A newly designed duodenal stent enables stent placement for jejunal obstruction
Shota Harai, Susumu Hijioka, Yoshikuni Nagashio, Daiki Yamashige, Yutaka Saito, Takuji Okusaka

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
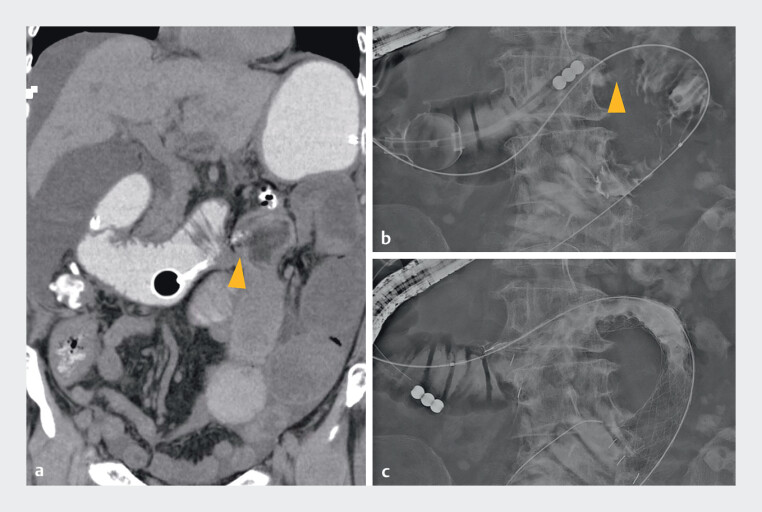 Fig. 1
Fig. 1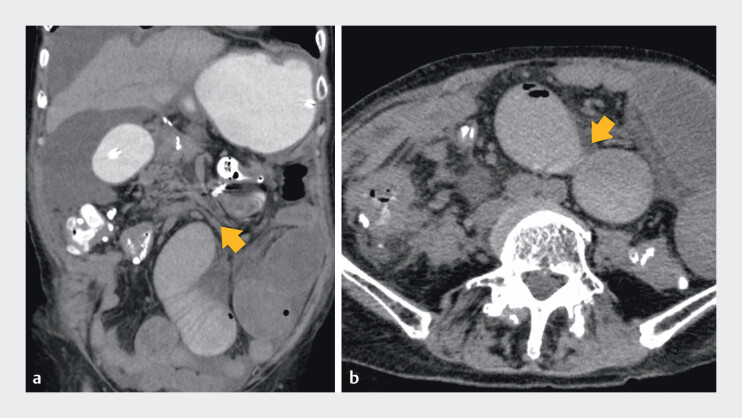 Fig. 2
Fig. 2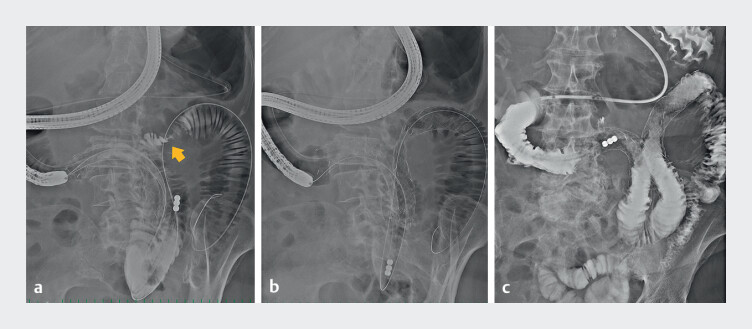 Fig. 3
Fig. 3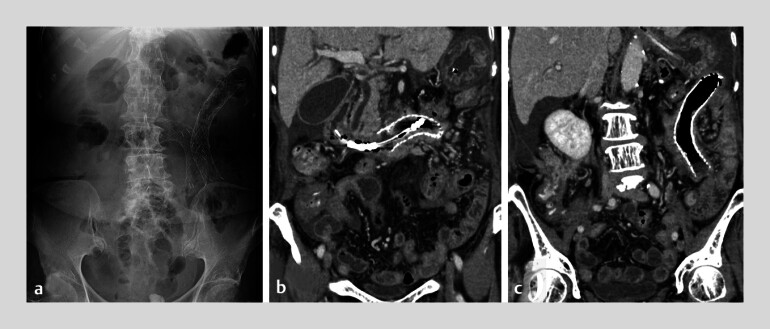 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Biliary and Gastrointestinal Fistulas · Intestinal and Peritoneal Adhesions
An 80-year-old woman who had undergone surgery for pancreatic tail cancer received chemotherapy for peritoneal dissemination recurrence, but the response was poor. She developed vomiting due to stenosis in the ascending part of the duodenum caused by tumor progression ( Fig. 1 a ). After decompression with an ileus tube, a duodenal stent was placed ( Fig. 1 b, c ), resulting in temporary relief. However, vomiting recurred after two weeks, and computed tomography (CT) revealed a jejunal stenosis approximately 20 cm distal to the ligament of Treitz ( Fig. 2 a, b ). An ileus tube was reinserted.
Duodenal stent placement for stenosis in the transverse part of the duodenum. a On the coronal view of the computed tomography (CT), a stricture in the transverse part of the duodenum (arrowhead) and dilatation of the proximal bowel were observed. b The endoscopic duodenal contrast study confirmed stenosis (arrowhead) in the transverse part of the duodenum. c A stent was placed at the stenosis site.
CT image showing a malignant stricture in the jejunum. a The stenosis was located approximately 20 cm from the Treitz ligament to the anal side (arrow). b Axial view.
Given that the narrowing was confined to a localized segment of the proximal jejunum, stent placement was considered appropriate. A colonoscope (CF-H260; Olympus, Tokyo, Japan) was used. A catheter and a 0.025-inch guidewire (GW) were inserted through the existing stent ( Video 1 ). Contrast imaging showed a stenosis 3 cm in length consistent with CT findings ( Fig. 3 a ). A 0.035-inch GW was added to enhance stent deliverability. Two duodenal stents (22 mm × 12 cm and 22 mm × 8 cm; JENTLLY NEO Duodenal Stent; Japan Lifeline, Tokyo, Japan) were selected to prevent kinking ( Fig. 3 b ). Both showed good trackability. The stents were accurately placed, and contrast confirmed adequate distal flow ( Fig. 3 c ). Postoperatively, ileus tube drainage decreased, and CT showed improvement in dilatation ( Fig. 4 a–c ). The patient resumed oral intake.
Stent placement for a malignant jejunal stricture. a The endoscopic duodenal contrast study confirmed stenosis (arrow) in the jejunum. b A stent (22 mm × 12 cm) was placed with sufficient length to prevent kinking on the anal side. An additional stent (22 mm × 8 cm) was placed on the oral side. c Contrast from the ileus tube confirmed smooth flow through the stent lumen into the distal bowel.
Imaging after duodenal stenting. a X-ray after duodenal stenting. b Duodenal stent at the ascending part of the duodenum. c Duodenal stent at the jejunum.
Duodenal stent placement for jejunal obstruction.Video 1
Stent placement is a minimally invasive alternative to surgery for gastrointestinal strictures 1 2 3 . However, placement in distal jejunal strictures is technically difficult due to the need to traverse the ligament of Treitz and navigate tortuous anatomy 4 . In this case, the newly designed stents’ strong outer sheath and low-friction inner surface enabled smooth advancement and accurate deployment in a deep, angulated jejunal segment. This report demonstrates a feasible stenting approach for malignant jejunum obstruction and may represent a valuable therapeutic option.
Endoscopy_UCTN_Code_TTT_1AO_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Krishnamoorthi R Bomman S Benias P Efficacy and safety of endoscopic duodenal stent versus endoscopic or surgical gastrojejunostomy to treat malignant gastric outlet obstruction: systematic review and meta-analysis Endosc Int Open 202210 E 874E 89710.1055/a-1794-063535692924 PMC 9187371 · doi ↗ · pubmed ↗
- 2Uemura S Iwashita T Iwata K Endoscopic duodenal stent versus surgical gastrojejunostomy for gastric outlet obstruction in patients with advanced pancreatic cancer Pancreatology 20181860160729753623 10.1016/j.pan.2018.04.015 · doi ↗ · pubmed ↗
- 3Jeurnink SM Van Eijck CH Steyerberg EW Stent versus gastrojejunostomy for the palliation of gastric outlet obstruction: a systematic review BMC Gastroenterol 2007711010.1186/1471-230X-7-1817559659 PMC 1904222 · doi ↗ · pubmed ↗
- 4Jeurnink SM Repici A Luigiano C Use of a colonoscope for distal duodenal stent placement in patients with malignant obstruction Surg Endosc 20092356256718389314 10.1007/s 00464-008-9880-5 · doi ↗ · pubmed ↗