Exceptional Response to Pembrolizumab in Metastatic ER+/HER2− Breast Cancer With Liver Metastases: A Case Report and Literature Review
Claudia Villa Celi, Supriya Peshin, Adit Dharia, Faizan Bashir, Linden Erica

TL;DR
A patient with hormone receptor-positive breast cancer showed a strong response to pembrolizumab after developing high PD-L1 expression in liver metastases.
Contribution
Demonstrates exceptional response to immunotherapy in a typically resistant breast cancer subtype with high PD-L1 expression.
Findings
The patient achieved near-complete remission with pembrolizumab after progressing on other therapies.
High PD-L1 expression (CPS 95%) was observed in liver metastases, which correlated with treatment response.
The remission lasted about 10 months before disease progression.
Abstract
Hormone receptor–positive (HR+) and HER2-negative breast cancer is the most common subtype in women, particularly in the postmenopausal setting. Unlike triple-negative breast cancer, the benefit of immune checkpoint inhibitors (ICIs) in HR+/HER2− disease remains uncertain because of low tumor immunogenicity and limited PD-L1 expression. We describe a case of a 70-year-old woman who presented with severe anemia and was incidentally found to have a bleeding left breast mass. Biopsy confirmed Grade 3 invasive ductal carcinoma (ER+/PR+ > 95%, HER2−) with nodal involvement but no distant metastases, consistent with Stage IIIc disease. She was treated with neoadjuvant anastrozole, modified radical mastectomy, adjuvant chemotherapy, radiation, and continued endocrine therapy. After 3 years, she developed extensive hepatic metastases. Biopsy revealed ER+/PR−/HER2− disease with striking PD-L1…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
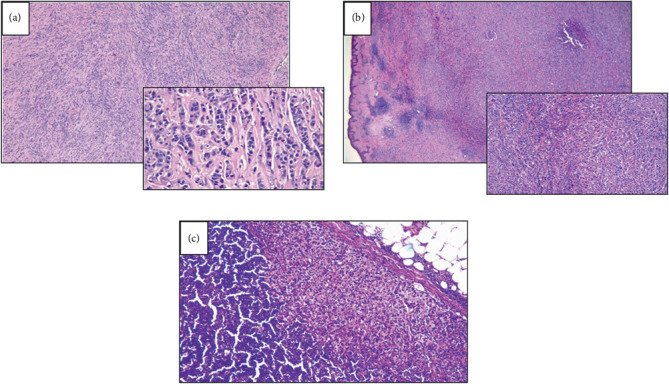 Figure 1
Figure 1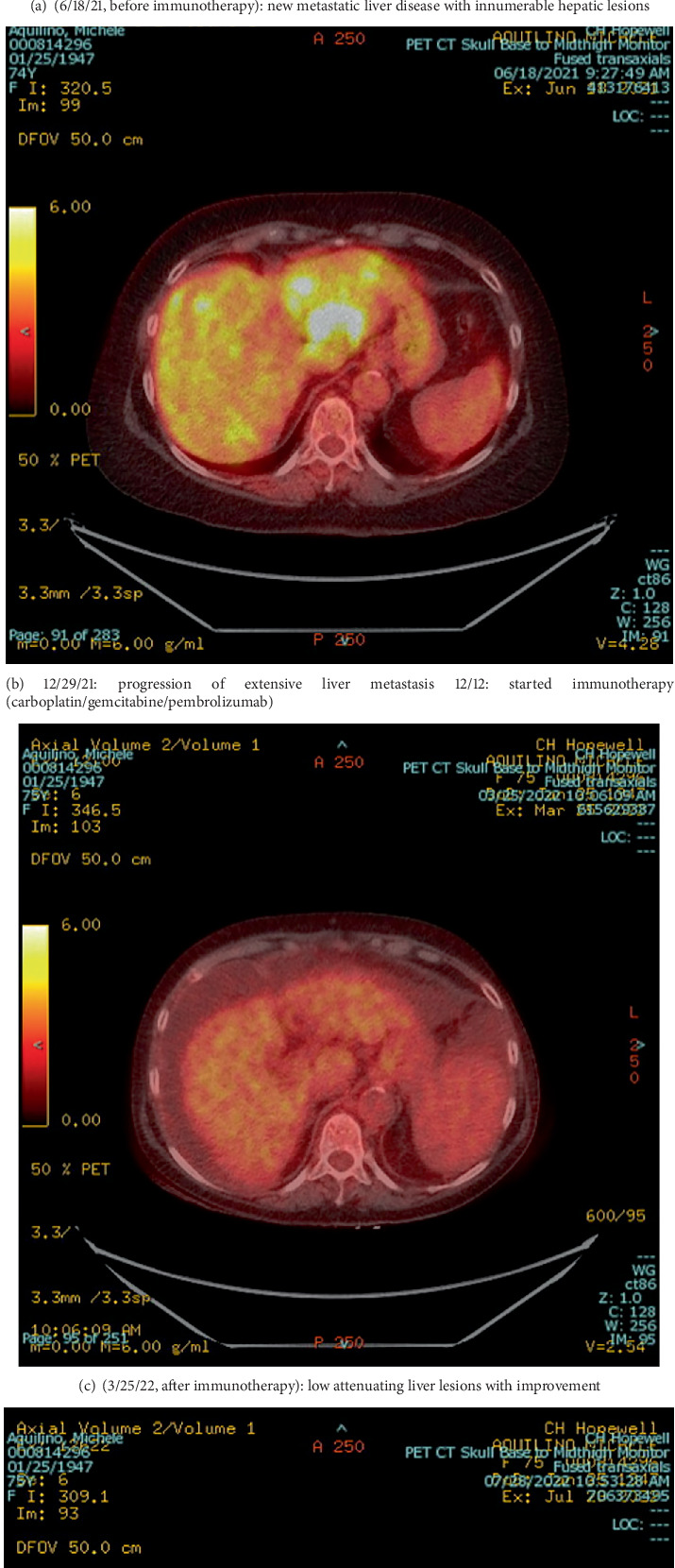 Figure 2
Figure 2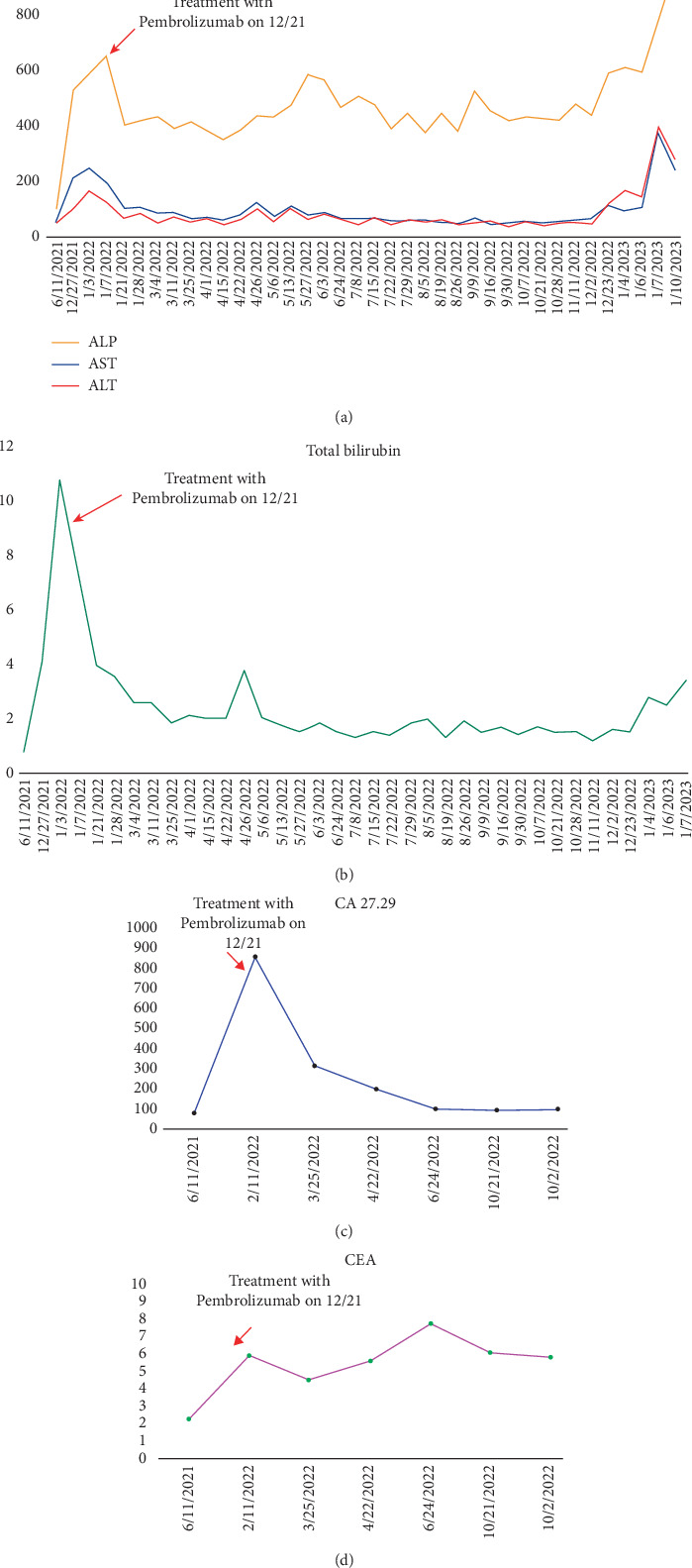 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Advanced Breast Cancer Therapies · Brain Metastases and Treatment
Summary
- • Immune checkpoint inhibitors (ICIs) may have a role in hormone receptor–positive (HR+) and human epidermal growth factor receptor 2-negative (HER2−) metastatic breast cancer with high programmed death-ligand 1 (PD-L1) expression.
- • The exceptional response to pembrolizumab underscores the need for future research into immunotherapy-driven approaches, potentially expanding treatment options beyond conventional endocrine and chemotherapy regimens.
1. Background
Breast cancer is the most frequently diagnosed cancer among women in the United States and North America, representing a significant public health burden [1, 2]. HR+ and HER2− breast cancers are the most common subtypes, accounting for approximately 60%–70% of all cases [3, 4]. Despite advancements in treatment, metastatic HR+/HER2− breast cancer remains challenging, with endocrine resistance often limiting long-term survival [5]. Current standard therapies, including endocrine therapy and cyclin-dependent kinase 4/6 (CDK4/6) inhibitors, have improved outcomes; however, the challenge of inevitable progression in advanced disease remains [6].
ICIs, which enhance the immune system's ability to detect and destroy cancer cells, have revolutionized the treatment of various malignancies [7]. However, their efficacy in HR+/HER2− breast cancer has been less pronounced compared to other subtypes, such as triple-negative breast cancer (TNBC) [8]. Lower PD-L1 expression and reduced immune infiltration in HR+ tumors are thought to contribute to this limited response [9]. Emerging evidence suggests that select HR+/HER2− breast cancer cases, particularly those with high tumor PD-L1 expression or significant tumor burden, may benefit from ICIs [10–12].
This report highlights the case of a 70-year-old woman with metastatic HR+/HER2− breast cancer and extensive liver metastases who demonstrated a remarkable response to pembrolizumab-based therapy. By exploring this case and reviewing relevant clinical trials, including the PACE trial and KEYNOTE-756 [13, 14], we aim to emphasize the potential role of ICIs in HR+ breast cancer and discuss future directions for integrating immunotherapy in this challenging disease subtype.
2. Case Presentation
A 70-year-old woman presented with severe anemia, with her hemoglobin level measuring 5.6 g/dL. She was initially evaluated for suspected peptic ulcer disease; however, during this work-up, an incidental finding of a large, ulcerated, and actively bleeding mass was noted in the left breast, specifically in the lower outer quadrant.
A core needle biopsy of the breast lesion revealed invasive ductal carcinoma (IDC), Grade 3. Immunohistochemistry showed strong expression of estrogen and progesterone receptors (> 95% positivity) and was negative for HER2. A biopsy of a regional lymph node confirmed metastatic involvement. Staging studies demonstrated no evidence of distant metastases, leading to a clinical diagnosis of Stage IIIc breast cancer (cT4a cN1).
The patient was started on anastrozole, which resulted in marked clinical improvement and near-complete resolution of the breast mass. Given this favorable response, she underwent a left modified radical mastectomy (MRM). Histopathological examination confirmed residual Grade 3 IDC with extensive lymphovascular invasion and involvement of one out of six lymph nodes (ypT2 ypN1) (Figure 1). Repeat staging with laboratory studies and PET imaging revealed no distant disease.
Postoperatively, she received dose-dense adriamycin and cyclophosphamide, followed by paclitaxel (ddAC-Taxol), in addition to comprehensive radiation therapy. She subsequently resumed endocrine therapy with anastrozole.
Three years later, at the age of 73, she developed biochemical evidence of disease recurrence, with a CA 27.29 level of 75.2 U/mL. PET imaging revealed multiple hepatic lesions, and a biopsy confirmed metastatic breast carcinoma (ER+, PR−, HER2− by IHC, and GATA3 positive). Next-generation sequencing (Foundation One) identified strikingly high PD-L1 expression (CPS 95%). This was an unusual finding in ER+/HER2− disease and suggested potential sensitivity to immunotherapy.
She was initially treated with fulvestrant and palbociclib, but her disease progressed, with worsening liver function tests and imaging findings. In view of her high PD-L1 expression, therapy was switched to carboplatin, gemcitabine, and pembrolizumab. Within 3 months, her liver function normalized, and imaging demonstrated a dramatic radiological response (Figures 2a, 2b, 2c, 2d, and 3).
The patient remained disease-free for approximately 10 months. Thereafter, she developed repeated hospitalizations due to infections and complications of pseudocirrhosis. Her disease subsequently progressed rapidly, and she transitioned to hospice care. She passed away shortly thereafter.
This case emphasizes the challenges of managing advanced breast cancer, while highlighting the potential benefit of immunotherapy in patients with exceptionally high PD-L1 expression, even in the ER+/HER2− subtype.
3. Discussion
TNBC is an aggressive and immunogenic subtype of breast cancer with a high propensity for metastasis and limited treatment options due to its lack of hormone receptors and HER2 amplification [9, 15]. Historically, chemotherapy has been the mainstay of treatment [2, 15, 16]. However, the advent of ICIs has significantly altered the therapeutic landscape, demonstrating survival benefits in appropriately selected patients [10, 11, 17–21]. This is probably because of the tumor's immunogenicity, a high proportion of tumor-infiltrating lymphocytes (TILs), tumor mutational burden, and PD-L1 expression [7, 9, 22–26]. In contrast, the role of immunotherapy in HR+ breast cancer remains under active investigation.
The first signal of activity for ICIs in HR+ breast cancer came from KEYNOTE-028, a Phase Ib multicohort basket study of pembrolizumab in PD-L1-positive advanced solid tumors. The HR+/HER2− breast cancer cohort included 25 heavily pretreated patients. While the objective response rate was modest at 12% (3 partial responses), the responses were durable with a median duration of response of ~12 months. Importantly, the trial confirmed that pembrolizumab was safe and tolerable in this population, providing early proof-of-concept that immune checkpoint inhibition can achieve disease control in select ER+ patients [27].
In the neoadjuvant setting, the I-SPY2 adaptive platform trial provided stronger evidence of benefit. This trial continuously evaluates novel agents in high-risk Stage II/III breast cancer using biomarker-driven adaptive randomization. In the ER+/HER2− high-risk cohort, the addition of pembrolizumab to standard chemotherapy nearly doubled pathologic complete response (pCR) rates to 30% compared with 13% for chemotherapy alone [28]. Although I-SPY2 is exploratory in nature, this result was important because it showed that immunotherapy could meaningfully enhance chemotherapy efficacy even in a traditionally immune-cold subtype, and it directly informed the design of Phase III trials such as KEYNOTE-756 [14].
The most definitive evidence to date comes from the CheckMate-7FL Phase III trial, which randomized 510 patients with early-stage, high-risk ER+/HER2− breast cancer to receive neoadjuvant chemotherapy with either nivolumab or placebo. The addition of nivolumab significantly improved pCR rates (24.5% vs. 13.8%, p = 0.0021), with the greatest benefit observed in PD-L1-positive tumors (44.3% vs. 20.2%). Safety was manageable, consistent with prior ICI experience, and while event-free survival data remain immature, the trial confirms that PD-1 blockade can potentiate chemotherapy response in this subtype [29].
In the metastatic setting, the PACE trial explored whether immunotherapy could overcome endocrine resistance after CDK4/6 inhibitor failure. Patients with HR+/HER2− metastatic breast cancer were randomized to fulvestrant alone, fulvestrant plus palbociclib, or fulvestrant plus palbociclib and the PD-L1 inhibitor avelumab [13]. While the trial did not meet its primary endpoint of improved progression-free survival, exploratory analysis revealed that the triplet arm achieved a longer median overall survival of 42.5 months compared with 27.5 months for fulvestrant alone and 24.6 months for fulvestrant plus palbociclib. These findings suggest that checkpoint blockade may synergize with endocrine and targeted therapy in a subset of patients, supporting continued investigation into rational combinations in advanced HR+ disease [30–32].
The most compelling data come from the KEYNOTE-756 trial, a randomized Phase III study enrolling 1278 patients with high-risk, Grade 3, early-stage ER+/HER2− breast cancer [14]. Patients were assigned to neoadjuvant chemotherapy with either pembrolizumab or placebo, followed by surgery, then adjuvant pembrolizumab or placebo plus endocrine therapy. Dual primary endpoints are pCR rate and EFS. The results revealed a significantly higher pCR in the pembrolizumab group compared to the control group (24.3% vs. 15.6%, p = 0.00005), reflecting an absolute improvement of 8.7%. These findings suggest that incorporating pembrolizumab may enhance the effectiveness of standard therapies. The study also assessed residual cancer burden (RCB) outcomes as a secondary endpoint, providing insights into the extent of residual disease posttreatment. Pembrolizumab was also associated with lower residual RCB scores, suggesting deeper responses. While EFS data remain immature, early trends favor pembrolizumab, suggesting that the addition of PD-1 blockade not only increases the chance of achieving pCR but may also translate into long-term survival benefit. Together with CheckMate-7FL, KEYNOTE-756 establishes proof-of-principle that immune checkpoint inhibition can improve outcomes in high-risk ER+/HER2− breast cancer (Table 1) [33–35].
Several published case reports mirror our patient's outcome and provide important clinical context. Wang et al. described an ER+/HER2−, TMB-high patient with a partial response to camrelizumab plus vinorelbine [36]. Wu et al. reported two ER+ cases who achieved progression-free survival beyond 21 months with pembrolizumab combined with letrozole or tamoxifen [37]. Li et al. documented an exceptional response to pembrolizumab and trastuzumab in a heavily pretreated HER2-positive patient with MSI-H and TMB-high disease [38]. Fitzpatrick and Cobleigh described a 72-year-old with lobular carcinoma and high TMB who achieved a complete response to pembrolizumab [39]. Kaplan et al. provided compelling evidence that the MLH1 1835del3 germline variant was pathogenic, with the affected patient experiencing a > 5-year remission after just four doses of pembrolizumab [40]. Collectively, these cases emphasize that rare, biomarker-defined subsets of ER+ breast cancer may achieve durable and exceptional responses to immunotherapy.
Our case adds to this growing body of evidence by demonstrating a dramatic response to pembrolizumab in HR+ metastatic breast cancer with extensive visceral involvement. Importantly, the patient's biomarker profile aligned with emerging predictors of ICI sensitivity, reinforcing the role of comprehensive molecular testing in treatment selection. This observation is consistent with recent reviews emphasizing that, although immunotherapy is not standard for HR+ breast cancer, biomarker-driven approaches and rational combinations may expand its therapeutic potential.
4. Conclusion
This case underlines the potential role of pembrolizumab in a select subgroup of HR+/HER2− metastatic breast cancer patients with high PD-L1 expression. The patient's durable response reinforces the need for further studies to refine predictive biomarkers and optimize immunotherapy strategies in this traditionally immunotherapy-resistant subtype. While ICIs have shown significant success in TNBC, their efficacy in HR+ breast cancer has been limited. However, emerging data suggest their potential benefit in specific subsets of patients. The PACE trial demonstrated a prolonged PFS with the addition of avelumab, and the KEYNOTE-756 trial reported a statistically significant improvement in pCR rates in the pembrolizumab arm. These findings highlight the promise of ICIs in HR+ breast tumors. Further research is essential to identify predictive biomarkers and develop personalized immunotherapy-based strategies for women with advanced breast cancer, especially those traditionally considered nonimmunogenic.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1American Cancer Society Breast Cancer Facts & Figures 2024 Cancer.org 2024 American Cancer Society https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-facts-and-figures/2024/breast-cancer-facts-and-figures-2024.pdf Accessed 4 Mar 2025
- 2Bleicher R. J. Timing and Delays in Breast Cancer Evaluation and Treatment Annals of Surgical Oncology 201825102829283810.1245/s 10434-018-6615-22-s 2.0-8504956983529968031 PMC 6123282 · doi ↗ · pubmed ↗
- 3National Cancer Institute Cancer Stat Facts: Female Breast Cancer Subtypes Available from: https://seer.cancer.gov/statfacts/html/breast-subtypes.html
- 4Fasching P. A. Kreipe H. Del Mastro L. Identification of Patients With Early HR+ HER 2- Breast Cancer at High Risk of Recurrence Geburtshilfe und Frauenheilkunde 202484216418410.1055/a-2238-319938344042 PMC 10853032 · doi ↗ · pubmed ↗
- 5Clarke R. Tyson J. J. Dixon J. M. Endocrine Resistance in Breast Cancer--An Overview and Update Molecular and Cellular Endocrinology 2015418322023410.1016/j.mce.2015.09.0352-s 2.0-8494956410626455641 PMC 4684757 · doi ↗ · pubmed ↗
- 6Ma J. Chan J. J. Toh C. H. Yap Y. S. Emerging Systemic Therapy Options Beyond CDK 4/6 Inhibitors for Hormone Receptor-Positive HER 2-Negative Advanced Breast Cancer npj Breast Cancer 202391 p. 7410.1038/s 41523-023-00578-337684290 PMC 10491615 · doi ↗ · pubmed ↗
- 7Núñez Abad M. Calabuig-Fariñas S. Lobo de Mena M. Programmed Death-Ligand 1 (PD-L 1) as Immunotherapy Biomarker in Breast Cancer Cancers 2022142 p. 30710.3390/cancers 1402030735053471 PMC 8773553 · doi ↗ · pubmed ↗
- 8Liu Y. Hu Y. Xue J. Advances in Immunotherapy for Triple-Negative Breast Cancer Molecular Cancer 2023221 p. 14510.1186/s 12943-023-01850-737660039 PMC 10474743 · doi ↗ · pubmed ↗