Per-oral endoscopic tunneling transgastric drainage of an acute pancreatic necrotic collection
Anastasios C. Manolakis, Tryfonas Mpektsis, Konstantinos Argyriou, Eirini Deligianni, Dimitrios Chougias, Ashish Sharma, Andreas Kapsoritakis

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
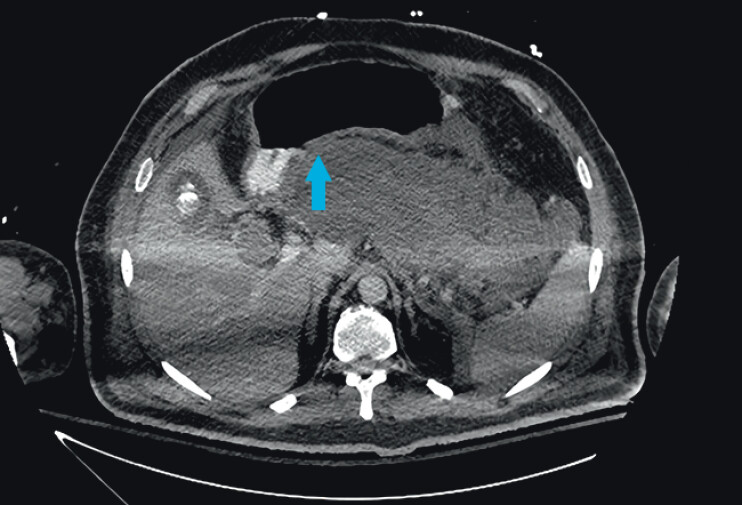 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatitis Pathology and Treatment · Pancreatic and Hepatic Oncology Research · Gastrointestinal disorders and treatments
Acute pancreatic necrotic collections (APNCs) complicating necrotic pancreatitis are managed conservatively. Upon onset of complications, percutaneous, endoscopic ultrasound (EUS)-guided or surgical drainage can be applied 1 2 .
A 40-year-old with severe necrotic pancreatitis became critically ill on week 3 due to an infected APNC, diagnosed via computed tomography (CT). Percutaneous and EUS-drainage failed while surgery carried a high risk of fatal outcomes. During gastroscopy, no visible “bulge” corresponding to a compression or indentation from the collection was identified. Based on anatomy and CT, the left lateral–posterior wall of the corpus–antrum junction below the incisura exhibited optimal APNC-gastric wall contact ( Fig. 1 ). A novel endoscopic technique conforming to the principles of NOTES, termed per-oral endoscopic tunneling transgastric drainage (POET-D), was applied as a rescue therapy ( Video 1 ).
Computed tomography image showing the site of optimal contact (blue arrow) between the pancreatic collection and the gastric wall.
Per-oral endoscopic tunneling transgastric drainage (POET-D) of an acute pancreatic necrotic collection.Video 1
First, submucosal injection of 10 cc indigo carmine-solution was performed at the left lateral–posterior wall of the corpus–antrum junction. A mucosal incision was made using an endoscopic knife. A short submucosal tunnel was created. Muscle fibers and serosa were gradually dissected near the distal end of the tunnel to allow for the preservation of a mucosal flap above the distal defect. The endoscope entered the omental bursa. The omentum, spleen and splenic ligament could be visualized. 560 cc of Klebsiella spp-infected APNCs were aspirated and the cavity was lavaged with saline and gentamycin. A nasobiliary tube was placed inside the omental bursa for further drainage and lavage. Within 48 hours the patient improved. The tube was removed and the defect was closed with clips.
POET-D allows for preservation of a mucosal flap over the sero-muscular defect and continuous visualization of adjacent structures during dissection. It can provide rapid, large-volume drainage of viscous contents and lavage of infected cavities. POET-D can treat complicated cases of APNCs, potentially filling a therapeutic gap in-between percutaneous, EUS and surgical procedures.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Baron TH Di Maio CJ Wang AY American Gastroenterological Association Clinical Practice Update: Management of Pancreatic Necrosis Gastroenterology 2020158677510.1053/j.gastro.2019.07.06431479658 · doi ↗ · pubmed ↗
- 2Arvanitakis M Dumonceau JM Albert J Endoscopic management of acute necrotizing pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) evidence-based multidisciplinary guidelines Endoscopy 20185052454610.1055/a-0588-536529631305 · doi ↗ · pubmed ↗