Cystic Duct Remnant Leading to Stump Cholelithiasis
Ayushi Rathore, Krishnanand Anand, Shivam Nagaich

TL;DR
A patient developed gallstone-like symptoms from a leftover cystic duct after gallbladder removal surgery, which was resolved through surgical excision.
Contribution
Highlights cystic duct remnant cholelithiasis as a rare but diagnosable cause of post-cholecystectomy syndrome.
Findings
Residual cystic duct with concretions was identified as the cause of persistent symptoms after cholecystectomy.
Surgical excision of the cystic duct remnant provided effective treatment and symptom relief.
Imaging techniques like MRCP were crucial for diagnosing the condition.
Abstract
A 42-year-old male presented with a two-month history of right upper quadrant abdominal pain, worsening over four days. Six months earlier, he had undergone a laparoscopic cholecystectomy. Examination revealed no jaundice or tenderness, and liver function tests were normal. The patient’s basic inflammatory markers were within the normal range. Ultrasound revealed a residual gallbladder stump or dilated cystic duct with a calculus, and magnetic resonance cholangiopancreatography (MRCP) demonstrated a 3 × 1 cm stump with an 8 mm hypointense focus. Endoscopic retrograde cholangiopancreatography (ERCP) was unsuccessful due to distorted anatomy. Surgical exploration confirmed a cystic duct remnant containing sludge and concretions, which was excised completely. Postoperative recovery was uneventful, and histopathology revealed chronic inflammatory changes consistent with cystic duct stump…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
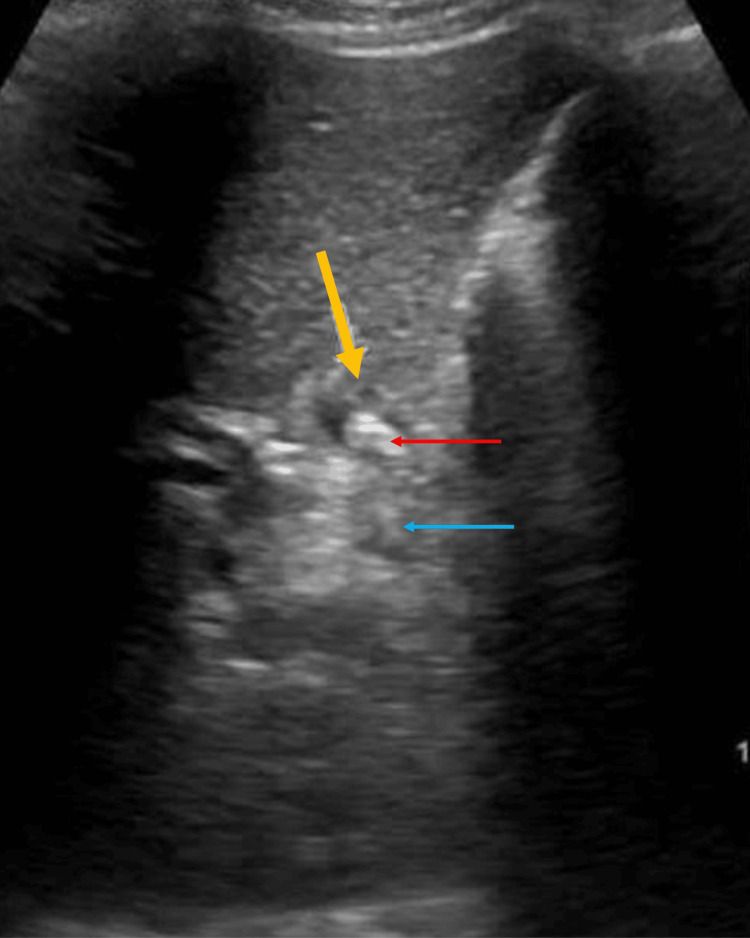 Figure 1
Figure 1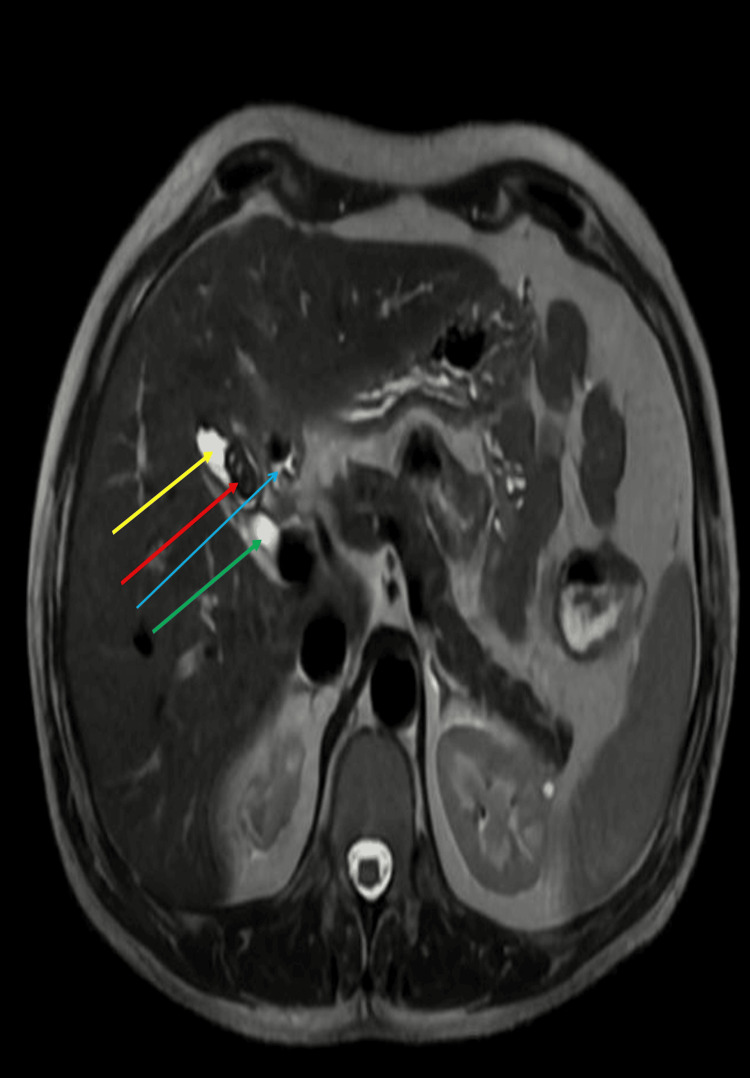 Figure 2
Figure 2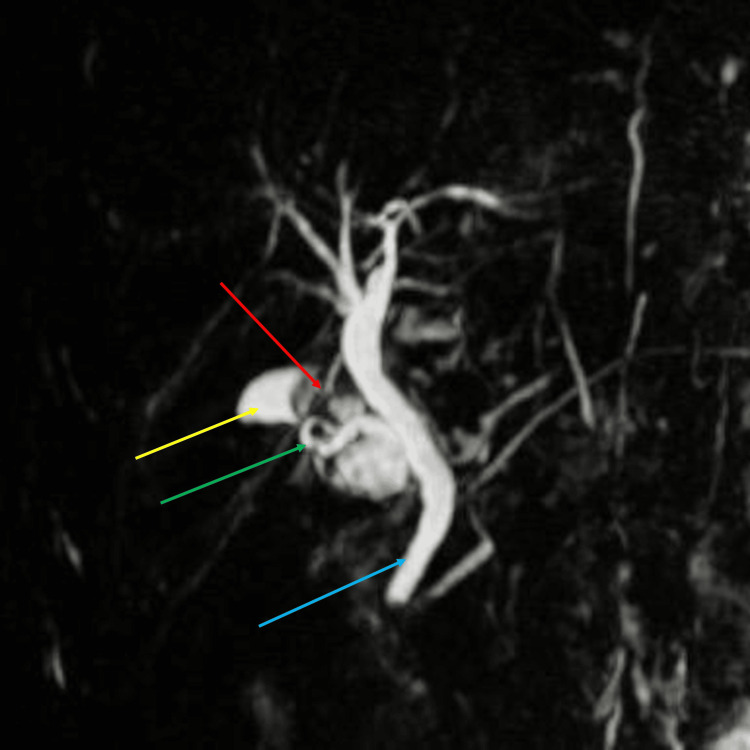 Figure 3
Figure 3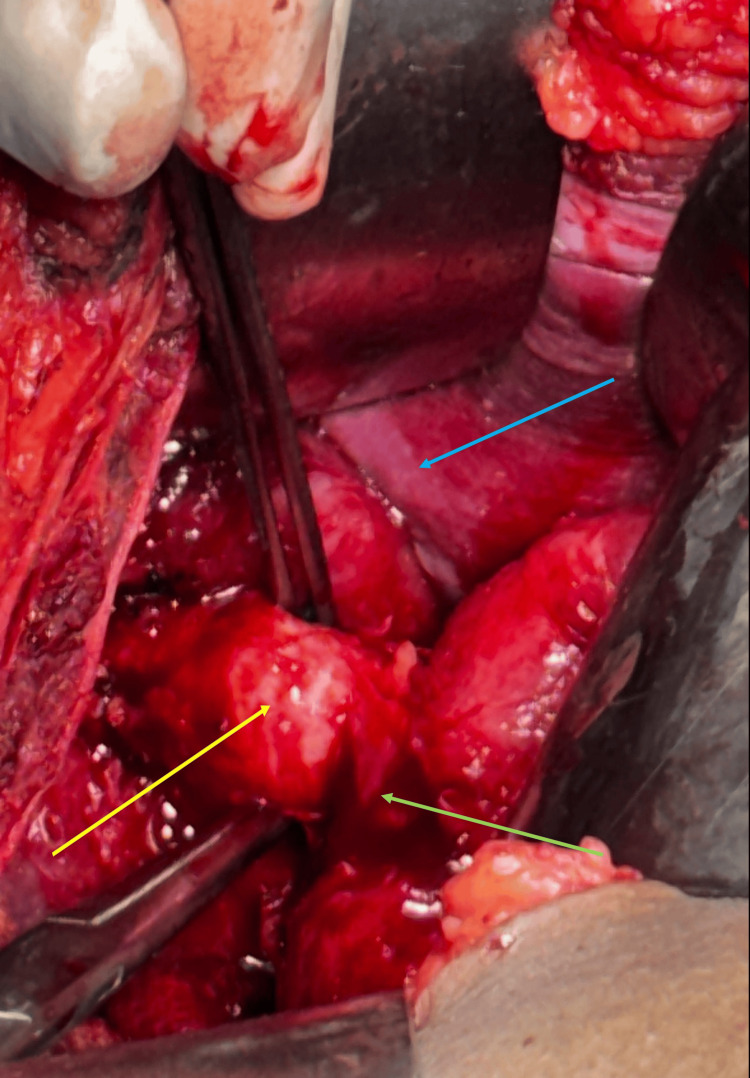 Figure 4
Figure 4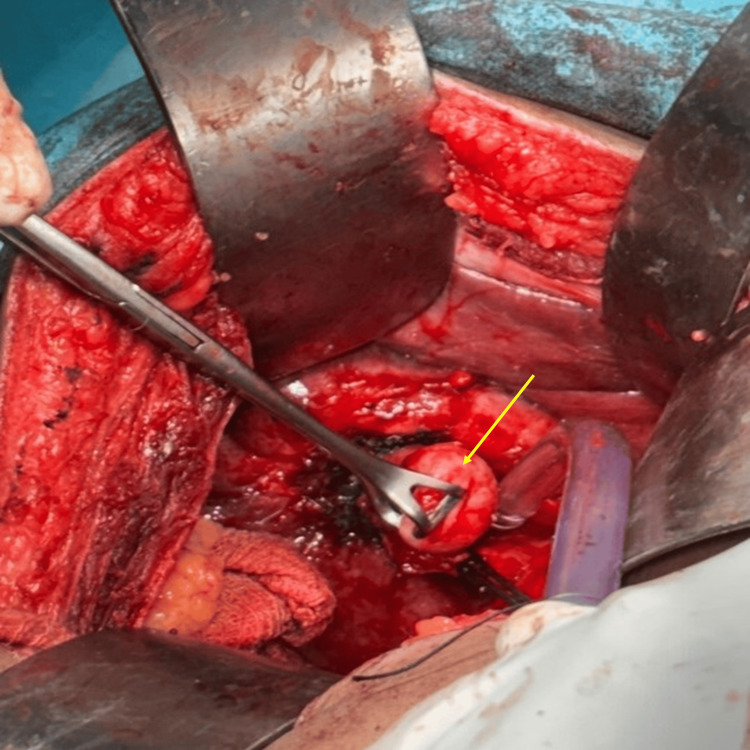 Figure 5
Figure 5 Figure 6
Figure 6 Figure 7
Figure 7| Timeline | Laboratory findings | Imaging findings | Intervention/outcome |
| Admission (Day 0) | Normal LFTs, amylase, lipase; no leukocytosis | Ultrasound: residual gallbladder stump/dilated cystic duct with calculus | Supportive management initiated |
| Day 1 | Stable labs | MRCP: 3 × 1 cm stump with 8 mm focus | – |
| Day 2 | Stable labs | – | ERCP was attempted but was unsuccessful due to distorted anatomy |
| Day 3 (Surgery, POD 0) | No leukocytosis, stable vitals | – | Open surgical exploration performed; cystic duct stump excised with concretions and sludge. IV antibiotics and analgesics were administered for 48 hours |
| POD 2 | – | – | Oral intake resumed |
| POD 3 | – | – | Drain removed |
| POD 5 | – | – | Patient discharged |
| Follow-up (6 months) | – | – | Patient remains well and asymptomatic |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Pediatric Hepatobiliary Diseases and Treatments · Biliary and Gastrointestinal Fistulas
Introduction
Cystic duct remnant stone formation is an uncommon but recognized cause of post-cholecystectomy syndrome (PCS), with an incidence reported between 2.5% and 5% [1]. Although laparoscopic cholecystectomy remains the gold standard for symptomatic gallstone disease, a subset of patients continues to experience biliary symptoms postoperatively [2]. PCS occurs in 10-40% of patients [3] and may present within days or even decades after surgery. It encompasses a wide spectrum of manifestations, including abdominal pain, nausea, vomiting, jaundice, and abdominal distension. Non-biliary causes include peptic ulcer disease, gastroesophageal reflux, irritable bowel syndrome, and chronic pancreatitis, whereas biliary causes include strictures, bile leaks, retained or dropped stones, bilomas, abscesses, long cystic duct remnants, sphincter of Oddi dysfunction, and bile salt-induced gastritis [4]. It is important to distinguish two separate entities: (a) residual gallbladder with retained stones due to incomplete or subtotal excision, and (b) cystic duct stump calculi or sludge (cystic duct remnant syndrome). The latter results from a stump longer than 1 cm left behind, which predisposes to bile stasis and stone formation [5]. Residual stump stones remain a diagnostic challenge, and imaging modalities such as ultrasound, magnetic resonance cholangiopancreatography (MRCP), and endoscopic retrograde cholangiopancreatography (ERCP) are valuable in identifying this rare complication [5]. Awareness of these distinctions is essential for accurate diagnosis and to guide the appropriate surgical approach.
Case presentation
A 42-year-old male presented to the surgical outpatient department with complaints of right upper quadrant abdominal pain for two months, which had worsened over the previous four days. The pain radiated to the back and was not associated with food intake. The patient denied nausea, vomiting, fever, anorexia, or weight loss.
The patient had undergone laparoscopic cholecystectomy seven months earlier for acute cholecystitis of one month’s duration. Intraoperatively, the gallbladder was grossly distended with dense omental adhesions. Because of the distension and acutely inflamed wall, it was difficult to grasp the gallbladder; therefore, aspiration was performed, yielding approximately 100 mL of purulent fluid. The cystic duct and artery were clipped, and the gallbladder was completely removed.
On examination, the abdomen was soft and non-tender, and there was no jaundice. Based on this history, cholelithiasis was initially considered unlikely, and the patient was evaluated for alternative causes. Liver function tests, serum amylase, and lipase were all within normal limits, with no biochemical evidence of obstructive jaundice. The patient’s total leukocyte count and C-reactive protein were within normal range, consistent with the absence of systemic infection. Abdominal ultrasound revealed a residual gallbladder stump or dilated cystic duct with a calculus (Figure 1).
Abdominal ultrasound showing residual gallbladder stump or dilated cystic duct remnant (yellow arrow) with echogenic foci (red arrow) casting posterior acoustic shadow (blue arrow), suggestive of calculus.
MRCP demonstrated a 3 × 1 cm T2 hyperintense outpouching with an 8 mm T2 hypointense focus in the gallbladder fossa, consistent with a residual gallbladder stump calculus or a dilated cystic duct with a surgical clip (Figures 2, 3).
Transverse section of magnetic resonance cholangiopancreatography (MRCP) showing stump of dilated cystic duct (yellow arrow), calculus (red arrow), surgical clip (light blue arrow), and cystic duct (green arrow).
Magnetic resonance cholangiopancreatography (MRCP) showing stump of dilated cystic duct (yellow arrow), calculus (red arrow), cystic duct (green arrow), and common bile duct (blue arrow).
ERCP was attempted for both diagnostic confirmation and possible therapeutic stone retrieval. However, cannulation was unsuccessful due to the distorted anatomy of the sphincter of Oddi.
The patient subsequently underwent open surgical exploration through a right subcostal incision. Dense adhesions were encountered and carefully released using sharp and blunt dissection. The common bile duct was identified, and a remnant of the enlarged cystic duct was palpated. The cystic duct remnant was dissected using a right-angled (Mixter) forceps, ligated with suture material, and excised. A size 28 abdominal drain was placed in the gallbladder fossa (Figures 4-7).
Intraoperative image showing dilated cystic duct remnant (yellow arrow), liver (blue arrow), and bowel (green arrow).
Dilated cystic duct remnant grasped with Babcock forceps (yellow arrow).
Cut section of the dilated cystic duct remnant showing sludge.
Excised specimen of the dilated cystic duct remnant.
The postoperative course was uneventful, and the patient did not require ICU admission. Postoperative management included intravenous antibiotics and analgesics for 48 hours, followed by oral analgesics. The patient tolerated early oral intake, and the abdominal drain was removed on postoperative day three. A summary of the patient’s clinical course, laboratory values, imaging, and interventions is presented in Table 1.
Histopathological examination revealed chronic inflammatory changes with focal epithelial hyperplasia, consistent with post-cholecystectomy cystic duct stump pathology. The patient was well on a six-month follow-up.
Written informed consent was obtained from the patient for participation in this study and for the publication of this case report, including accompanying images.
Discussion
PCS refers to the persistence or recurrence of biliary or gastrointestinal symptoms following cholecystectomy. Laparoscopic cholecystectomy provides long-term symptomatic relief in nearly 85% of patients, yet a subset continues to experience symptoms resembling their preoperative state [2,6]. Stump or remnant calculi are particularly challenging to diagnose. Ultrasonography may demonstrate acoustic shadows suggestive of stones, but MRCP and ERCP remain the preferred diagnostic tools, though even these may miss small or anatomically obscured calculi [7-9]. Cystic duct remnant syndrome (CDRS), as in the present case, occurs when a residual cystic duct longer than 1 cm is left behind, with a reported prevalence of less than 2.5% [10]. A long cystic duct stump acts as a blind loop that predisposes to bile stasis, sludge, and subsequent calculus formation [1,10]. Difficult dissections in the setting of empyema, severe inflammation, or dense adhesions often result in a longer residual stump or missed stones, further increasing the risk [1,4,11,12]. Emergency or technically challenging cholecystectomies, including subtotal procedures, are additional contributors to cystic duct remnant pathology [8,9,11,12]. Symptoms may develop soon after surgery or present years later as biliary colic, jaundice, or recurrent infection [7,9]. In our patient, MRCP confirmed biliary PCS. However, ERCP failed due to the distorted anatomy of the sphincter of Oddi. Residual gallbladder with stones requires a complete cholecystectomy, whereas cystic duct stump stones (as in this case) require cystic duct exploration and excision. Although ERCP is typically considered the first-line therapeutic option, recent advances such as laparoscopic re-exploration and laparoscopic cystic duct excision offer safe, minimally invasive alternatives when ERCP fails or is not technically feasible [8,11,12]. In this case, open surgical excision of the stump was performed successfully, providing definitive treatment. Reoperations in the Calot’s triangle can be technically demanding due to chronic inflammation and scarring. Open surgery, however, continues to be a safe and effective alternative, as demonstrated here. This case emphasizes the importance of meticulous surgical technique during the index cholecystectomy to prevent long cystic duct remnant complications. Additionally, thorough imaging and clinical vigilance are critical for the diagnosis of cystic duct stump stones, while complete excision of the stump remains the definitive treatment, offering complete cure.
Conclusions
Long cystic duct remnants containing sludge or concretions represent a rare but preventable cause of post-cholecystectomy syndrome. In our patient, MRCP confirmed the diagnosis, while ERCP failed due to distorted anatomy. Open surgical excision of the stump was successfully performed and provided durable symptom relief. These findings are consistent with published data demonstrating MRCP’s high diagnostic accuracy, ERCP’s limited therapeutic role due to technical challenges, and the efficacy of surgical excision in achieving symptom resolution. This case underscores the importance of meticulous surgical technique during the index cholecystectomy to avoid leaving a long cystic duct stump. Thorough preoperative imaging, careful intraoperative dissection, and timely reoperation when indicated remain the cornerstones for preventing and managing this uncommon but clinically significant complication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Remnant gall bladder and cystic duct stump stone after cholecystectomy: tertiary multicenter experience Int Surg J Mageed SAA Omar MA Redwan AA 3478348352018 http://doi.org/10.18203/2349-2902.isj 20184612
- 2Clinical patterns of postcholecystectomy syndrome Ann Hepatobiliary Pancreat Surg Shirah BH Shirah HA Zafar SH Albeladi KB 5257222018 http://doi.org/10.14701/ahbps.2018.22.1.522953605610.14701/ahbps.2018.22.1.52PMC 5845611 · doi ↗ · pubmed ↗
- 3The persistence of symptoms following cholecystectomy Ann Surg Womack NA Crider RL 315512619471785897610.1097/00000658-194707000-00004 PMC 1803303 · doi ↗ · pubmed ↗
- 4Postcholecystectomy syndrome (PCS)Int J Surg Jaunoo SS Mohandas S Almond LM 1517820101985761010.1016/j.ijsu.2009.10.008 · doi ↗ · pubmed ↗
- 5Endoscopic diagnosis and treatment of post-cholecystectomy syndrome Hepatobiliary Pancreat Dis Int Zhou PH Liu FL Yao LQ Qin XY 11712022003 http://pubmed.ncbi.nlm.nih.gov/14607662/14607662 · pubmed ↗
- 6Post-cholecystectomy syndrome: a retrospective study analysing the associated demographics, aetiology, and healthcare utilization Transl Gastroenterol Hepatol Saleem S Weissman S Gonzalez H Rojas PG Inayat F Alshati A Gaduputi V 58620213480558010.21037/tgh.2019.11.08PMC 8573368 · doi ↗ · pubmed ↗
- 7Insufficient cholecystectomy diagnosed by endoscopic ultrasonography Endoscopy Hassan H Vilmann P 2362383620041498622410.1055/s-2004-814254 · doi ↗ · pubmed ↗
- 8Surgical management of cystic duct stump stone or gall bladder remnant stone Indian J Surg Kar A Gulati S Mohammed S Valappil MV Sarala BB Ghatak S Bhattacharyya A 2842878020182997376310.1007/s 12262-018-1724-5PMC 6014961 · doi ↗ · pubmed ↗