Chimeric Antigen Receptor-Engineered Natural Killer (CAR-NK) Cell Therapy in Acute Myeloid Leukemia: A Systematic Review of the Literature
Mayra Steffania Novoa Arias

TL;DR
This paper reviews CAR-NK cell therapy for AML, assessing its potential as a safe and effective treatment while identifying key challenges.
Contribution
A systematic review of CAR-NK cell therapy in AML, highlighting current progress and barriers to clinical application.
Findings
CAR-NK cells show potential as a safe and scalable treatment for AML.
Important obstacles remain before CAR-NK therapy can be used clinically.
Future development directions are suggested based on current findings.
Abstract
Chimeric antigen receptor (CAR)-engineered natural killer (NK) cells are attracting considerable interest as a potential therapeutic option in acute myeloid leukemia (AML), driven by the search for safe, scalable, and effective alternatives. To provide an overview of the current state of the field, a systematic review was performed to evaluate the safety and efficacy of CAR-NK cells for AML. The findings suggest possible directions for future development and also highlight important obstacles that must be addressed before they can be used in clinical settings. Therefore, although CAR-NK therapy remains in its early stages, its eventual application in AML is possible if these barriers can be resolved.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
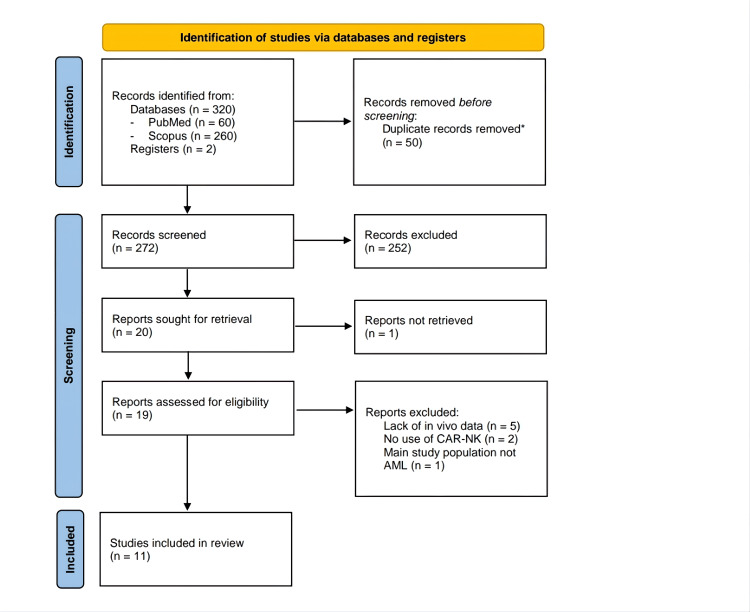 Figure 1
Figure 1| Type of bias | Selection bias | Performance bias | Detection bias | Attrition bias | Reporting bias | Other | ||||
| Domain | Sequence generation | Baseline characteristics | Allocation concealment | Random housing | Blinded interventions | Random outcome assessment | Blinded outcome | Incomplete outcome data | Selective reporting | Other sources of bias |
| Study | Outcome | |||||||||
| [ | U | U | U | U | U | U | U | U | Y | Y |
| [ | U | U | U | U | U | U | U | Y | Y | Y |
| [ | U | U | U | U | U | U | U | Y | Y | Y |
| [ | U | U | U | U | U | U | U | Y | Y | N |
| [ | U | U | Y | U | U | U | Y | Y | Y | Y |
| [ | U | U | Y | U | U | U | U | Y | Y | N |
| [ | U | U | U | U | U | U | U | Y | Y | Y |
| [ | U | U | U | U | U | U | U | Y | Y | N |
| [ | U | U | Y | U | U | U | U | Y | Y | Y |
| [ | U | U | Y | U | U | U | U | Y | Y | Y |
| Study | NK cell source | Antigen-binding domain | CAR generation | Costimulatory domain | Transduction method | Transduction efficiency |
| Albinger et al. 2022 [ | PB | CD33 | 2nd | 4-1BB-CD3ζ | Lentivirus | 35-60% |
| Albinger et al. 2024 [ | PB | CD33 | 2nd | 4-1BB-CD3ζ | Lentivirus | 28-32% |
| Caruso et al. 2022 [ | PB | CD123 | 2nd | 4-1BB-CD3ζ | Retrovirus | 58,8% |
| Christodoulou et al. 2021 [ | PB | CD123 | 2nd - 4th | 2B4-CD3ζ | Retrovirus | 21-98% |
| 4-1BB-CD3ζ | ||||||
| 2B4-CD3ζ-sIL15 | ||||||
| Dong et al. 2022 [ | PB | NPM1c + HLA-A2 | 2nd - 4th | 4-1BB-CD3ζ | Lentivirus | 65% |
| 4-1BB-CD3ζ-m15 | ||||||
| Du et al. 2021 [ | PB | NKG2D | 2nd - 4th | 4-1BB-CD3ζ | Non-viral transposons | 63-90% |
| 4-1BB-CD3ζ-sIL15 | ||||||
| Mansour et al. 2023 [ | NK-92 - hUC | FLT3 | 2nd - 4th | CD28-CD3ζ | Lentivirus | 46.30% |
| 2B4-CD3ζ | ||||||
| CD28-CD3ζ-sIL15 | ||||||
| Morgan et al. 2021 [ | Non-irradiated NK92 | CD123 | 4th | 4-1BB-CD3ζ-hIL15 | Retrovirus | N.R |
| Salman et al. 2019 [ | NK-92 | CD4 | 3rd | CD28-4-1BB-CD3ζ | Lentivirus | 85% |
| Tang et al. 2018 [ | NK-92 | CD33 | 3rd | CD28-4-1BB-CD3ζ | Lentivirus | 90% |
| Zhang et al. 2023 [ | PB | CD33 + B16 VHH* | 2nd | 4-1BB-CD3ζ | Lentivirus | 45-60% |
| Study | Xenograft (cells) | Type of transplanted cells | Leukemic burden | ||||
| Treatment - Control | Tt | n | Total flux (p/s) | Statistical Test | p-value | ||
| Mean ± SD / (range) | |||||||
| Albinger et al. 2022 [ | OCI-AML2 | CD33-CAR-NK (1 dose) | 21 | 7 | 1.2×108 (1x108 - 2x1010) | Median ± Range | N.R |
| Ctrl: NT-NK | 5×1010 (1.7x1010 - 2.4x109) | ||||||
| CD33-CAR-NK (3 doses) | 21 | 7 | 1.5×108 (1x108 - 4.8x108) | Median ± Range | N.R | ||
| Ctrl: NT-NK | 6 | 1.8×1010 (1.4x1010 - 2.7x1010) | |||||
| Albinger et al. 2024 [ | OCI-AML2 | CD33-CAR-NK (PROD/ SS) | 18 | 9 | 8.7x100 (2.3x101) ** | Mean±SD | N.R |
| Ctrl 1: CD33-CAR-NK | 9 | 4.6x100 (5.7x101) ** | Mean±SD | ||||
| Ctrl: 2 NT-NK | 7 | 1.1x106 (8.2x108) ** | Mean±SD | ||||
| Caruso et al. 2022 [ | THP-1 | CD123-CAR-NK | 50 | 4 | 5.4×105 (4.8x105 - 2.3x107) | Median ± Range | N.R |
| Ctrl 1: CD123-CAR-T | 4.4×105 (3.2x105 - 2.2x1010) | ||||||
| Ctrl 2: NT-NK | 30 | 5.5×109 (2.3 - 6.6x109) | |||||
| Christodoulou et al. 2021 [ | MV-4-11 | CD123-2B4.ζ CAR-NK | 14 | (8-12) | 1.9×104 (5.3x103 - 9.4x104) | ANOVA | <0.01 |
| Ctrl 1: 4-1BB.ζ CARNK | 4.3×104 (1.1x104 - 9.5x104) | ||||||
| Ctrl 2: NT-NK | 1.2×105 (2.8x104 - 2.4x105) | <0.0001 | |||||
| 2B4.ζ/sIL-15 CAR-NK | 14 | (5-7) | 5.3×103 (2x103 - 1.2x104) | ANOVA | N.R | ||
| Ctrl 1: 2B4.ζ CARNK | 7.1×103 (1x103 - 2.3x104) | ||||||
| Ctrl 2: NT-NK | 1.4×105 (5.2x104 - 2.9x105) | <0.0001 | |||||
| MOLM-13 | 2B4.ζ/sIL-15 CAR-NK | 14 | 5 | 1.3×105 (1.6x104 - 2.8x105) | ANOVA | <0.0001 | |
| Ctrl 1: 2B4.ζ CARNK | 5.9×105 (4.3x105 - 8.4x105) | ||||||
| Ctrl 2: NT-NK | 7.3×106 (4x106 - 1.6x107) | <0.0001 | |||||
| Dong et al. 2022 [ | OCI-AML3 | NPM1c-CAR-CIML NK | 10 | 4 | 2 ± 0.6 x108 † | ANOVA | 0.02 |
| Ctrl: NT-NK | 4.3 ± 0.4 x108 † | ||||||
| NPM1c-CARm15-NK | 18 | 4 | 5.3 ± 3.4 x108 † | ANOVA | 0.05 | ||
| Ctrl 1: NPM1c-CAR-NK | 11.2 ± 4.8 x108 † | ||||||
| Ctrl 2: NT-NK | 14.6 ± 7.4 x108 † | 0.05 | |||||
| NPM1c-CARm15-NK | 18 | 4 | 1.3 ± 1.2 x109 † | ANOVA | 0.49 | ||
| Ctrl 1: NPM1c-CAR-T | 1.2 ± 0.6 x109 † | ||||||
| Ctrl 2: NT-NK | 2.8 ± 1.2 x109 † | 0.001 | |||||
| Du et al. 2021 [ | KG1 | NKG2D CAR-NK | 42 | 5 | 1.5×108 (1.4x108 - 1.6x108) | Median ± Range | N.R |
| Ctrl: NT-NK | 2.3×108 (1.9x108 - 2.9x108) | ||||||
| NKG2D CAR/IL15-NK (1 dose) | 17 | 6 | 2.5×103 (1.3x103 - 4.6x103) | N.R | <0.05 " | ||
| NKG2D CAR/IL15-NK (2 doses) | 4 | 2.3×103 (1x103 - 5.4x103) | |||||
| NKG2D CAR/IL15-NK (3 doses) | 4 | 5.1×103 (2.6x103 - 8.8x103) | |||||
| Ctrl 1: NKG2D CAR-NK | 6 | 6.7×105 (4.5x104 - 1.6x106) | |||||
| Ctrl 2: NT-NK | 5 | 2.7×106 (2.4x106 - 3.6x106) | <0.0001 " | ||||
| Mansour et al. 2023 [ | MOLM-13 | FLT3 CAR_CD28/CD3ζ | 12 | 3 | 1.6 ± 0.52 x108 † | ANOVA | N.R |
| Ctrl1: CAR 2B4/CD3ζ | 2.3 ± 0.69 x108 † | ||||||
| Ctrl2: NT-NK-tCD19 | 5.3 ± 3.12 x108 † | <0.01 | |||||
| Morgan et al. 2021 [ | LMA-PDX~ | CD123-CAR-hIL15-NK-92 (1 dose) | 14 | 7 | 39.2 ± 10 %† | Unpaired t-test | n.s |
| Ctrl: NT-NK92 | 4 | 32.9 ± 7.4 %† | |||||
| CD123-CAR-hIL15-NK-92 (2nd dose) | 21 | 7 | 19.8 ± 12.4 %† | Unpaired t-test | 0.05 | ||
| Ctrl: NT-NK92 | 4 | 61.9 ± 11.8 %† | |||||
| Salman et al. 2019 [ | MOLM-13 | CD4-CAR-NK | 9 | 8 | 3.3 ± 2.8 x106 | N.R | < .00001 |
| Ctrl: NT-NK | 0 | ||||||
| Study | Xenograft (cells) | Type of transplanted cells | Survival analysis | ||||
| Treatment - Control | Statistical Test | T | Median (days) | n | p-value | ||
| Caruso et al. 2022 [ | THP-1 | CD123-CAR-NK | Mantel Cox | 100 | >80** | 4 | n.s |
| Ctrl 1: CD123-CAR-T | 60 | 4 | |||||
| Ctrl 2: NT-NK | 40 | 4 | 0.02 | ||||
| CD34+ HSCs | CD123-CAR-NK | Kaplan– Meier | 15 | >15** | 6 | N.R | |
| Ctrl 1: CD123-CAR-T | 5 | 6 | |||||
| Ctrl 2: NT-NK | >15** | 6 | |||||
| Christodoulou et al. 2021 [ | MV-4-11 | CD123-2B4.ζ CAR-NK | Mantel Cox | 80 | 63 | (8-12) | <0.01 |
| Ctrl 1: 4-1BB.ζ CARNK | 56 | (8-12) | |||||
| Ctrl 2: NT-NK | 55 | (8-12) | <0.05 | ||||
| 2B4.ζ/sIL-15 CAR-NK | Mantel Cox | 80 | 26 | (5-7) | <0.001 | ||
| Ctrl 1: 2B4.ζ CARNK | 71 | (5-7) | |||||
| Ctrl 2: NT-NK | 48 | (5-7) | <0.001 | ||||
| MOLM-13 | 2B4.ζ/sIL-15 CAR-NK | Mantel Cox | 30 | 27 | 5 | n.s | |
| Ctrl 1: 2B4.ζ CARNK | 26 | 5 | |||||
| Ctrl 2: NT-NK | 20 | 5 | <0.01 | ||||
| Du et al. 2021 [ | KG1 | NKG2D CAR-NK | Log rank | 55 | 52 | 5 | <0.01 |
| Ctrl: NT-NK | 45 | 5 | |||||
| NKG2D CAR/IL15-NK (1 dose) | Log rank | 100 | 52 | 6 | <0.0001 | ||
| NKG2D CAR/IL15-NK (2 doses) | 67.5 | 4 | |||||
| NKG2D CAR/IL15-NK (3 doses) | >100** | 4 | |||||
| Ctrl 1: NKG2D CAR-NK | 44 | 6 | |||||
| Ctrl 2: NT-NK | 41 | 5 | |||||
| Mansour et al. 2023 [ | MOLM-13 | FLT3 CAR NK-92 | Log rank | 60 | >60** | 5 | <0.01 |
| Ctrl: NT-NK | 37 | ||||||
| FLT3 CAR-sIL15 Off-the-shelf | Log rank | 50 | 45 | 5 | <0.05 | ||
| Ctrl1: sIL-15-NK | 34 | ||||||
| Ctrl2: NK-tCD19 (NT) | 25 | <0.001 | |||||
| AML blast | FLT3 CAR-sIL15 | Log rank | 50 | 43 | 9 | 0.012 | |
| Ctrl2: NT-NK | 30 | ||||||
| Salman et al. 2019 [ | MOLM-13 | CD4-CAR-NK (2 doses) | Mantel Cox | 20 | 20 | 8 | 0.0017 |
| Ctrl: NT-NK | 15 | ||||||
| Zhang et al. 2023 [ | THP1 | CD33/B16 CAR-NK | Kaplan– Meier | 60 | >60** | 4 | N.R |
| Ctrl 1: CD33 CAR-NK | 37 | ||||||
| Ctrl 2: NT-NK | 27 | ||||||
| Study | Xenograft (cells) | Type of transplanted cells | Leukemic burden | |||||||
| Treatment - Control | Tt | n | Bone Marrow | Statistical Test | p-value | Spleen | Statistical Test | p-value | ||
| Mean ± SD / (range) | Mean ± SD / (range) | |||||||||
| Albinger et al. 2022 [ | OCI-AML2 | CD33-CAR-NK (1 dose) | 21 | 7 | 0% | Median ± Range | N.R | 0% | Median ± Range | N.R |
| Ctrl: NT-NK | 1.7 (1.4 -1.9%) | 1.5 (0.5-2.7%) | ||||||||
| CD33-CAR-NK (3 doses) | 21 | 7 | 0% | Mann– Whitney | <0.0001 | 0% | Mann– Whitney | <0.0001 | ||
| Ctrl: NT-NK | 6 | 9.3 (6.3 -12.1%) | 5.6 (3.7 -7.6%) | |||||||
| Albinger et al. 2024 [ | OCI-AML2 | CD33-CAR-NK (PROD y SS) | 19 | 9 | 0.3 ± 0.2% | Student’s t test | 0.23 | 0 ± 0.1% | Student’s t test | 0.011 |
| Ctrl 1: CD33-CAR-NK | 9 | 0.1 ± 0.2% | 0% | |||||||
| Ctrl: NT-NK | 7 | 2.9 ± 2% | 0.0012 | 1.4 ± 0.7% | ||||||
| Christodoulou et al. 2021 [ | MV-4-11 | CD123-2B4.ζ CAR-NK | 22 | (8-12) | 58.7% | Mean | N.R | 1.75% | Mean | N.R |
| Ctrl: 4-1BB.ζ CARNK | 74.1% | 12.3% | ||||||||
| Ctrl: NT-NK | 90.8% | 12.8% | ||||||||
| 2B4.ζ/sIL-15 CAR-NK | 22 | (5-7) | 0.1% | Mean | N.R | 3.2% | Mean | N.R | ||
| Ctrl: 2B4.ζ CARNK | 98.2% | 97.7% | ||||||||
| Ctrl: NT-NK | 95% | 98.1% | ||||||||
| Dong et al. 2022 [ | OCI-AML3 | NPM1c-CAR-CIML NK | 10 | 4 | 6.8 ± 3.4 x105 † | ANOVA | 0.06 | 1.4 ± 0.8 x104 † | ANOVA | 0.06 |
| Ctrl: NT-NK | 14.2 ± 3.6 x105 † | 2.6 ± 0.6 x104 † | ||||||||
| NPM1c-CARmb15-NK | 18 | 4 | 5.3 ± 1 x106 † | ANOVA | 0.03 | 1.1 ± 0.4 x105 † | ANOVA | 0.03 | ||
| Ctrl: NPM1c-CAR-NK | 7.6 ± 3.8 x106 † | 2.1 ± 0.2 x105 † | ||||||||
| Ctrl 2: NT-NK | 13.6 ± 6.8 x106 † | 0.2 | 2.7 ± 1 x106 † | 0.34 | ||||||
| Mansour et al. 2023 [ | MOLM-13 | FLT3 CAR-sIL15 Off-the-shelf | 21 | 4 | 0% | ANOVA | n.s | N.R | N.R | N.R |
| Ctrl1: sIL-15-NK | 4.2 ± 1.6% | |||||||||
| Ctrl2: NK-tCD19 (NT) | 40 ± 13% | <0.01 | ||||||||
| Morgan et al. 2021 [ | LMA-PDX~ | CD123-CAR-hIL15-NK-92 (2nd dose) | 21 | 7 | 91.9 ± 6.35% † | Unpaired t-test | n.s | 60.9 ± 14% † | Unpaired t-test | 0.05 |
| Ctrl: NT-NK92 | 4 | 88.6 ± 9.8% † | 88.5 ± 6.4% † | |||||||
| Tang et al. 2018 [ | C: LMA M4 ETO+, C-KIT+ | Pre-treatment | 1M / 4M | 1** | 4% | Mean | N.R | N.R | N.R | N.R |
| Ctrl: Post-treatment | 0 / 76% | |||||||||
| M: LMA M4 t(3;16) | Pre-treatment | 1M | 27% | |||||||
| Ctrl: Post-treatment | 75% | |||||||||
| W: LMA M4 | Pre-treatment | 10 | 37.50% | |||||||
| Ctrl: Post-treatment | 79.50% | |||||||||
| Zhang et al. 2023 [ | THP1 | CD33/B16 CAR-NK | 21 | 4 | 7.7 ± 2.2% | Student’s t test | <0.01 | N.R | N.R | N.R |
| Ctrl 1: CD33 CAR-NK | 39.3 ± 7.2% | |||||||||
| Ctrl 2: NT-NK | 95.7 ± 4.8% | <0.01 | ||||||||
| Study | Xenograft (cells) | Type of transplanted cells | NK cell infiltration | |||||||
| Treatment - Control | Tr | n | Bone Marrow | Statistical test | p-value | Spleen | Statistical test | p-value | ||
| Mean ± SD / (range) | Mean ± SD / (range) | |||||||||
| Albinger et al. 2022 [ | OCI-AML2 | CD33-CAR-NK (1 dose) | 18 | 7 | 0.4 (0.3-0.5%) | Median ± Range | N.R | 0.9 (0.5-1.6%) | Median ± Range | N.R |
| Ctrl: NT-NK | 0% | 0% | ||||||||
| CD33-CAR-NK (3 doses) | 21 | 7 | 1.1 (0.7-1.5%) | Mann– Whitney | < 0.01 | 17.8 (9.8-26.1%) | Mann– Whitney | <0.001 | ||
| Ctrl: NT-NK | 6 | 0.4 (0.3-0.5%) | 2.2 (0.8-3.8%) | |||||||
| Albinger et al. 2024 [ | OCI-AML2 | CD33-CAR-NK (PROD y SS) | 19 | 9 | 0% | Mean± SD | N.R | 0% | Mean± SD | N.R |
| Ctrl 1: CD33-CAR-NK | 9 | 0% | 0% | |||||||
| Ctrl: NT-NK | 7 | 0 ± 0.1% | 0% | |||||||
| Christodoulou et al. 2021 [ | MV-4-11 | CD123-2B4.ζ CAR-NK | 22 | (8-12) | 39.8% | Mean | N.R | 98% | Mean | N.R |
| Ctrl: 4-1BB.ζ CARNK | 24.2% | 87% | ||||||||
| Ctrl: NT-NK | 8.4% | 86% | ||||||||
| 2B4.ζ/sIL-15 CAR-NK | 22 | (5-7) | 99% | Mean | N.R | 99% | Mean | N.R | ||
| Ctrl: 2B4.ζ CARNK | 1.97% | 2.39% | ||||||||
| Ctrl: NT-NK | 4.45% | 1.9% | ||||||||
| Dong et al. 2022 [ | OCI-AML3 | NPM1c-CARmb15-NK | 14 | 4 | 3.1 ± 1% † | ANOVA | 0.03 | 1.1 ± 0.6% † | ANOVA | 0.03 |
| Ctrl: NPM1c-CAR-NK | 0.8 ± 0.2% † | 0.1 ± 0.2% † | ||||||||
| Ctrl 2: NT-NK | 0% | 0% | ||||||||
| Mansour et al. 2023 [ | MOLM-13 | FLT3 CAR-sIL15 Off-the-shelf | 21 | 4 | 14.7 ± 2% | ANOVA | <0.01 | N.R | N.R | N.R |
| Ctrl1: sIL-15-NK | 5.5 ± 2.9% | |||||||||
| Ctrl2: NK-tCD19 (NT) | 0% | <0.001 | ||||||||
| Morgan et al. 2021 [ | LMA-PDX~ | CD123-CAR-hIL15-NK-92 (2nd dose) | 21 | 7 | 0% | Unpaired t-test | n.s | 28.8 ± 17.4% † | Unpaired t-test | 0.05 |
| Ctrl: NT-NK92 | 4 | 0% | 0% | |||||||
| Zhang et al. 2023 [ | THP1 | CD33/B16 CAR-NK | 21 | 4 | 1.7 ± 0.3% | Student’s t test | <0.05 | N.R | N.R | N.R |
| Ctrl 1: CD33 CAR-NK | 0% | |||||||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCAR-T cell therapy research · Immune Cell Function and Interaction · RNA Interference and Gene Delivery
Introduction and background
Acute myeloid leukemia (AML) is a malignant disease that affects hematopoietic stem cells, characterized by uncontrolled proliferation and impaired differentiation of myeloid progenitors [1]. Globally, its incidence and mortality have almost doubled in the past three decades, rising from 63,840 to 119,570 cases between 1990 and 2017 and from 51,770 to 99,900 deaths [2]. These numbers underscore the aggressive course of AML and the biological diversity that makes predicting outcomes and guiding treatment so challenging.
Although most cases appear de novo, AML is influenced by chromosomal rearrangements and acquired mutations [1]. The classical “two-hit hypothesis” proposed by Gilliland [3] distinguishes class I mutations (FLT3, RAS, KIT), which activate proliferative pathways, from class II mutations (NPM1, CEBPA, AML1, PML/RARα), which affect cellular differentiation. Particularly, FLT3-ITD occurs in 30% of patients with a normal karyotype, and NPM1 mutations in approximately 60% [4,5].
Despite advances in molecular and genomic characterization that have driven the development of novel therapies, standard treatment for AML still relies on intensive chemotherapy and/or hematopoietic stem cell transplantation [6]; outcomes, however, remain poor, and five-year survival is particularly low among patients with adverse cytogenetics or those over 60 years of age, with overall survival ranging between 5 and 10% [7,8].
Therefore, the search for more effective therapies has brought attention to chimeric antigen receptor (CAR) T-cell therapy, motivated by its progress in treating refractory hematologic cancers [9,10]. Yet, the application of CAR-T therapy in AML faces multiple limitations, including severe adverse events such as cytokine release syndrome (CRS), negative immunomodulation by the tumor microenvironment, significant immunosuppression associated with pancytopenia, as well as high costs and extensive production times [11-13]. As a result, no CAR-T product has been approved for the treatment of AML.
In this field, CAR-engineered natural killer (CAR-NK) cells are gaining attention. NK cells are members of the innate lymphoid group, and integrate activating and inhibitory receptors such as KIRs, C-type lectins, and natural cytotoxicity molecules to distinguish healthy from malignant cells. Specifically, they recognize human leukocyte antigen (HLA) class I molecules, respond to the absence of MHC-I through the “missing-self” mechanism, detect stress-induced ligands, and mediate tumor lysis via death receptors, antibody-dependent mechanisms, and effector proteins like perforin and granzymes [14,15]. These processes help NK cells to exert powerful antitumor responses while maintaining tolerance to healthy tissues.
The advance from early constructs with CD3ζ signaling to fourth-generation platforms that integrate costimulatory domains (CD28, 4-1BB), cytokine transgenes such as IL-15, safety switches like iCasp9, and more sophisticated regulatory elements has broadened CAR-NKs' applicability, improving their cytotoxicity, expansion, and scalable production [16].
In parallel, allogeneic sources expand the therapeutic landscape, and the most exciting frontier lies in induced pluripotent stem cells (iPSC)-derived NK cells, which are renewable, genetically malleable, and primed for standardized CAR design, they hold promise to overcome many of the bottlenecks that have affected earlier platforms (peripheral blood NKs, NK-92 lines, cord blood cells) such as heterogeneity, limited expansion, loss of persistence for irradiation, and immature phenotypes [16,17].
Encouraging preclinical and early clinical studies in B-cell malignancies, multiple myeloma, and aggressive T-cell leukemias have demonstrated that CAR-NK therapy can provide meaningful antitumor activity with a consistently favorable safety profile related to other adoptive immunotherapies [18,19]. Therefore, the low rate of toxicity, antigen specificity, and feasibility for large-scale manufacturing of CAR-NK cells make them a potentially safer and more accessible therapeutic option for AML [18-20].
Against this backdrop, the present systematic review synthesizes the available clinical and preclinical evidence on CAR-NK therapy in AML, with the aim of providing a basis for future research and facilitating the development of more effective therapeutic strategies.
Methodology
The literature was searched from PubMed and Scopus by taking “AML”, “immunotherapy”, “natural killer cells”, and “chimeric antigen receptor” as keywords. The words were combined with “or” and “and” for joint search. It should search for clinical studies without date restrictions, limited to open-access articles in English or Spanish (Appendix). The last search was performed on April 5, 2024, following the process indicated by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [21].
Eligibility Criteria
Eligible studies included clinical trials of any age or sex, and in vivo preclinical studies using human leukemic cells that evaluated CAR-NK therapy in AML. Studies were required to include a control group of any type and report at least two of the following outcomes: leukemic burden reduction, overall survival, tissue infiltration in bone marrow or spleen, and/or CAR-NK cell persistence. Randomized, quasi-randomized, and non-randomized designs were accepted, provided the full text was available in English or Spanish. Exclusion criteria included in vitro or ex vivo studies, investigations of other cell therapies (e.g., CAR-T, BiKE, TriKE), and studies using alternative methodologies.
Selection Process
The articles retrieved from the databases were organized by publication date. In the first stage, duplicates were removed by matching the year of publication, title, and authors using the Rayyan artificial intelligence platform [22]. The remaining articles were then screened by title and abstract; those that met the predefined eligibility criteria underwent full-text review to assess their relevance in greater detail. All stages of the selection process were carried out by one reviewer.
Data Collection Process
Data from eligible studies were extracted and analyzed using a custom template in Microsoft Excel (v16.0, Redmond, WA, USA). References were managed and documents organized with Zotero (v6.0.36). All stages of screening, extraction, and analysis were performed by a single reviewer.
Risk of Bias Assessment
Risk of bias in preclinical studies was assessed with the Systematic Review Centre for Laboratory Animal Experimentation (SYRCLE) tool [23], which covers 10 domains across six bias categories (selection, performance, detection, attrition, reporting, and other); judgments were recorded as Yes (Y) for low risk, No (N) for high risk, and Unclear (U) when information was insufficient. For clinical studies, methodological quality was appraised using the Joanna Briggs Institute (JBI) tool for quasi-experimental designs [24], comprising nine items spanning internal validity and statistical conclusion validity; a total score above 5 (five) was interpreted as good quality (i.e., lower risk of bias).
Synthesis Methods
Data synthesis was performed in Microsoft Excel (v16.0). For each study, leukemic burden, overall survival, tissue infiltration, and CAR-NK cell persistence were extracted into structured tables (ordered by first author), noting xenograft model, treatment/control cell types, point estimates, and the reported statistical tests with p-values. When numerical values were not provided, data were digitized and estimated from figures using WebPlotDigitizer (v5.2; Automeris, Dublin, CA, USA) [25]. Outcomes were summarized as mean ± SD; if SD could not be obtained, results were presented as median (range); and, when only SEM was reported, SD was derived from the sample size. Log-scaled figures were analyzed on the log scale and back-transformed. A meta-analysis was not performed due to heterogeneity and incomplete reporting of statistical measures in several studies.
Review
Of 322 records identified, 19 were assessed in full text, and 11 met the inclusion criteria (Figure 1). Ten were preclinical mouse xenograft studies using human leukemic cells, two directly comparing CAR-NK with CAR-T [26,27], and one was a phase I clinical trial involving three patients (two adults, one pediatric) [28].
Article retrieval.Process following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [21]. * Duplicates were removed using the Rayyan platform [22].
Most preclinical studies carried a high risk of bias, mainly from absent randomization, blinding, and sample size calculation, although all provided details on animal strain and transplantation methods (Table 1). By contrast, the only clinical study demonstrated good methodological quality, achieving a JBI score of 7 [28].
Characteristics of Cell Models and In Vitro Cytotoxicity
All studies used allogeneic NK cells: 63% from peripheral blood and the remainder from the NK-92 line; only one study used umbilical cord blood (Table 2). All confirmed in vitro cytotoxicity against leukemic cells, with CD33 and CD123 being the most frequently evaluated antigens. All studies used IL-2 for CAR-NK expansion; several also employed feeder cells K562 [31-33] or closed-system expansion platforms (e.g., CliniMACS Prodigy®, Miltenyi Biotec, Bergisch Gladbach, Germany), achieving post-thaw viabilities >80% [30].
Second-generation CARs incorporating 4-1BB or 2B4 domains showed superior cytotoxicity, while the addition of IL-15, whether secreted, membrane-bound, or complexed, enhanced persistence, activation, and effector function [27,31-34]. Cytokine-induced memory-like (CIML) CAR models showed increased cytotoxicity and proliferation [27].
Transduction was primarily viral, with reported efficiencies between 28% and 85% (Table 2). Notably, Du et al. [32] applied a non-viral PiggyBac transposon system, achieving 14% efficiency at day seven, 63% at day 28, and up to 90% by day 49 of culture.
In Vivo Effectiveness
Most studies used NSG mice, while only a few employed humanized models such as NSGS [29,30,34] or IL15-NOG [26]. Xenografts varied in cell type and dose, and only two studies tested primary AML blasts [33,34]. Therapy was administered primarily intravenously, with doses ranging from 1×10⁶ to 1×10⁷ in preclinical models and up to 5×10⁹ in the clinical trial [28].
Bioluminescence (BLI) analyses (Table 3) consistently showed reduced leukemic burden in CAR-NK groups compared to controls, particularly with NPM1c [27], 2B4.ζ [31], NKG2 [32], and CD4 [35] constructs. Nevertheless, progressive disease was observed in all groups, progressing faster without CAR therapy [26-36].
CAR-NK therapy significantly improved overall survival (OS), especially in CD123 [26], FLT3 [33], and bispecific CD33/B16 [36] models (Table 4). Only Christodoulou et al. [31] reported early toxicity and mortality, restricted to MV-4-11 xenografts treated with 2B4.ζ/sIL-15 CAR-NK.
Combination strategies incorporating IL-15 into the CAR construct [27,31-34] generally prolonged survival and produced greater reductions in bioluminescence (Tables 3, 4). Du et al. [32] showed a clear dose-response: two and three infusions of NKG2D-CAR/IL-15 NK cells extended survival to ~60 and ~100 days, respectively, preventing the relapse observed after a single dose. Consistently, Morgan et al. [33] reported a significant further decrease in leukemic burden after a second dose of CD123-CAR/hIL-15 NK cells, an effect not achieved with a single infusion.
Two studies compared CAR-NK with CAR-T [26,27], finding no significant differences in leukemic burden or survival (Tables 3, 4).
Leukemic and NK Infiltration
Control groups exhibited substantially greater leukemic infiltration in bone marrow and spleen (~2-100%) than CAR-treated mice (~0-20%). An exception was Morgan et al. [34], who observed no reduction even after two doses of CD123-hIL15 CAR-NK (Table 5). The largest decreases were achieved with CAR-IL15 constructs [27,33], bispecific CD33/B16 CAR-NK [36], PROD-CAR-NK [30], and with multiple dosing regimens [29]. Dong et al. [27] additionally reported lower hepatic leukemic infiltration with NPM1c-targeted therapy compared to controls (not tabulated).
NK infiltration was consistently higher in CAR-treated groups (Table 6), with ~0-99% positivity in bone marrow and spleen, versus ~0-24% (BM) and ~0-86% (spleen) in controls. Dong et al. [27] also noted greater hepatic infiltration with NPM1c CAR-NK therapy (not tabulated). The highest tissue levels were observed with CD123-2B4ζ CAR-NK ± IL-15 [31] and FLT3 CAR-sIL-15 [33]. Across models, NK presence declined over time [26-36], although repeat dosing improved tissue infiltration [29,34].
In the clinical trial [28], three patients with relapsed/refractory AML (M4) received dose-escalated, irradiated CAR-NK-92 cells after chemotherapy. No objective responses were observed; all patients showed increasing blast counts, which led to treatment discontinuation (Table 5). The pediatric case had the latest relapse (four months) and showed transient molecular improvements (AML1/ETO: 1574→308; WT1: 247→12 per 10,000 ABL). Circulating CAR-NK-92 cells were detectable but short-lived, measuring 4×10² to 2.9×10³ cells/mL in the pediatric patient (days three to eight post-infusion) and 7.6×10² to 2.9×10³ cells/mL in the adult male over the same interval (not tabulated) [28].
Safety and Cytokine Profile
CAR-NK therapy induced increased activation and degranulation markers across models (IFN-γ, MIP-1α, GM-CSF, granulysin, granzymes A/B, sFasL) [26,29,30,34]. Caruso [26] additionally noted upregulation of CD16, CD57, and PD-1 in expanded NK cells, whereas Albinger [29] reported no significant differences from controls.
In preclinical studies, inflammatory cytokines (IL-6, IL-10, TNF-α) remained low [29,30,34]. In contrast, Tang et al. [28] observed transient increases of IL-6, IL-10, and IL-17A after CD33-CAR-NK-92 infusion in patients, resulting in grade I CRS that resolved within 24-48 hours without sequelae, and Morgan et al. [34] reported similar IL-10/IL-17A elevations in CD123-CAR-NK-92-treated mice without any complications. Christodoulou et al. [31] was the only study to describe increased hTNF-α with CD123-CAR-2B4ζ/sIL-15, accompanied by a sustained rise in hIL-15 (from <100 pg/ml at day 14 to >1000 pg/ml at day 28), correlating with early toxicity and mortality.
Safety was otherwise preserved. Mansour et al. [33] reported that FLT3 CAR-sIL-15 NK cells reduced tumor burden without affecting CD34⁺ HSC-derived populations in marrow, blood, liver, or spleen. Similarly, Caruso et al. [26] demonstrated a favorable profile for CD123-CAR-NK cells compared with CAR-T: CAR-T caused endothelial injury, marrow aplasia, and death, whereas CAR-NK maintained 100% survival without hematopoietic or endothelial toxicity.
Discussion
CAR-NK cells are attracting considerable interest as an emerging immunotherapeutic platform for acute myeloid leukemia. Preclinical studies in this review consistently show superior efficacy in eliminating leukemic cells compared to unmodified NKs, and a more proliferative and metabolically active phenotype (Tables 3-6). These properties position CAR-NK therapy as a potentially transformative approach within adoptive cell therapies; however, it is important to note that the high risk of bias reduces the overall strength and reliability of the evidence and should be carefully considered when interpreting these results.
Similarly, clinical translation remains at a very early stage. The single-phase I trial failed to show meaningful efficacy, reflecting the intrinsic limitations of CAR-NK cells, and especially the restricted activity of irradiated NK-92 cells [28,37,38]. This combination of limited clinical data and the high risk of bias in preclinical evidence underscores a central challenge for the field: how to convert promising laboratory advances into durable therapeutic benefit for patients.
Manufacturing and engineering hurdles persist. Gene transfer still relies predominantly on viral vectors, with lentiviral transduction being the most used approach in this review (Table 2); which, while effective, raises concerns about insertional mutagenesis and imposes costly, labor-intensive processes [39-41]. Non-viral platforms (e.g., PiggyBac, Sleeping Beauty) offer scalable, lower-cost alternatives and are beginning to show workable efficiencies in NK engineering, but require further safety validation [32,42,43].
Persistence is equally critical. Several strategies have been explored to prolong CAR-NK survival and function, including cytokine supplementation, feeder cell-based expansion, and the incorporation of constitutive IL-15 into CAR designs. Results, however, are mixed: IL-2, long used to support NK cell growth, is limited by adverse effects (cytokine storm, endothelial cell damage) and T-reg activation [44-47]. IL-15 more effectively sustains proliferation and cytotoxicity, yet its short half-life necessitates continued dosing, raising concerns about systemic toxicity and NK cell exhaustion [47-49]. Meanwhile, modified K562 feeder cells support NK expansion and reduce post-infusion dysfunction, but their malignant origin and the associated risk of contamination demand rigorous (and costly) release testing to ensure clinical safety [50,51].
Therefore, more innovative strategies, including constitutive IL-15 CARs and preactivation with IL-12/15/18 (CIML), are emerging as a new approach given their improved persistence and greater antitumor activity in several models [52-55]. Collectively, studies incorporating combined expansion/persistence strategies demonstrated enhanced cytotoxicity, persistence, and survival benefits in this review (Tables 3-6). Nonetheless, progressive leukemic burden remained a recurring limitation even with CAR-based interventions [26-36], underscoring the need for designs that decouple durability from toxicity and further optimize the activity in disease sites.
Tissue infiltration further complicates the picture, with consistently low persistence of CAR-NK cells in bone marrow and spleen [26-36]. While restricting long-term persistence has been a safety goal, particularly with CAR-T to avoid myeloablation, emerging evidence suggests marrow NK proportions may carry prognostic value in leukemia [56]. Trafficking cues, such as CXCR4 overexpression, represent rational pathways to improve marrow homing and bolster antileukemic effects [57].
Overall, security was favorable in most of the studies analyzed. While the clinical trial reported only mild, self-limited adverse events [28], Christodoulou et al. [31] described significant toxicity and early mortality in mice treated with CD123-sIL15 CAR-NK; although CRS was unlikely due to the absence of murine inflammatory cytokines, this pattern raises concern for alloreactivity or on-target/off-tumor effects, given CD123 expression on endothelial and hematopoietic cells [31,58].
In my view, these adverse outcomes likely reflected a convergence of target selection on healthy tissues, feeder-driven hyperproliferation, and supra-physiologic IL-15 signaling. This interpretation is reinforced by other studies reporting no toxicity when constitutive IL-15 or feeder support is paired with alternative antigens (NKG2D, FLT3) [32,33], and satisfactory tolerance of CD123-CARs without constitutive IL-15 or feeder dependence [26,34].
Despite these obstacles, CAR-NK cells offer distinct advantages: a favorable safety profile with low rates of CRS and no reported neurotoxicity [26-36], CAR-dependent and CAR-independent cytotoxicity [15], a robust cytokine and cytotoxic protein secretion that broaden malignant-cell recognition [26,29,30,34], multiple sources of NK (peripheral blood, umbilical cord blood, or iPSCs), and lower manufacturing cost; enabling standardized, “off-the-shelf” products that improve access and scalability [26,30,33].
Looking ahead, progress will require innovation and smarter solutions that strengthen trafficking and marrow infiltration, improve persistence without undue toxicity, and prevent on-target/off-tumor damage. Emerging tools such as nanobody-based CARs, CRISPR/Cas9 genome editing, bispecific or adapter CARs, and inducible suicide genes represent promising next steps [36,59-62]. But technology alone won’t be enough; impact will also depend on stronger study designs, standardized models, and larger patient cohorts. Only through this combination can CAR-NK therapy move from a promising concept to a reliable therapy in oncology.
As mentioned before, this review has limitations. The risk of bias demonstrated unclear performance in several SYRCLE domains (Table 1), with substantial methodological issues, small sample sizes, and heterogeneity in experimental models, doses, and administration methods; on the clinical side, the available evidence is further constrained by the very limited number of patients studied, which restricts interpretability and weakens the strength of the conclusions.
Conclusions
CAR-NK cells are becoming a promising therapeutic strategy, with features that make them particularly attractive for patients with AML. They may offer a flexible and complementary approach that expands available treatment options; however, the long-term benefits in this regard will depend on addressing key challenges in production and persistence to ensure that initial progress can lead to reproducible and meaningful clinical outcomes. Sustained progress in CAR-NK cell design and manufacturing could help establish this therapy as a viable option for AML, ultimately supporting more personalized care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Genomic classification and prognosis in acute myeloid leukemia N Engl J Med Papaemmanuil E Gerstung M Bullinger L 2209222137420162727656110.1056/NEJ Moa 1516192 PMC 4979995 · doi ↗ · pubmed ↗
- 2The global burden and attributable risk factor analysis of acute myeloid leukemia in 195 countries and territories from 1990 to 2017: estimates based on the global burden of disease study 2017 J Hematol Oncol Yi M Li A Zhou L Chu Q Song Y Wu K 721320203251322710.1186/s 13045-020-00908-z PMC 7282046 · doi ↗ · pubmed ↗
- 3Genetics of myeloid leukemias Annu Rev Genomics Hum Genet Kelly LM Gilliland DG 179198320021219498810.1146/annurev.genom.3.032802.115046 · doi ↗ · pubmed ↗
- 4The importance of FLT 3 mutational analysis in acute myeloid leukemia Leuk Lymphoma Patnaik MM 227322865920182916496510.1080/10428194.2017.1399312 · doi ↗ · pubmed ↗
- 5Cytoplasmic nucleophosmin in acute myelogenous leukemia with a normal karyotype N Engl J Med Falini B Mecucci C Tiacci E 25426635220051565972510.1056/NEJ Moa 041974 · doi ↗ · pubmed ↗
- 6Update on current treatments for adult acute myeloid leukemia: to treat acute myeloid leukemia intensively or non-intensively? That is the question Haematologica Jaramillo S Schlenk RF 34235210820233672240410.3324/haematol.2022.280802 PMC 9890037 · doi ↗ · pubmed ↗
- 7Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European Leukemia Net Blood Döhner H Estey EH Amadori S 45347411520101988049710.1182/blood-2009-07-235358 · doi ↗ · pubmed ↗
- 8Acute myeloid leukemia (AML) SEER relative survival rates by time since diagnosis, 2000-2021 Leukemia 10 2025 Walter RB Othus M Burnett AK 312320292024 https://seer.cancer.gov/statistics-network/explorer/application.html?site=96&data_type=4&graph_type=6&compare By=sex&chk_sex_1=1&chk_sex_3=3&chk_sex_2=2&race=1&age_range=141&hdn_stage=101&advopt_precision=1&advopt_show_ci=on&hdn_view=0&advopt_show_apc=on&advopt_display=2