Diagnostic and management challenges of prune belly syndrome in a low-income country: a neonatal case report
Mohamed Nur Ali, Abdisalam Ismail Hassan, Ali Abdi Jama, Abdisalam Mohamed Sh Abdilahi, Abdisamad Omar Ali, Fardowsa Hassan Ahmed, Yasir Khalif Ali, Farah Ali Ahmed, Farah Abdullahi Ismail, Fardowso Ali Mohamud, Ahmed Mohamed Ali, Ismail Gedi Ibrahim

TL;DR
This case report describes the challenges of diagnosing and managing Prune Belly Syndrome in a low-income country, highlighting the importance of early intervention to protect kidney function.
Contribution
The first documented case of Prune Belly Syndrome in Somalia, emphasizing management in resource-limited settings.
Findings
The neonate showed improved urine output and renal function after percutaneous nephrostomy.
Bilateral ureteropelvic junction obstruction was confirmed as the underlying urinary tract abnormality.
Early surgical intervention was critical in stabilizing the infant's condition.
Abstract
Prune Belly Syndrome (PBS) is a rare congenital anomaly defined by deficient abdominal wall musculature, urinary tract abnormalities, and cryptorchidism. It is associated with high morbidity, particularly in low-resource settings where prenatal imaging and specialized surgical care are limited. We report the first documented case of PBS from Somalia in a 6-day-old male neonate delivered without antenatal care. He presented with abdominal distension, respiratory distress, bilateral undescended testes, and oliguria. Laboratory tests showed impaired renal function and elevated inflammatory markers. Ultrasound revealed multilocular cystic hydronephrosis with thinned renal parenchyma, and a nephrostogram confirmed bilateral ureteropelvic junction obstruction. The infant was managed with oxygen, antibiotics, and bilateral percutaneous nephrostomy, which led to improved urine output,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1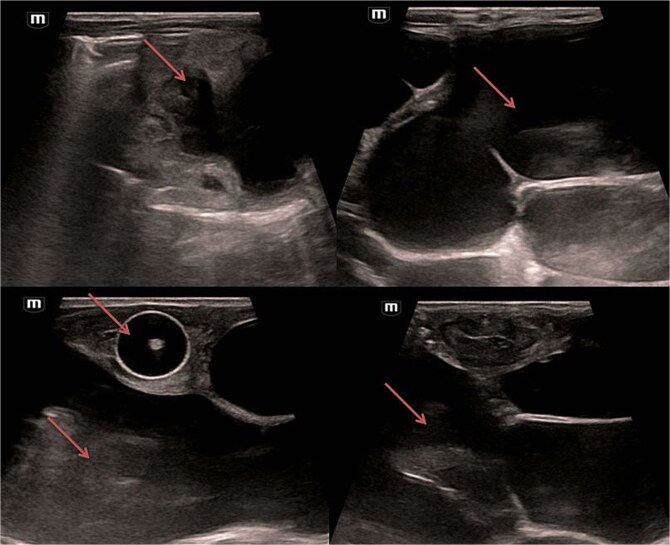 Figure 2
Figure 2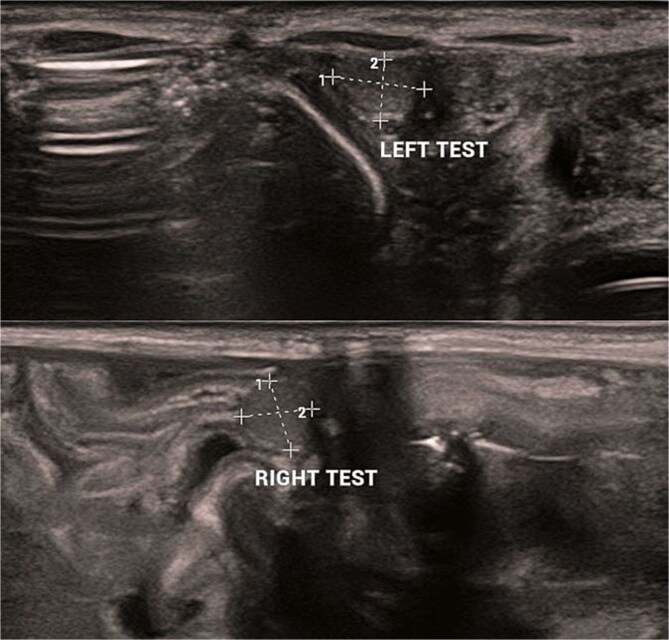 Figure 3
Figure 3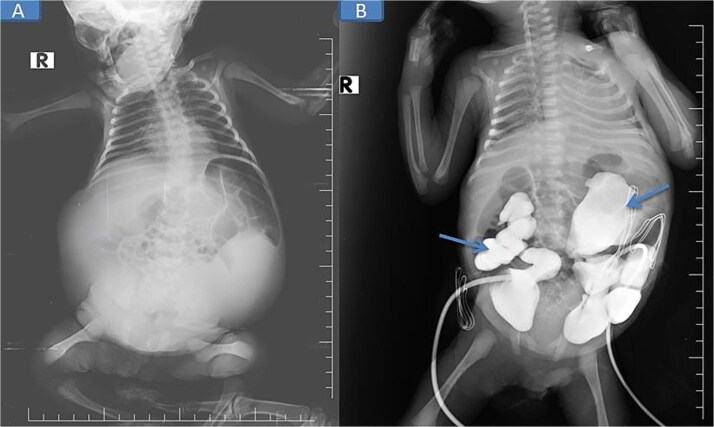 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPediatric Urology and Nephrology Studies · Neonatal Health and Biochemistry · Metabolism and Genetic Disorders
Introduction
Prune Belly Syndrome (PBS), also called Eagle–Barrett or Obrinsky syndrome, is a rare congenital disorder defined by a triad of deficient abdominal wall musculature, urinary tract anomalies, and cryptorchidism [1]. Its etiology remains unclear, though genetic factors have been suggested, including associations with trisomy 21 and chromosome 6q deletions [2]. PBS occurs in ~3.6–3.8 per 100 000 live births, with males comprising 95% of cases [3].
Affected neonates display a characteristic ‘prune-like’ abdomen and may have multisystem involvement—cardiopulmonary (≈49%), musculoskeletal (≈65%), and gastrointestinal (≈63%) anomalies [4]. Prognosis depends on renal function and pulmonary development; perinatal mortality ranges from 10%–25% [4]. Females are rarely affected and generally lack gonadal anomalies [5].
In sub-Saharan Africa, PBS is exceedingly rare, with many pediatricians never encountering a case during their careers [6, 7]. We present a rare documented Somali case of PBS, underscoring the diagnostic and management challenges in a low-resource setting.
Case presentation
A 6-day-old Somali male neonate was delivered through normal vaginal delivery in Cadaado, Somalia, and referred to our hospital for further assessment of insufficient abdominal wall musculature, abdominal distention, low urine output, and respiratory distress. He was lethargic and tachycardic on arrival due to hypoglycemia (blood glucose 37 mg/dl, corrected with 2 mg/kg of 10% dextrose). The mother was 27 years old (gravida 3, para 3) with no medical history, and the pregnancy was not screened by ultrasound or laboratory tests. Family history was negative for congenital disorders.
On examination, the neonate weighed 2.905 kg, measured 45 cm in length, and had a head circumference of 32 cm, all appropriate for gestational age. He was lethargic, in respiratory distress requiring continuous positive airway pressure (CPAP) oxygen support, and had a soft, distended, prune-like abdomen (Fig. 1). The anal canal was patent, and stool passage was normal. Both scrotal sacs were empty.
Pre-nephrostomy drainage abdominal distention (A) and post-nephrostomy (B).
Laboratory results revealed elevated creatinine (1.46 mg/dl), urea (76 mmol/L), and markedly high C-reactive protein (CRP) (142 mg/dl). Human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV) were negative.
Abdominal and scrotal ultrasonography demonstrated multilocular cystic hydronephrosis with thinning of renal parenchyma, extending into the pelvis, and absence of testes within the scrotum. Both testes were located intra-abdominally between bowel loops (left 7 × 4.5 mm, right 6 × 5.5 mm) (Figs 2 and 3). Abdominal X-ray after percutaneous nephrostomy with contrast revealed pooling in both kidneys without ureteric passage, suggesting bilateral ureteropelvic junction obstruction (UPJO) (Fig. 4).
Bilateral multilocular cystic hydronephrosis.
Bilateral cryptorchidism.
Pre-op abdominal X-ray (A) and post-operative percutaneous nephrostomy procedure with contrast injection through the nephrostomy (B).
The patient was stabilized with CPAP oxygen, intravenous antibiotics (ampicillin, cefotaxime, metronidazole), and supportive care. Following preoperative evaluation and parental consent, bilateral nephrostomy was performed, yielding significant urine drainage. Postoperatively, renal function improved with normalization of creatinine and urea, and by Day 5 post-nephrostomy, values had returned to normal (urea 13 mg/dl [reference: 10–45] and creatinine 0.48 mg/dl [reference: 0.35–1.10]), accompanied by a reduction in abdominal distention.
He tolerated breastfeeding well and was discharged after 15 days in good condition, with ongoing outpatient follow-up at the pediatric surgery clinic.
Discussion
PBS affects 3.6–3.8 per 100 000 live births, predominantly males [3, 8]. Its hallmark, a prune-like abdomen, results from absent or hypoplastic abdominal musculature. Cryptorchidism and urinary tract anomalies, including hydronephrosis and UPJO, form the diagnostic triad.
Pathogenesis remains debated. One hypothesis links PBS to mesodermal developmental defects between 6 and 10 weeks’ gestation [10]. Severe obstructive uropathy and urinary ascites may contribute to abdominal wall muscle degeneration and failed testicular descent [9].
Diagnosis is usually antenatal via ultrasound, typically in the second trimester. In this case, absence of antenatal imaging in rural Somalia delayed recognition until postnatal presentation with abdominal distension and renal dysfunction. Postnatal ultrasound and contrast nephrostogram confirmed bilateral UPJO, a key distinguishing feature.
Prognosis depends largely on renal and pulmonary function. Favorable outcomes are seen when at least one kidney functions normally and serum creatinine remains <0.7 mg/dl during childhood [4]. Our patient improved significantly following nephrostomy, normalizing renal function before discharge.
Management requires a multidisciplinary approach: pediatric urologists, nephrologists, pulmonologists, gastroenterologists, and physical therapists coordinate long-term care [11]. In resource-limited settings, this ideal is often constrained by infrastructure and finances. Our case demonstrates that timely decompression of obstructed kidneys via nephrostomy can stabilize critically ill neonates, even when definitive reconstructive urologic surgery is delayed.
Comparison with literature: Previously reported Somali cases described severe jaundice and vesicoureteral reflux managed conservatively due to financial limitations. In contrast, our case was distinguished by confirmed bilateral UPJO treated successfully with nephrostomy, underscoring the importance of individualized management even in constrained environments.
Conclusion
PBS is a rare, life-threatening congenital disorder with high morbidity and mortality. Early antenatal detection and multidisciplinary management optimize outcomes. In resource-limited settings such as Somalia, delayed diagnosis and constrained surgical options pose significant challenges. This case demonstrates that timely supportive care, including nephrostomy, can improve renal function and short-term survival. More research is needed to better understand PBS genetics, optimize management, and improve access to advanced pediatric urology in low-income countries.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alkhawaldeh IM . First Case of Female Prune Belly Syndrome Following In Vitro Fertilization-Induced Pregnancy : A Rare Case Report and Systematic Review of the Literature. 2023.10.1155/2023/5521590 PMC 1070098138073712 · doi ↗ · pubmed ↗
- 2Quilici G, Tolarova MM, Quilici M, et al. Dental treatment of patients with prune belly syndrome. Spec Care Dent 2023;43:67–72. 10.1111/scd.12728 PMC 1008389935526214 · doi ↗ · pubmed ↗
- 3Achour R, Bennour W, Ksibi I, et al. Prune belly syndrome: approaches to its diagnosis and management. Intractable Rare Dis Res 2018;7:271–4. 10.5582/irdr.2018.0109430560020 PMC 6290839 · doi ↗ · pubmed ↗
- 4Papanikolaou GE, Aravanis G, Varvarousis DN, et al. Anatomic and functional reconstruction of the abdominal wall in prune belly syndrome: a case report case presentation. Cureus 2024;16:e 75883. 10.7759/cureus.7588339822405 PMC 11738102 · doi ↗ · pubmed ↗
- 5Lopes RI, Baker LA, Dénes FT. Modern management of and update on prune belly syndrome. J Pediatr Urol 2021;17:548–54. 10.1016/j.jpurol.2021.04.01034016542 PMC 8502198 · doi ↗ · pubmed ↗
- 6Aloni MN, Mujinga V, Tady BM, et al. A first description of prune belly syndrome in Central Africa. Pediatr Neonatol 2015;56:355–6. 10.1016/j.pedneo.2015.01.00625937487 · doi ↗ · pubmed ↗
- 7Hassett S, Smith GHH, Holland AJA. Prune belly syndrome. Pediatr Surg Int 2012;28:219–28. 10.1007/s 00383-011-3046-622198807 · doi ↗ · pubmed ↗
- 8Kazouini I, Chbichib C, Zouita B, et al. A case of prune belly syndrome: radiological aspects of a rare disease. Sch J Med Case Reports 2023;11:1811–6. 10.36347/sjmcr.2023.v 11i 10.023 · doi ↗