Endoluminal radiofrequency ablation for ingrowth occlusion after endoscopic ultrasound-guided hepaticogastrostomy with bridging stent placement
Kenjiro Yamamoto, Takayoshi Tsuchiya, Ryosuke Tonozuka, Shuntaro Mukai, Hiroyuki Kojima, Noriyuki Hirakawa, Takao Itoi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
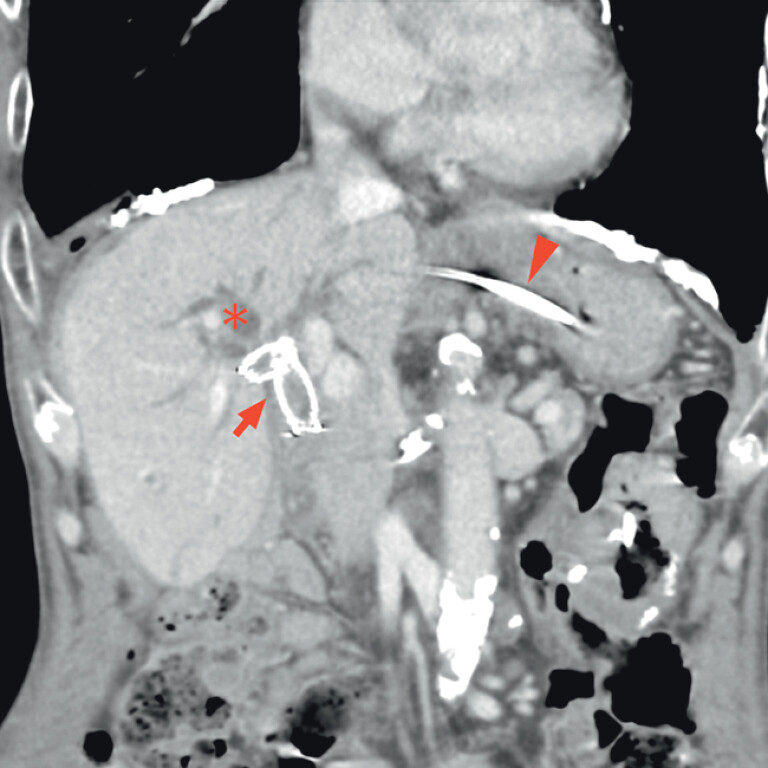 Fig. 1
Fig. 1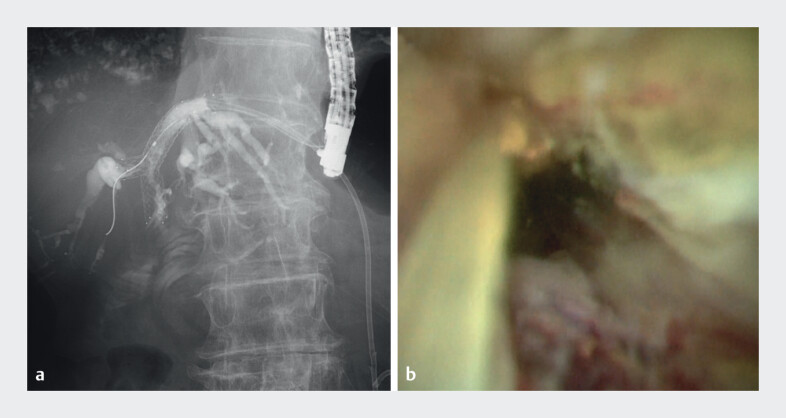 Fig. 2
Fig. 2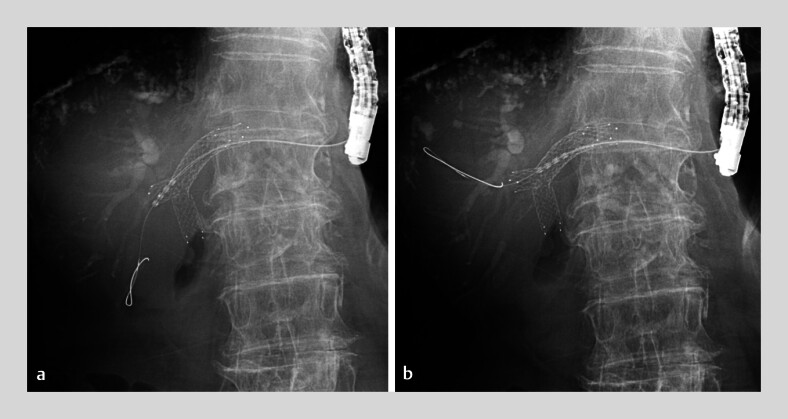 Fig. 3
Fig. 3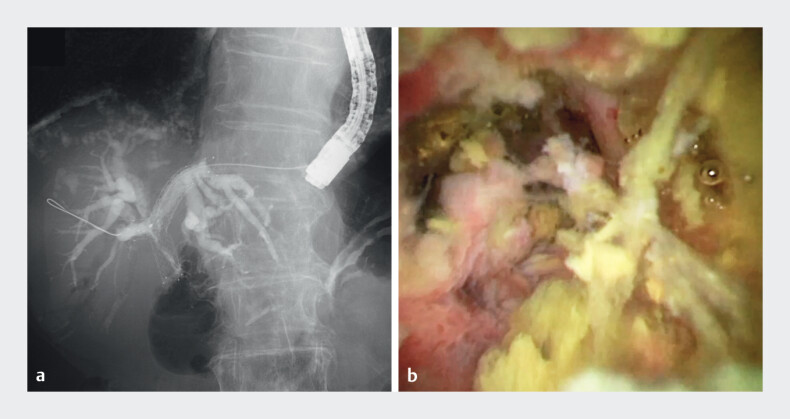 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments · Cholangiocarcinoma and Gallbladder Cancer Studies
Endoscopic ultrasound-guided hepaticogastrostomy with bridging stent placement is a useful drainage option when endoscopic retrograde cholangiopancreatography fails for reasons such as inaccessible papillae or surgical anastomosis, particularly in patients with malignant hilar biliary obstruction who require bilateral drainage 1 2 . Recent advances in chemotherapy, such as targeted drugs for specific gene mutations, have improved prognosis in biliary tract cancers 3 . Therefore, the management of recurrent biliary obstruction after stent placement is also an important issue. Endoluminal radiofrequency ablation (RFA) is a novel procedure for biliary diseases and may be an option for treating ingrowth occlusion after metal stent deployment 4 5 .
An 80-year-old man was admitted with obstructive jaundice during chemotherapy for local relapse after Whipple surgery for cholangiocarcinoma. He had previously undergone right hepatic drainage with bridging metal stent placement through the hepaticogastrostomy route. Contrast-enhanced computed tomography demonstrated dilatation of the anterior bile duct ( Fig. 1 ). Cholangiography and peroral cholangioscopy (POCS) revealed stent occlusion due to tumor ingrowth ( Fig. 2 ). Additional stent placement through previously inserted bilateral metal stents was considered technically challenging. Thus, RFA was performed with a temperature-controlled RF catheter (ELRA; StarMed Co., Goyang, Korea). The RF generator (VIVA Combo; StarMed Co.) was set to a maximum temperature of 80°C and power of 7W for a 2-min duration and was then connected to an 18-mm RF catheter. Ablation was performed stepwise, spanning the stricture ( Fig. 3 ). After RFA, a temporary endoscopic nasobiliary drainage tube was placed. Four days after RFA, cholangiography and POCS confirmed ablation of the ingrowth regions and recanalization of the stent lumen ( Fig. 4 ; Video 1 ). The patient was discharged after plastic stent placement through the hepaticogastrostomy route. Recanalization using RFA was clinically successful, with no recurrence of biliary obstruction for more than 3 months.
Contrast-enhanced computed tomography showing dilatation of the anterior bile duct (asterisk). For local relapse after Whipple surgery for cholangiocarcinoma, right hepatic drainage with bridging metal stent placement through the hepaticogastrostomy route had previously been performed and another metal stent placed from the jejunum to the left hepatic duct in a stent-in-stent configuration (arrow). A plastic stent had been placed across the hepaticogastrostomy route (arrowhead).
Stent occlusion due to tumor ingrowth: a cholangiographic view; b peroral cholangioscopic view.
Stepwise endoluminal radiofrequency ablation spanning the stricture: fluoroscopic view.
Successful ablation of the ingrowth regions and recanalization of the stent lumen: a cholangiographic view; b peroral cholangioscopy.
Radiofrequency ablation for ingrowth occlusion after endoscopic ultrasound-guided hepaticogastrostomy with bridging stent placement.Video 1
Endoscopy_UCTN_Code_TTT_1AR_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ogura T Sano T Onda S Endoscopic ultrasound-guided biliary drainage for right hepatic bile duct obstruction: novel technical tips Endoscopy 201547727510.1055/s-0034-137811125264761 · doi ↗ · pubmed ↗
- 2Takeshita K Hijioka S Nagashio Y Comparison of stent patency between EUS-guided hepaticogastrostomy with bridging and endoscopic transpapillary biliary drainage for hilar obstruction Endosc Int Open 202412 E 875E 88610.1055/a-2333-789838989254 PMC 11236478 · doi ↗ · pubmed ↗
- 3Shionoya K Sofuni A Mukai S Initial use experience of durvalumab plus gemcitabine and cisplatin for advanced biliary tract cancer in a Japanese territory center Cancers (Basel)20251731410.3390/cancers 1702031439858096 PMC 11764297 · doi ↗ · pubmed ↗
- 4Yamamoto K Itoi T Sofuni A Verification in an animal study of the appropriate settings for a novel radiofrequency generator in radiofrequency ablation therapy for residual intraductal lesions after endoscopic papillectomy (with video)Dig Endosc 202510.1111/den.14986 PMC 1216241739833995 · doi ↗ · pubmed ↗
- 5Inoue T Ibusuki M Kitano R Endoscopic radiofrequency ablation for ingrowth occlusion after bilateral metal stent placement for malignant hilar biliary obstruction: a prospective pilot study Gastrointest Endosc 202397282290010.1016/j.gie.2022.09.02536220379 · doi ↗ · pubmed ↗