Multi-holed fully covered self-expandable metal stent to dilate a benign hepaticojejunostomy anastomotic stricture
Tesshin Ban, Yoshimasa Kubota, Yota Hirayama, Kei Ando, Naoto Imura, Shun Sasoh, Takashi Joh

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
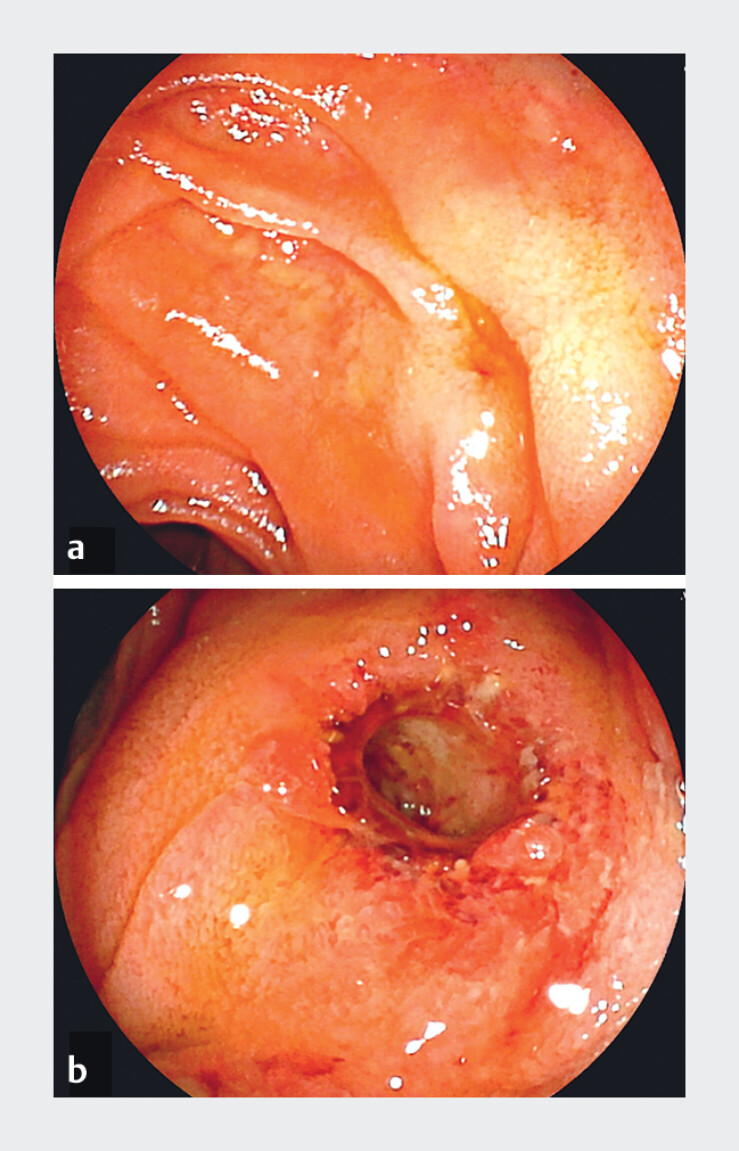 Fig. 1
Fig. 1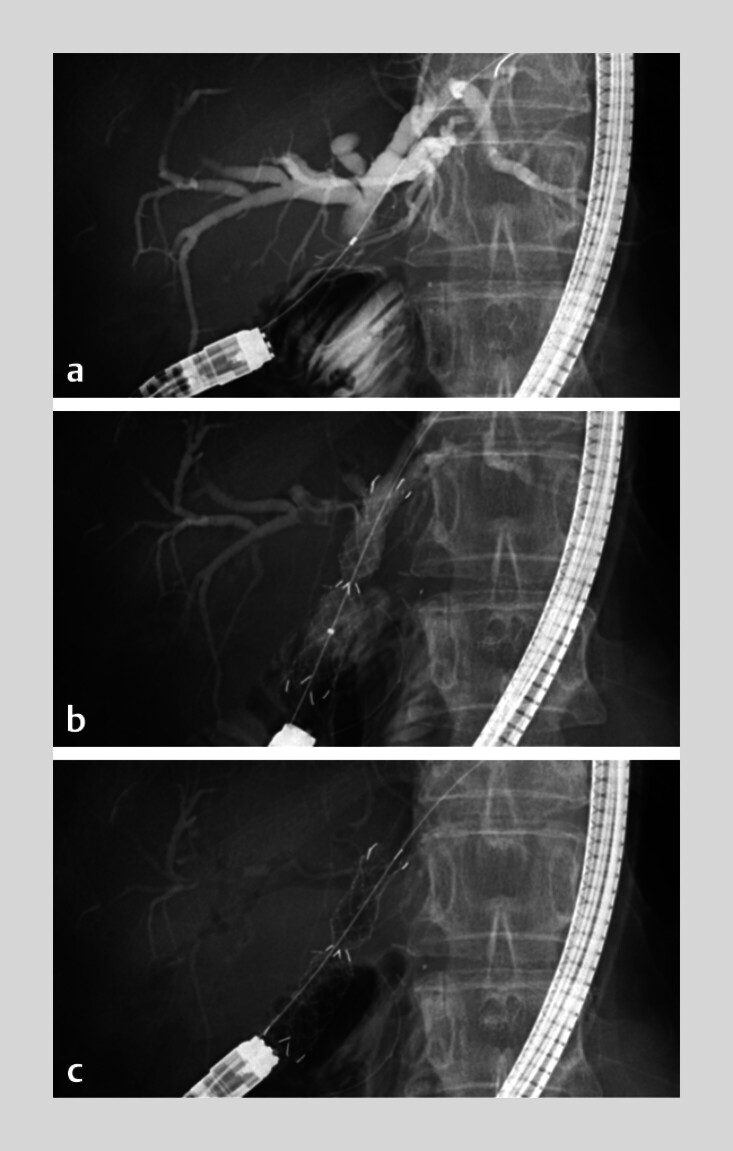 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Esophageal and GI Pathology · Biliary and Gastrointestinal Fistulas
In balloon-assisted enteroscopy (BAE)-guided recanalization in patients with benign hepaticojejunostomy anastomotic strictures (HJAS), balloon dilation followed by plastic stent placement maintains long-term recanalization 1 . Temporary placement of a fully covered self-expandable metal stent (FCSEMS) may increase stricture patency rates. However, an FCSEMS may cause acute cholangitis by blocking the biliary bifurcations. Therefore, additional plastic stents are sometimes required to preserve bifurcations 2 3 . A recently developed removable multi-holed FCSMES (MH-FCSEMS) is designed to preserve the biliary branches even when placed unilaterally in the perihilar stricture 4 5 . Herein, we report a patient in whom the HJAS was successfully recanalized without cholangitis using the MH-FCSEMS under BAE guidance.
A 56-year-old female with a history of robotic pancreatoduodenectomy for duodenal papillary cancer presented with fever and gradually worsening serum transaminase levels, which was suspected to be HJAS.
We attempted BAE-guided recanalization of the HJAS using balloon dilation, followed by temporary unilateral placement of the MH-FCSEMS at the anastomosis ( Video 1 ). The HJAS had a pinhole-like appearance on the jejunal side and was 8 mm long ( Fig. 1 a , Fig. 2 a ). We dilated the HJAS with a 6-mm dilation balloon catheter, followed by deployment of a single MH-FCSEMS (HANAROSTENT Biliary Multi-hole NEO, 10 mm, 5 cm; Boston Scientific, Marlborough, Massachusetts, USA) across the stricture up to the left hepatic duct ( Fig. 2 b ). After stent deployment, remnant contrast medium in the bilateral intrahepatic duct was quickly aspirated through the MH-FCSEMS, and these ducts changed into pneumobilia, even though the MH-FCSEMS obstructed the right hepatic duct and segment IV bile duct ( Fig. 2 c ). The postprocedural clinical course was uneventful, and the HJAS was successfully recanalized when the stent was removed one month later ( Fig. 1 b ).
Endoscopic views of hepaticojejunostomy anastomotic stricture. a The anastomosis site shows a pinhole-like appearance before placement of a multi-holed fully covered self-expandable metal stent (MH-FCSMES) during balloon-assisted enteroscopy. b The anastomosis stricture is considered sufficiently recanalized when the stent is removed after one month from the index procedure.
Fluoroscopic images showing the placement of an MH-FCSMES at the hepaticojejunostomy anastomotic stricture during balloon-assisted enteroscopy. a The severe stricture measured 8mm in length. b The deployed MH-FCSMES is observed to be obstructing the right hepatic duct and the segment IV bile duct. c However, multiple holes in the stent membrane allow for the aspiration of bilateral remnant contrast medium and its replacement with the insufflated gas.
Multi-holed fully covered self-expandable metal stent to dilate a benign hepaticojejunostomy anastomotic stricture.Video 1
Temporary placement of the MH-FCSEMS for HJAS is a simple procedure aimed at preventing segmental cholangitis and ensuring adequate stricture dilation.
Endoscopy_UCTN_Code_TTT_1AR_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1T Kato H Miyamoto K Comparison between endoscopic biliary stenting combined with balloon dilation and balloon dilation alone for the treatment of benign hepaticojejunostomy anastomotic stricture J Gastrointest Surg 2020241352135831228084 10.1007/s 11605-019-04297-8 · doi ↗ · pubmed ↗
- 2Sato T Kogure H Nakai Y Endoscopic treatment of hepaticojejunostomy anastomotic strictures using fully-covered metal stents Dig Endosc 20213345145710.1111/den.1377332559351 · doi ↗ · pubmed ↗
- 3Hanaoka T Okuwaki K Watanabe M Efficacy and safety of a 6-month placement of a fully covered self-expanding metal stent for refractory or recurrent hepaticojejunostomy anastomotic stricture via balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography DEN Open 20256 e 7017210.1002/deo 2.7017240599978 PMC 12210144 · doi ↗ · pubmed ↗
- 4Park JS Jeong S Kobayashi M Safety, efficacy, and removability of a fully covered multi-hole metal stent in a swine model of hilar biliary stricture: a feasibility study Endosc Int Open 20197 E 498E 50310.1055/a-0846-077531041366 PMC 6447406 · doi ↗ · pubmed ↗
- 5Kobayashi M Development of a biliary multi-hole self-expandable metallic stent for bile tract diseases: A case report World J Clin Cases 201971323132810.12998/wjcc.v 7.i 11.132331236396 PMC 6580344 · doi ↗ · pubmed ↗