgical intervention.
Head, chest, and facial injuries were significantly associated with ICU admission and intubation.
Abstract
Motorcycle accidents are a significant cause of morbidity and mortality worldwide, with an increasing trend observed in Saudi Arabia. These accidents often result in severe injuries, leading to long-term disability or death, highlighting the need for better understanding and management in trauma centers. These findings highlight the vulnerability of motorcyclists on the roads and underscore the critical need to address motorcycle safety in order to reduce the burden of road traffic accidents. This retrospective study assessed the rate, injury patterns, and outcomes of motorcycle accidents at King Abdulaziz Medical City (KAMC) in Riyadh, a level 1 trauma center, from January 2016 to December 2024. A total of 415 adult patients were included, with data on demographics, injury types, and treatment outcomes collected from hospital records. Multivariable logistic regression was performed to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
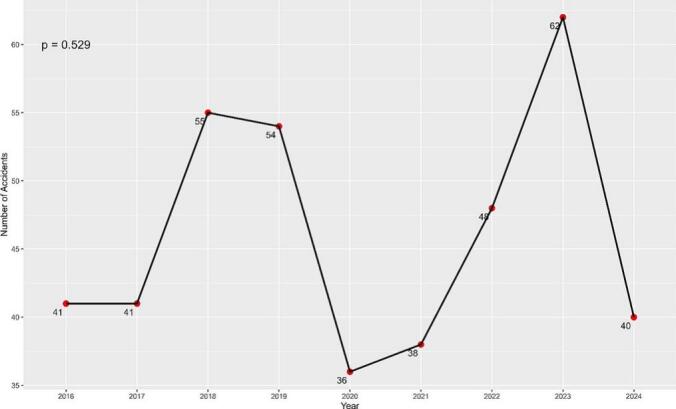 Figure 1
Figure 1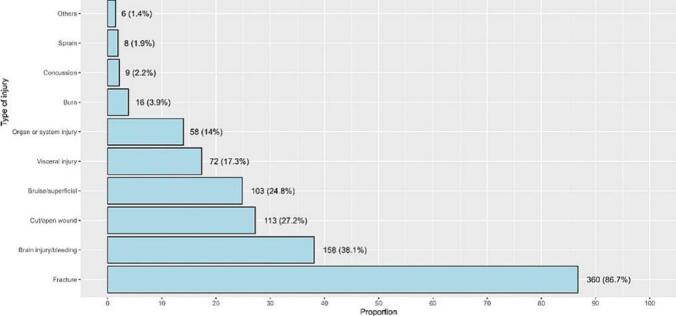 Figure 2
Figure 2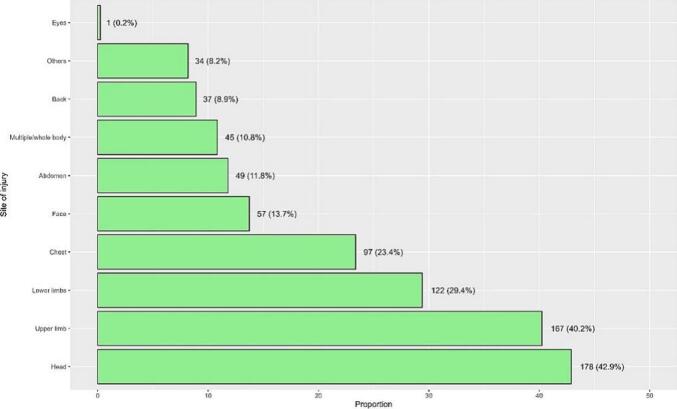 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraffic and Road Safety · Injury Epidemiology and Prevention · Trauma and Emergency Care Studies
Introduction
Road traffic injuries are a very common and critical cause of morbidity and mortality around the world [1]. Globally, road traffic crashes cause approximately 1.19 million deaths annually according to the World Health Organization [2]. Moreover, road traffic crashes cost most countries 3 % of their gross domestic product causing significant economic burden [2,3]. In Saudi Arabia, road injuries are ranked the third leading cause of death causing 36 deaths per 100,000 population [4]. More recent statistics from the Saudi Ministry of Health (MOH) report a rising number of road traffic injuries, with 76 injuries per 100,000 population [5].
While there have been numerous studies assessing the broader spectrum of motor vehicle accidents in Saudi Arabia, motorcycle accidents have received relatively less attention in comparison [[6], [7], [8], [9], [10]]. Motorcyclists face a significantly higher risk of fatality and injury compared to occupants of passenger cars in the event of a crash. Previous studies have found that motorcyclists are around 8 times more likely to sustain injuries and 35 times more likely to cause death when involved in a collision [11]. This focus is critical because motorcyclists face a disproportionate risk of harm. These injuries are also associated with a high economic burden due to the need for surgical care, intensive care, and long-term rehabilitation [3]. Regarding fatalities of motorcycle accidents, there has been a 2 % increase in 2023 compared to 2022 in the US [12]. Locally there are no statistics that describe motorcycle accident trends in recent years.
Motorcycles have become an increasingly popular mode of transportation in Saudi Arabia because they offer a convenient and maneuverable option for navigating congested roads. Particularly, online food ordering applications have increased in popularity in the post-COVID period, and these applications employ motorcycle riders to deliver. However, this growth in motorcycle usage has also been accompanied by a concerning rise in the number of motorcycle-related accidents and fatalities. Therefore, we aim to assess the rate, injury pattern, and outcomes of motorcycle accidents to provide insights that can inform policies and interventions aimed at reducing the burden of motorcycle-related accidents.
Methods
The study was conducted at King Abdulaziz Medical City, Riyadh. KAMC is a level 1 trauma center with 24/7 availability of specialized care. The center is equipped to handle all types of traumatic injuries, including complex cases such as multiple traumas, severe head injuries, and spinal cord injuries. The center is also home to a trauma registry, which is a comprehensive database capturing all patients admitted following traumatic events, including motorcycle accidents. The study was conducted at a single trauma center, which may limit generalizability to other regions.
The study included all adult patients admitted following a motorcycle accident from January 2016 to December 2024. On the other hand, patients with minor injuries not necessitating hospital admission were excluded. Additionally, patients admitted for non-trauma related reasons, out of hospital deaths or transferred from other hospitals were also excluded.
The study was approved by the institutional review board (IRB) at KAIMRC protocol no. NRR24/080/7 as a retrospective review, informed consent was not required. All patient data were anonymized to maintain confidentiality and privacy in accordance with ethical standards.
Demographic data, including age, sex, nationality, and body mass index (BMI), were collected for each patient. The primary measures of interest included injury type and severity, need for surgical intervention, intensive care unit (ICU) admission, intubation, or prolonged hospital stay, mortality rate, long-term disability and rehabilitation needs, the use of safety measures (e.g., helmets, protective gear), and injury locations and specific body areas affected (head, limbs, chest, abdomen, etc.).
Injury types were categorized based on documentation in the trauma registry, which is derived from clinical notes and documented by trained registry staff. Data on helmet use were also extracted from trauma registry entries, which rely on documentation by emergency department physicians.
All statistical analyses were performed using RStudio (version 2024.9.1.394, Boston, MA, USA, using R version 4.4.2). Categorical variables were analyzed using Fisher's exact test or Pearson's chi-squared test as appropriate. Binary logistic regression models were constructed to examine factors associated with specific outcomes related to motorcycle accidents. Variables with a p-value of less than 0.05 in the univariate analyses were included in the multivariable logistic regression models to adjust for potential confounders. A p-value of <0.05 was considered statistically significant.
Missing data for BMI (1 %, 4 records) were excluded from subgroup analyses. For safety measures, where 91.1 % of cases were undocumented (Unknown), these cases were reported descriptively as a separate category, but excluded from multivariable regression.
Results
Demographic characteristics and incidence over time
The current study included data of 415 patients. The majority of patients were male (84.1 %), and the most common age groups were 25 to 35 years (38.6 %) and 18 to 25 years (36.6 %). Regarding BMI, 37.5 % had a healthy BMI, followed by 29.9 % who were overweight and 25.5 % who were obese. Saudi nationals accounted for 68.9 % of the cases, while non-Saudis comprised 31.1 % (Table 1).Table 1. Demographic characteristics and the statistical differences in the incidence of motorcycle accidents over time.Table 1. CharacteristicOverallN = 4152016N = 412017N = 412018N = 552019N = 542020N = 362021N = 382022N = 482023N = 622024N = 40p-ValueAge0.247 18 to <25152 (36.6 %)20 (48.8 %)18 (43.9 %)25 (45.5 %)23 (42.6 %)14 (38.9 %)8 (21.1 %)14 (29.2 %)18 (29.0 %)12 (30.0 %) 25 to <35160 (38.6 %)15 (36.6 %)12 (29.3 %)18 (32.7 %)19 (35.2 %)15 (41.7 %)18 (47.4 %)19 (39.6 %)26 (41.9 %)18 (45.0 %) 35 to <4569 (16.6 %)4 (9.8 %)6 (14.6 %)6 (10.9 %)10 (18.5 %)5 (13.9 %)4 (10.5 %)12 (25.0 %)13 (21.0 %)9 (22.5 %) 45 to <5526 (6.3 %)1 (2.4 %)5 (12.2 %)5 (9.1 %)1 (1.9 %)1 (2.8 %)5 (13.2 %)3 (6.3 %)4 (6.5 %)1 (2.5 %) 55 to <658 (1.9 %)1 (2.4 %)0 (0.0 %)1 (1.8 %)1 (1.9 %)1 (2.8 %)3 (7.9 %)0 (0.0 %)1 (1.6 %)0 (0.0 %)Gender0.038 Male349 (84.1 %)32 (78.0 %)38 (92.7 %)51 (92.7 %)39 (72.2 %)27 (75.0 %)33 (86.8 %)39 (81.3 %)54 (87.1 %)36 (90.0 %) Female66 (15.9 %)9 (22.0 %)3 (7.3 %)4 (7.3 %)15 (27.8 %)9 (25.0 %)5 (13.2 %)9 (18.8 %)8 (12.9 %)4 (10.0 %)BMIa0.748 Underweight29 (7.1 %)2 (5.1 %)3 (7.3 %)1 (1.9 %)3 (5.6 %)2 (5.6 %)3 (7.9 %)6 (12.5 %)6 (9.7 %)3 (7.5 %) Healthy154 (37.5 %)12 (30.8 %)15 (36.6 %)23 (43.4 %)26 (48.1 %)14 (38.9 %)9 (23.7 %)18 (37.5 %)20 (32.3 %)17 (42.5 %) Overweight123 (29.9 %)12 (30.8 %)14 (34.1 %)19 (35.8 %)11 (20.4 %)11 (30.6 %)11 (28.9 %)13 (27.1 %)22 (35.5 %)10 (25.0 %) Obese105 (25.5 %)13 (33.3 %)9 (22.0 %)10 (18.9 %)14 (25.9 %)9 (25.0 %)15 (39.5 %)11 (22.9 %)14 (22.6 %)10 (25.0 %)Nationality0.239 Saudi286 (68.9 %)28 (68.3 %)32 (78.0 %)41 (74.5 %)42 (77.8 %)26 (72.2 %)26 (68.4 %)29 (60.4 %)40 (64.5 %)22 (55.0 %) Non-Saudi129 (31.1 %)13 (31.7 %)9 (22.0 %)14 (25.5 %)12 (22.2 %)10 (27.8 %)12 (31.6 %)19 (39.6 %)22 (35.5 %)18 (45.0 %)n (%).Fisher's exact test; Pearson's Chi-squared test.aBMI values had 4 missing records.
The number of motorcycle accidents remained stable in 2016 and 2017 (n = 41 each year), followed by a slight increase in 2018 and 2019 (n = 55 and 54, respectively). A noticeable decline occurred in 2020, with the lowest number of accidents reported during the study period (n = 36). Subsequently, the frequency increased gradually, reaching 48 in 2022 and peaking at 62 in 2023, before decreasing again to 40 in 2024. Despite these fluctuations, the Mann-Kendall test indicated no statistically significant trend in accident incidence over the study period (p = 0.529, Fig. 1). The peak in 2023 may reflect contextual factors such as the expansion of motorcycle-based delivery services in Riyadh. Though specific data to confirm this was unavailable.Fig. 1. The frequencies of motorcycle accidents over time.Fig. 1
Regarding the statistical differences, only gender showed a statistically significant difference in the incidence of motorcycle accidents over time (p = 0.038). Males consistently accounted for the majority of cases each year, ranging from 72.2 % in 2019 to 92.7 % in 2017 and 2018 (Table 1).
Characteristics of injuries and outcomes
Most accidents occurred on streets or roads (90.8 %), with unknown activities reported in 93.7 % of cases. The use of safety measures was reported in only 2.7 % of cases, while 6.3 % had no safety measures. The most common injury types were fractures (86.7 %), brain injuries/bleeding (37.6 %), and cut/open wounds (27.5 %). Regarding outcomes, 64.8 % of patients did not require ICU admission, and 70.8 % did not undergo intubation. However, 69.9 % required surgical intervention, and hospital stays were typically less than one month (88.0 %). Long-term disability, which was defined according to discharge disposition and recorded rehabilitation requirements, was reported in 28.2 % of cases, and mortality occurred in 4.4 % (Table 2).Table 2. Characteristics of injuries and outcomes of patients.Table 2. CharacteristicDescriptionActivity at time of injury Leisure22 (5.3 %) Work2 (0.5 %) Unknown389 (93.7 %) Others2 (0.5 %)Where did the injury occur Street/road377 (90.8 %) Chalet/resort/camping35 (8.4 %) Others3 (0.7 %)Presence of safety measures No26 (6.3 %) Yes11 (2.7 %) Unknown378 (91.1 %)Multiple injuries182 (43.9 %)GCS 0 to 333 (8.0 %) 4 to 715 (3.6 %) 8 to 941 (9.9 %) 10 to 1224 (5.8 %) 12 to 15302 (72.8 %)ICU length of stay (weeks) None269 (64.8 %) <294 (22.7 %) 2 to 438 (9.2 %) 4 to 611 (2.7 %) 6 to 83 (0.7 %)Intubation period (weeks) None294 (70.8 %) <299 (23.9 %) 2 to 422 (5.3 %)Need for surgical intervention No124 (29.9 %) Yes290 (69.9 %) Unknown1 (0.2 %)Hospital length of stay (months) <1365 (88.0 %) 1 to 332 (7.7 %) 3 to 610 (2.4 %) 6 to 93 (0.7 %) 9 to 123 (0.7 %) >122 (0.5 %)Hospital disposition and projected effect of injurya No significant disability139 (33.8 %) Short-term disability113 (27.5 %) Long-term disability116 (28.2 %) Permanent disability25 (6.1 %) Death18 (4.4 %)n (%).GCS = Glascow Coma Scale.ICU = intensive care unit.aThe variable had 4 missing records.
Fig. 2 illustrates the distribution of injury types among patients involved in motorcycle accidents. Fractures were the most common injury, affecting 86.7 % of patients, followed by brain injuries or bleeding (38.1 %) and cut/open wounds (27.2 %). Regarding injury sites, injuries to the head and upper limbs were the most prevalent, affecting 42.9 % and 40.2 % of patients, respectively, followed by lower limb injuries (29.4 %) and chest injuries (23.4 %, Fig. 3).Fig. 2. Types of injuries after motorcycle accidents.Fig. 2. Fig. 3Sites of injuries after motorcycle accidents.Fig. 3
Factors associated with surgical intervention
The likelihood of undergoing a surgical intervention was significantly increased with specific injury types, including cut/open wounds (p = 0.005), lower limb injuries (p < 0.001), and upper limb injuries (p < 0.001) (Table 3).Table 3. Factors associated with the need for surgical interventions.Table 3. CharacteristicInferential analysisMultivariable regressionNoN = 125YesN = 290p-ValueOR95 % CIp-ValueAge0.756 18 to <2544 (28.9 %)108 (71.1 %) 25 to <3550 (31.3 %)110 (68.8 %) 35 to <4520 (29.0 %)49 (71.0 %) 45 to <557 (26.9 %)19 (73.1 %) 55 to <654 (50.0 %)4 (50.0 %)Sex0.797 Male106 (30.4 %)243 (69.6 %) Female19 (28.8 %)47 (71.2 %)Presence of safety measures0.177 No11 (42.3 %)15 (57.7 %) Yes5 (45.5 %)6 (54.5 %) Unknown109 (28.8 %)269 (71.2 %)Type of injury Brain injury bleeding68 (43.6 %)88 (56.4 %)<0.0012.090.80, 5.760.140 Bruise superficial31 (30.1 %)72 (69.9 %)0.995 Fracture92 (25.6 %)268 (74.4 %)<0.0011.590.78, 3.260.200 Visceral injury30 (40.0 %)45 (60.0 %)0.0390.970.48, 1.970.924 Organ or system injury28 (47.5 %)31 (52.5 %)0.0020.760.35, 1.610.466 Open wound25 (21.9 %)89 (78.1 %)0.0252.511.34, 4.890.005 Concussion5 (55.6 %)4 (44.4 %)0.136 Burn2 (12.5 %)14 (87.5 %)0.165 Sprain1 (12.5 %)7 (87.5 %)0.445 Others3 (50.0 %)3 (50.0 %)0.371n (%).Fisher's exact test; Pearson's Chi-squared test.OR = odds ratio, CI = confidence interval.The multivariable regression model was based on binomial logistic regression analysis, which included the significantly associated variables from the inferential analysis as independent variables.
Factors associated with ICU admission
ICU admission was associated with sex, with females less likely to require ICU care than males (p = 0.048). Brain injuries/bleeding were significant risk factors for ICU admission (p = 0.007). Having injuries in specific sites was significantly associated with an increased odds of ICU admission, including head injuries (p < 0.001), chest injuries (p = 0.012) and whole-body injuries (p < 0.001, Table 4).Table 4. Factors associated with ICU admission.Table 4. CharacteristicInferential analysisMultivariable regressionNoN = 269YesN = 146p-ValueOR95 % CIp-ValueAge0.791 18 to <2594 (61.8 %)58 (38.2 %) 25 to <35106 (66.3 %)54 (33.8 %) 35 to <4544 (63.8 %)25 (36.2 %) 45 to <5519 (73.1 %)7 (26.9 %) 55 to <656 (75.0 %)2 (25.0 %)Sex<0.001 Male211 (60.5 %)138 (39.5 %)ReferenceReference Female58 (87.9 %)8 (12.1 %)0.360.12, 0.970.048Type of injury Brain injury bleeding40 (25.6 %)116 (74.4 %)<0.0013.741.45, 10.00.007 Bruise superficial68 (66.0 %)35 (34.0 %)0.769 Fracture237 (65.8 %)123 (34.2 %)0.268 Visceral injury23 (30.7 %)52 (69.3 %)<0.0012.460.99, 6.240.054 Organ or system injury18 (30.5 %)41 (69.5 %)<0.0012.150.80, 6.050.138 Cut open wound55 (48.2 %)59 (51.8 %)<0.0011.640.76, 3.560.207 Concussion3 (33.3 %)6 (66.7 %)0.072 Burn9 (56.3 %)7 (43.8 %)0.464 Others6 (100.0 %)0 (0.0 %)0.095 Sprain7 (87.5 %)1 (12.5 %)0.270Site of injury Abdomen14 (28.6 %)35 (71.4 %)<0.0011.570.46, 5.500.473 Back14 (38.9 %)22 (61.1 %)<0.0011.140.33, 4.230.835 Head47 (28.5 %)118 (71.5 %)<0.0019.843.34, 29.9<0.001 Chest28 (30.4 %)64 (69.6 %)<0.0013.081.30, 7.590.012 Lower limbs76 (63.9 %)43 (36.1 %)0.796 Face12 (21.1 %)45 (78.9 %)<0.0012.851.17, 7.330.024 Others14 (42.4 %)19 (57.6 %)0.0051.810.61, 5.510.289 Upper limb131 (79.4 %)34 (20.6 %)<0.0010.550.24, 1.220.144 Multiple whole body23 (51.1 %)22 (48.9 %)0.0416.522.18, 20.5<0.001 Eyes0 (0.0 %)1 (100.0 %)0.352n (%).Fisher's exact test; Pearson's Chi-squared test.OR = odds ratio, CI = confidence interval.The multivariable regression model was based on binomial logistic regression analysis, which included the significantly associated variables from the inferential analysis as independent variables.
Factors associated with intubation
Table 5 presents factors associated with intubation among patients involved in motorcycle accidents. Brain injuries/bleeding (p = 0.020) and head injuries (p < 0.001) were significantly associated with higher odds of intubation. Additionally, injuries to the face (p = 0.003) and other sites (p = 0.020) were also significantly linked to intubation.Table 5. Factors associated with intubation.Table 5. CharacteristicInferential analysisMultivariable regressionNoN = 294YesN = 121p-ValueOR95 % CI^3^p-ValueAge0.950 18 to <25109 (71.7 %)43 (28.3 %) 25 to <35114 (71.3 %)46 (28.8 %) 35 to <4546 (66.7 %)23 (33.3 %) 45 to <5519 (73.1 %)7 (26.9 %) 55 to <656 (75.0 %)2 (25.0 %)Gender<0.001 Male232 (66.5 %)117 (33.5 %)ReferenceReference Female62 (93.9 %)4 (6.1 %)0.170.04, 0.530.004Type of injury Brain injury bleeding56 (35.9 %)100 (64.1 %)<0.0013.011.18, 7.730.020 Bruise superficial69 (67.0 %)34 (33.0 %)0.321 Fracture257 (71.4 %)103 (28.6 %)0.532 Visceral injury33 (44.0 %)42 (56.0 %)<0.0011.530.63, 3.710.347 Organ or system injury26 (44.1 %)33 (55.9 %)<0.0011.240.52, 3.040.628 Cut open wound64 (56.1 %)50 (43.9 %)<0.0011.870.89, 3.940.097 Concussion4 (44.4 %)5 (55.6 %)0.130 Burn13 (81.3 %)3 (18.8 %)0.416 Others5 (83.3 %)1 (16.7 %)0.676Site of injury Abdomen19 (38.8 %)30 (61.2 %)<0.0012.190.73, 6.910.168 Back19 (52.8 %)17 (47.2 %)0.0130.550.18, 1.670.292 Head62 (37.6 %)103 (62.4 %)<0.0017.152.66, 19.8<0.001 Chest40 (43.5 %)52 (56.5 %)<0.0011.710.75, 3.930.203 Lower limbs83 (69.7 %)36 (30.3 %)0.756 Face16 (28.1 %)41 (71.9 %)<0.0013.591.58, 8.530.003 Others14 (42.4 %)19 (57.6 %)<0.0013.651.24, 11.10.020 Upper limb138 (83.6 %)27 (16.4 %)<0.0010.520.23, 1.120.099 Multiple whole body29 (64.4 %)16 (35.6 %)0.317 Eyes0 (0.0 %)1 (100.0 %)0.292n (%).Fisher's exact test; Pearson's Chi-squared test.OR = odds ratio, CI = confidence interval.The multivariable regression model was based on binomial logistic regression analysis, which included the significantly associated variables from the inferential analysis as independent variables.
Discussion
This nine-year retrospective review demonstrates the significant burden of motorcycle-related injuries in Saudi Arabia, with severe consequences including long-term disability and death. As our study showed fractures were the most prevalent injury affecting 86.7 % of patients, reflecting the high-impact nature of motorcycle crashes and the absence of protective barriers compared to enclosed vehicles. Brain injuries or bleeding were the second most common injuries, affecting 38.1 % of patients, which is concerning given the high mortality and long-term disability associated with such injuries. Cut and open wounds were seen in 27.2 % of patients, reflecting the severity of road crash and external injuries are common in motorcycle accidents. The head and upper limbs were the most commonly injured sites, with significant associations between these injuries and the need for ICU care or surgery. Head injuries were particularly associated with severe outcomes, including ICU admission, intubation, and surgical intervention.
The majority of the patients were male (84.1 %), with the highest incidence observed in the age groups 18–25 and 25–35 years, likely due to the increased use of motorcycles in these age groups. The study also notes an increase in motorcycle accidents, peaking in 2023, although no statistically significant trend over time was found. The significant decrease in accidents in 2020 (n = 36) can likely be attributed to the direct effects of the COVID-19 pandemic, which resulted in lockdowns, curfews, and restrictions on travel, leading to fewer motorcycles on the road.
Our study's main findings on the impact of motorcycle accidents are consistent with many other publications. Various studies [11,13,14] reported similar age and gender proportions, with the average age ranging from 21 to 32 and a constant predominant male proportion of 85 % to 86 % across these studies. In our trauma center, Suliman Alghnam et al [11] reported similar demographic results with male predominance of 85 % with the great majority of patients being younger than 40 years old and clustered around the 20s range. It is very important to note that these were pre-COVID-19 findings, pointing out that the pandemic did not influence the main demographic trends seen across studies.
Our data also revealed that more than half of riders were overweight or obese. While current evidence suggests BMI is not directly associated with mortality or hospital length of stay [15], biomechanics may differ, greater body mass increases kinetic energy transfer during crashes, potentially predisposing to specific fracture patterns or higher injury severity. Future studies could explore how body composition influences injury mechanisms in motorcycle accidents.
The presence of safety measures was only reported in 9 % of the patients in our study, which means that documentation is still an issue being faced in our center, as also reported by Suliman Alghnam et al [11] in his study in 2019. This poor documentation likely stems from factors such as inconsistent reporting by emergency department physicians. Furthermore, the absence of mandatory fields for safety measures in the KAMC trauma registry likely exacerbates this issue. Wearing a helmet and following safety protocols while riding a motorcycle are mandatory traffic regulations in Saudi Arabia. Therefore, we would expect a high level of compliance with these regulations among most patients, which may contribute to a predominance of mild to moderate injuries, as observed across various variables in Table 3. This is consistent with findings from other studies that have linked the severity of injuries to the use of safety measures [19].
Extremity injuries (69.6 %) were the most common site of injury in our study, followed by head (42.2 %) and chest injuries (23.4 %), which is a trend observed and expected with some variation in almost all motorcycle accidents studies [11,[13], [14], [15], [16], [17]]. Surgical interventions mostly were needed for orthopedic injuries which may include open fractures and open wound injuries. Fletcher et al published a study that focused on predictors of hospitalization and surgical intervention, and most patients that required either or both were orthopedic patients [18]. ICU admission and intubation, on the other hand, was observed more in the head injury spectrum compared to fractures or extremity injuries, which, for the latter, is not usually severe to require ICU admission. This pattern was also noticed in other studies that assessed the severity of head injuries in motorcycle accidents [20].
Given the high incidence of fractures and brain injuries observed in this study, enhanced protective measures such as stricter helmet enforcement and safety training programs could significantly reduce morbidity and mortality. Studies have shown that helmet use can reduce the risk of severe head injuries by 69 % and decrease the likelihood of fatal outcomes by 42 % [21].
Moreover, the substantial proportion of patients requiring surgical intervention (69.9 %) increases the burden on healthcare resources, emphasizing the necessity of optimizing trauma care infrastructure, including orthopedic and neurosurgical services. A study in the United States found that motorcycle-related injuries accounted for 15 % of all trauma-related surgeries in major trauma centers, placing a significant strain on surgical and rehabilitation services [22].
Despite its valuable insights, this study has several limitations. First, as a retrospective analysis, it is subject to documentation bias, particularly concerning helmet use and other safety measures, which were reported in only 9 % of cases. Studies have shown that underreporting of helmet use is common in trauma registries, leading to an inaccurate assessment of safety compliance [23].
Second, the study is limited to a single Level 1 trauma center, which may not fully represent the broader national motorcycle accident trends in Saudi Arabia. Different regions may have varying accident rates, injury patterns, and hospital capacities, affecting generalizability. Additionally, out-of-hospital deaths and cases managed in non-trauma centers were excluded, potentially leading to an underestimation of fatality rates. A study in Southeast Asia found that up to 35 % of motorcycle-related fatalities occur before hospital arrival, suggesting that the true burden of mortality may be higher than reported [24].
Another limitation is the lack of information on other risk factors, such as alcohol or drug use, road conditions, and the involvement of other vehicles in crashes. These factors have been identified in previous research as significant contributors to motorcycle accidents, yet they were not documented in our study [25]. Finally, while the study establishes associations between injury patterns and outcomes, causality cannot be inferred due to the observational nature of the research.
The high rate of surgical intervention emphasizes the need for strong orthopedic and neurosurgical capacity in trauma centers. Prehospital systems also play a crucial role: rapid triage and early recognition of head, chest, and spinal trauma could improve outcomes. With 28.2 % of patients experiencing long-term disability.
Future studies should address the identified limitations to improve the understanding of motorcycle accidents in Saudi Arabia. A nationwide, multi-center study incorporating data from various hospitals and emergency services would provide a more comprehensive overview of motorcycle accident trends and outcomes.
Research on the effectiveness of safety interventions, such as mandatory helmet laws, speed regulations, and motorcycle lane implementations, would be beneficial. Studies have indicated that countries with stricter helmet enforcement and designated motorcycle lanes report lower injury and fatality rates among motorcyclists [26]. Also, we could benefit from public health interventions including school-based safety education, media campaigns, and enhanced enforcement of helmet laws.
Finally, studies analyzing the long-term functional and economic impact of motorcycle injuries would be valuable in assessing the burden on individuals, families, and healthcare systems. Research has shown that long-term disabilities following motorcycle accidents can significantly reduce quality of life and impose financial strain on healthcare systems [27].
By addressing these gaps, future research can contribute to more effective interventions, ultimately reducing motorcycle accident-related morbidity and mortality in Saudi Arabia.
Conclusion
Motorcycle accidents continue to pose a public health challenge in Saudi Arabia, with young male motorcyclists being the most vulnerable group. The high incidence of fractures and brain injuries emphasizes the importance of improving safety measures to reduce the severity of injuries. Surgical interventions and ICU admissions highlight the substantial healthcare burden, suggesting the need for optimized trauma care systems and targeted preventive measures for high-risk populations such as delivery riders.
CRediT authorship contribution statement
Hussam Alhathlol: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Khalid Alsikhan: Writing – review & editing, Writing – original draft, Visualization, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Turki Alharbi: Writing – review & editing, Writing – original draft, Visualization, Methodology, Investigation, Data curation, Conceptualization. Ibrahim Alsamaani: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Methodology, Investigation. Ali Alhathloul: Writing – review & editing, Visualization, Validation, Supervision, Investigation, Data curation, Conceptualization. Rifan Alyami: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Methodology, Data curation, Conceptualization.
Ethics approval
Ethical approval for this study was obtained from KAIMRC protocol no. NRR24/080/7.
Funding sources
The authors received no funding for this publication.
Declaration of competing interest
The authors declare no conflict of interest related to this study. The research was conducted independently, with no financial support from external sources or competing interests influencing the outcomes of the study. All authors contributed equally to the design, data collection, analysis, and writing of the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1James S.L.Lucchesi L.R.Bisignano C.Morbidity and mortality from road injuries: results from the Global Burden of Disease Study 2017 Inj Prev 26Supp 12020 i 46i 5610.1136/injuryprev-2019-04330231915274 PMC 7571357 · doi ↗ · pubmed ↗
- 2World Health Organization Road traffic injuries Available at:https://www.who.int/news-room/fact-sheets/detail/road-traffic-injuries
- 3Alghnam S.Alkelya M.Aldahnim M.Healthcare costs of road injuries in Saudi Arabia: a quantile regression analysis Accid Anal Prev 159202110626610.1016/j.aap.2021.10626634225170 · doi ↗ · pubmed ↗
- 4World Health Organization Leading causes of death in Saudi Arabia Available at:https://data.who.int/countries/682
- 5Saudi Ministry of Health Statistical yearbook 2022 Available at:https://www.moh.gov.sa/en/Ministry/Statistics/book/Documents/Statistical-Yearbook-2022.pdf
- 6Alenezi E.Z.Al Qahtani A.M.Althunayan S.F.Prevalence and determinants of road traffic accidents in Saudi Arabia: a systematic review Cureus 1512 Dec 27 2023 e 5120510.7759/cureus.51205 PMC 1081812938283470 · doi ↗ · pubmed ↗
- 7Mansuri F.A.Al-Zalabani A.H.Zalat M.M.Qabshawi R.I.Road safety and road traffic accidents in Saudi Arabia. A systematic review of existing evidence Saudi Med J 364201541842410.15537/smj.2015.4.1000325828277 PMC 4404474 · doi ↗ · pubmed ↗
- 8Shanks N.J.Ansari M.al-Kalai D.Road traffic accidents in Saudi Arabia Public Health 10811994273410.1016/s 0033-3506(05)80032-08202582 · doi ↗ · pubmed ↗