Cardiac Medication Prescription Pattern and Association With Transplant-free Survival in the Adult Fontan Population
Andrew M. Freddo, Molly Eron, Antara Mondal, Alexis Z. Tomlinson, Srinivas Denduluri, Sara Partington, Emily Ruckdeschel, Allison L. Tsao, Constantine D. Mavroudis, Muhammad Nuri, Stephanie Fuller, Juan M. Ortega-Legaspi, Yuli Y. Kim, Sumeet Vaikunth

TL;DR
This study examines how medications affect survival in adults with Fontan circulation, finding that loop diuretics are linked to worse outcomes.
Contribution
The study provides one of the first large-scale analyses of medication patterns and survival in adult Fontan patients.
Findings
Loop diuretic prescriptions were associated with significantly worse transplant-free survival.
Antiplatelet agents were the most commonly prescribed medication class.
The study reports detailed medication patterns in a large cohort of adult Fontan patients.
Abstract
There are limited data on the cardiac medications taken by patients with Fontan circulation in adult congenital heart disease (ACHD) clinics. The objectives of the study were to describe the type and frequency of cardiac medications prescribed to adults with Fontan circulation and assess for association between medication prescriptions/burden and transplant-free survival. A retrospective cohort study of adults with Fontan circulation followed in an outpatient ACHD clinic between 2009 and 2023 was performed. Demographics, clinical variables, and all prescribed outpatient cardiac medications were abstracted from the electronic medical record. The outcome of interest was transplant-free survival. Cox proportional hazards analysis was performed to determine the association between the medication type/burden and transplant-free survival. There were 429 patients (55.2% male, 72.5% White,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
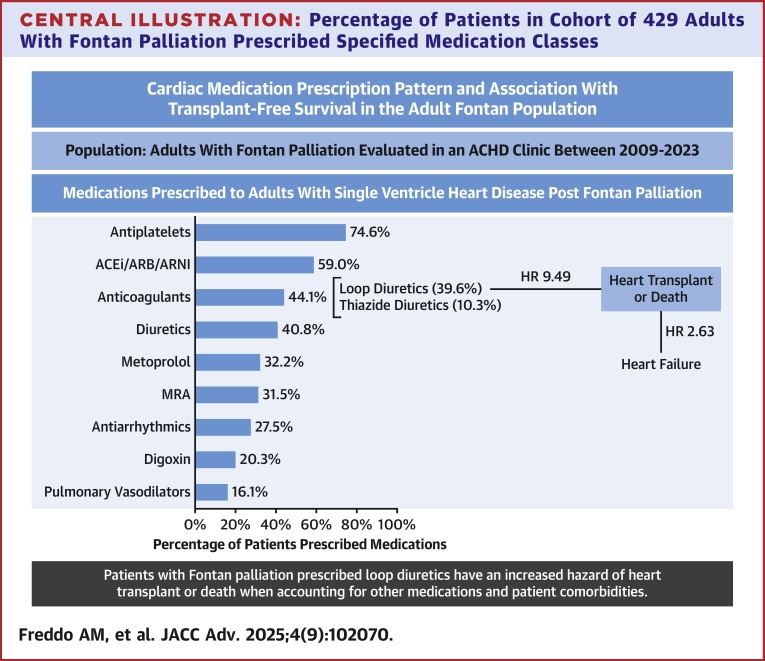 Figure 1
Figure 1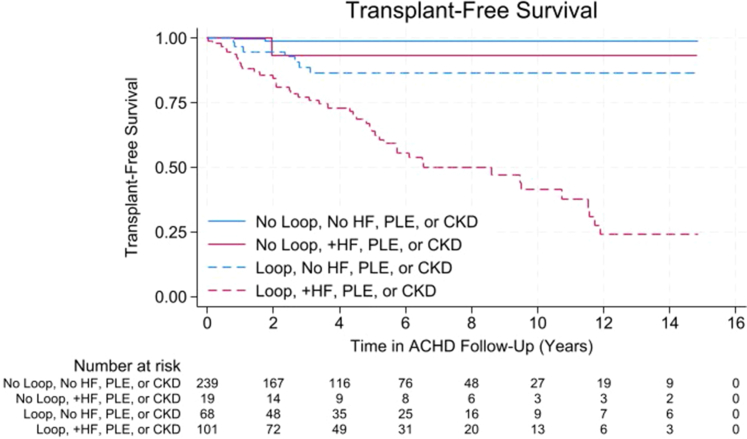 Figure 2
Figure 2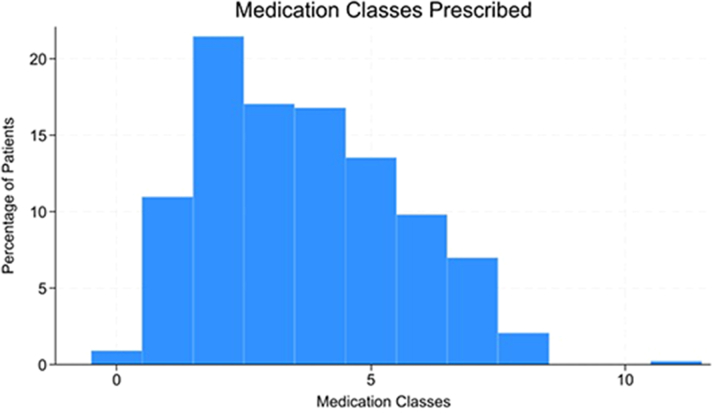 Figure 3
Figure 3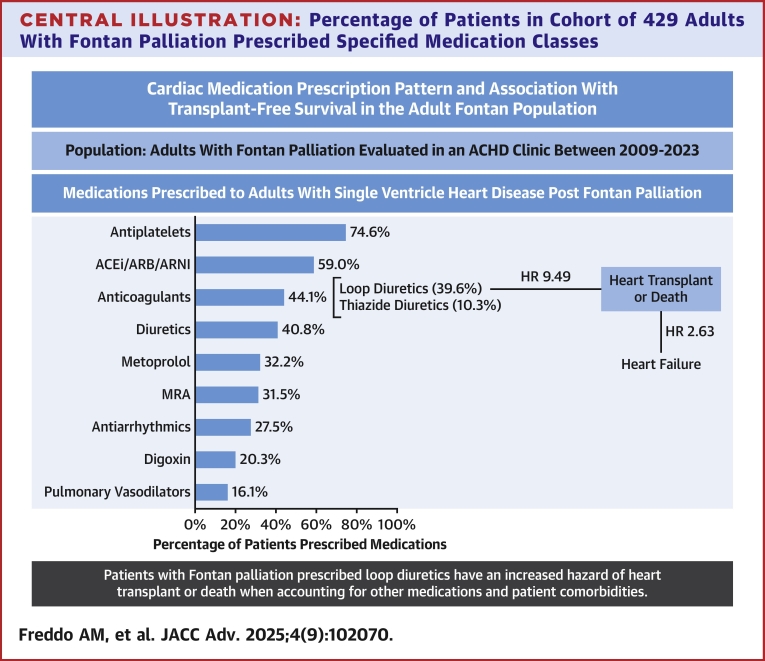 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Cardiac pacing and defibrillation studies · Heart Failure Treatment and Management
Since the advent of the Fontan operation in the late 1960s for tricuspid atresia1 and subsequent modifications thereafter, an increasing number of patients surviving into adulthood are seeking adult congenital heart disease (ACHD) care. Unlike acquired heart disease, for which practice guidelines on medical therapy exist based on high-level evidence, there are limited data-driven guidelines for medical therapy in ACHD. Without these guidelines, it is likely that prescription patterns vary. Previous work has shown large variation in prescription practices in pediatric age patients with Fontan circulation,2 but few studies describe medications in the adult. There also are limitations in the ability to prospectively follow patient response to therapy given the extended timeline for adverse events to occur, heterogeneity of the population, and variations between centers.3 Limited placebo-controlled clinical trials, such as the FUEL (Fontan Udenafil Exercise Longitudinal) and RUBATO trials, have attempted to evaluate the effect of medications on surrogate outcomes, such as measures of oxygen consumption from cardiopulmonary exercise testing, although with mixed results.4^,^5 Medications prescribed can reflect both comorbid conditions as well as illness severity, which predict long-term clinical outcomes. Here we describe medications prescribed to patients with Fontan circulation at our ACHD center and explore the relationship between medication prescriptions and adverse outcomes.
Methods
Data source and study design
A retrospective cohort was identified by searching the electronic medical record (EMR) for adults ≥18 years of age using International Classification of Diseases-Ninth Revision and International Classification of Diseases-10th Revision codes indicating Fontan circulation (Supplemental Table 1) who had at least one office visit encounter in the outpatient ACHD clinic between January 1, 2009, and December 31, 2023. Additional clinical data abstracted from the EMR included demographics, cardiac diagnosis, details of Fontan operation, and cardiac and extracardiac comorbidities. The outcome of interest was transplant-free survival. For cardiac and extracardiac comorbidities, these were noted if listed in the patient's problem list or provider documentation. For arrhythmia, this included bradyarrhythmias (including sinus node dysfunction and high-degree atrioventricular block) and tachyarrhythmias (including atrial and ventricular arrhythmias). This included findings on Holter monitor, when available, and excluded isolated asymptomatic premature atrial or ventricular contractions. For cirrhosis, this included either clinical findings of cirrhosis in ACHD or hepatology documentation and/or imaging findings consistent with cirrhosis. Follow-up was defined as the time from the first clinic visit until either the last confirmed contact in the EMR (up to and including January 31, 2024) or the date of heart transplant or death. This study was approved by the University of Pennsylvania IRB 827550.
Medications
For each patient, medication history (including medication names, start dates, and end dates) was automatically collected. Medications were filtered, and the following categories of medications were removed: noncardiac medications, inpatient medications, and pulmonary vasodilators with an indication for erectile dysfunction. Start and end dates obtained in the initial data collection were verified by chart review, and medications that had a start and end date ≤10 days apart were removed. Medications were collated by generic name and grouped into medication classes and superclasses based on clinical indication. Metoprolol succinate and tartrate were separated from other beta blockers because they could be prescribed for multiple indications (eg, heart failure or arrhythmia). Calcium channel blockers and other beta blockers were separated based on typical indication, antiarrhythmic or not. These classes and superclasses are summarized in Supplemental Table 2. If a patient had a medication class prescribed at any point during their follow-up, they were included in that medication class group. For each patient, total medication burden was defined as the number of superclasses prescribed (as defined in Supplemental Table 2).
Data analysis
Descriptive statistics were reported as frequencies and percentages for categorical variables, and median and IQR for continuous variables. Cox regression was performed to determine if various medication classes were associated with transplant-free survival. Transplant-free survival was defined as no heart transplant or death before the patient's last contact date with our health system. Patients were followed from their first encounter in the ACHD clinic as reported in the EMR to the date of heart transplant or death, whichever came first. Patients who did not experience heart transplant or death were censored at their last contact date with our health system.
Medications prescribed
The independent association between each medication class and transplant-free survival from the first ACHD encounter was initially assessed using univariable Cox proportional hazard models. Medication classes with significant univariable relationships were then analyzed jointly in a multivariable Cox proportional hazard model.
Sensitivity analyses were also performed to assess the potential influence of several confounders on the effect of medication classes that had significant associations in the multivariable model. Confounders were identified as follows: for each medication class, univariable logistic regression was performed to identify whether each potential confounder was significantly associated with the prescription of the medication class. Confounders with significant univariable associations and determined to be clinically relevant to prescription of the medication class were then included in a multivariable logistic model. Significant confounders in the multivariable logistic model were then included in a final multivariable Cox model that included both confounders and medication classes.
Medication burden
The independent association between medication burden and transplant-free survival was assessed using univariable Cox regression. A second sensitivity analysis was performed as described above to assess the potential influence of confounders on medication burden and transplant-free survival.
Statistical analysis was performed using STATA (version 18, StataCorp). The proportional hazards assumption was assessed for all Cox models. Significance for all statistical tests was defined as P < 0.05.
Results
Patient characteristics
The underlying characteristics of the studied cohort is summarized in Table 1 and comorbidities summarized in Table 2 and Supplemental Table 3. Of 429 patients studied, 237 (55.2%) were male and 311 (72.5%) were White. The median age at the patient's first ACHD clinic visit was 24 years old, with an IQR of 22 to 29 years old. Median follow-up time was 3.97 years, with an IQR of 1.58 to 7.14 years. Just under half of patients had single left ventricle morphology (213, 49.7%) and the most common primary diagnosis was tricuspid atresia (114, 26.5%). The most common Fontan type was a lateral tunnel (253, 59.1%).Table 1. Patient Characteristics of Cohort (N = 429)Male237 (55.2)Age at first ACHD visit, y24 [22-29]Follow-up time, y3.97 [1.58-7.14]Race Asian11 (2.6) Black45 (10.5) White311 (72.5) Other18 (4.2) Unknown44 (10.3)Hispanic/Latino ethnicity20 (4.7)Primary cardiac diagnosis Tricuspid atresia114 (26.5) HLHS109 (25.4) DORV59 (13.8) DILV58 (13.5) Unbalanced atrioventricular canal42 (9.8) PA/IVS25 (5.8) Other22 (5.1)Ventricular morphology Single left ventricle213 (49.7) Single right ventricle187 (43.6) Mixed ventricular morphology29 (6.8)Other characteristics Bilateral SVC70 (16.3) Heterotaxy52 (12.1)Fontan type Lateral tunnel253 (59.1) Extracardiac87 (20.3) Aortopulmonary60 (14.0) Other28 (6.5)Fenestrated243 (56.6)Age at Fontan, months29.71 [20.89-52.90]Fontan revision56 (13.1)Fontan completion date 1976-1990114 (26.6) 1991-2000231 (54.0) 2001-201483 (19.4)Values are n (%) or median [IQR].ACHD = adult congenital heart disease; DILV = double-inlet left ventricle; DORV = double-outlet right ventricle; HLHS = hypoplastic left heart syndrome; PA/IVS = pulmonary atresia with intact ventricular septum; SVC = superior vena cava.Table 2. Cardiac and Fontan-Specific ComorbiditiesCardiovascular comorbidities Arrhythmia255 (59.4) Pacemaker/implantable cardioverter Defibrillator107 (24.9) Systolic and/or diastolic heart failure93 (21.7) Stroke/transient ischemic attack85 (19.8) Hypertension46 (10.7) Valve repair19 (4.4) Valve replacement15 (3.5) Pulmonary hypertension15 (3.5) Endocarditis12 (2.8) Hyperlipidemia11 (2.6) Myocardial infarction4 (0.9) Coronary artery disease1 (0.2) No cardiovascular comorbidities112 (26.1)Fontan comorbidities Cyanosis (SpO2 <90%)111 (25.9) Fontan thrombus44 (10.3) Pulmonary arteriovenous malformations35 (8.2) Protein losing enteropathy30 (7.0) Plastic bronchitis1 (0.2) No fontan comorbidities264 (61.5)Values are n (%).
Medications prescribed
The medications prescribed to patients in the cohort are summarized in Table 3. The most prescribed classes were antiplatelets (320 patients, 74.6% of the total cohort), angiotensin-converting enzyme inhibitors (ACEi) (224, 52.2%), loop diuretics (170, 39.6%), metoprolol (138, 32.2%), and mineralocorticoid receptor antagonists (MRA) (135, 31.5%). Certain classes were combined into superclasses of medications: ACEi/angiotensin receptor blocker (ARB)/angiotensin receptor/neprilysin inhibitor (253, 59.0%), anticoagulants, including direct oral anticoagulants (DOAC), heparin analogs, and warfarin (189, 44.1%), diuretic agents, including both loop and thiazide diuretic agents (175, 40.8%), and antiarrhythmics (118, 27.5%).Table 3. Cardiac Medications PrescribedMedication SuperclassN (%)Medication ClassN (%)Medication (Generic)N (%)ACEI/ARB/ARNI253 (59.0)ACEi224 (52.2)Captopril4 (0.9)Enalapril131 (30.5)Lisinopril113 (26.3)Quinapril1 (0.2)Ramipril4 (0.9)ARB46 (10.7)Irbesartan2 (0.5)Losartan42 (9.8)Olmesartan1 (0.2)Telmisartan1 (0.2)Valsartan3 (0.7)ARNI4 (0.9)Sacubitril-valsartan4 (0.9)Anticoagulants189 (44.1)DOAC85 (19.8)Apixaban55 (12.8)Dabigatran6 (1.4)Edoxaban1 (0.2)Rivaroxaban36 (8.4)Heparin analog49 (11.4)Dalteparin1 (0.2)Enoxaparin48 (11.2)Heparin2 (0.5)Warfarin119 (27.7)Warfarin119 (27.7)Diuretics175 (40.8)Loop diuretic170 (39.6)Bumetanide36 (8.4)Furosemide143 (33.3)Torsemide44 (10.3)Thiazide diuretic44 (10.3)Chlorothiazide7 (1.6)Chlorthalidone4 (0.9)Hctz11 (2.6)Indapamide1 (0.2)Metolazone28 (6.5)Other diuretic1 (0.2)Amiloride1 (0.2)Antiarrhythmics118 (27.5)Other antiarrhythmic84 (19.6)Amiodarone30 (7.0)Dofetilide29 (6.8)Flecainide3 (0.7)Mexiletine3 (0.7)Propafenone2 (0.5)Sotalol37 (8.6)Antiarrhythmic beta blocker44 (10.3)Atenolol24 (5.6)Nadolol16 (3.7)Propranolol5 (1.2)Antiarrhythmic calcium channel blocker16 (3.7)Diltiazem14 (3.3)Verapamil3 (0.7)Antiplatelets320 (74.6)Aspirin319 (74.3)Clopidogrel6 (1.4)Ticagrelor1 (0.2)Metoprolol138 (32.2)Metoprolol succinate120 (28.0)Metoprolol tartrate55 (12.8)Mineralocorticoid receptor antagonists135 (31.5)Eplerenone24 (5.6)Spironolactone122 (28.4)Digoxin87 (20.3)Digoxin87 (20.3)Pulmonary vasodilators69 (16.1)Bosentan2 (0.5)Macitentan2 (0.5)Sildenafil53 (12.4)Tadalafil18 (4.2)Treprostinil1 (0.2)Udenafil1 (0.2)Other beta blockers45 (10.5)Bisoprolol2 (0.5)Carvedilol37 (8.6)Labetalol6 (1.4)Pindolol1 (0.2)Statins17 (4.0)Atorvastatin13 (3.0)Lovastatin2 (0.5)Rosuvastatin2 (0.5)Simvastatin3 (0.7)GLP110 (2.3)Dulaglutide2 (0.5)Liraglutide3 (0.7)Semaglutide8 (1.9)Other calcium channel blockers9 (2.1)Amlodipine9 (2.1)Felodipine1 (0.2)SGLT2i8 (1.9)Dapagliflozin3 (0.7)Empagliflozin5 (1.2)Note that some patients were prescribed multiple medications within a class or superclass, and thus the total number of generic prescriptions does not equal the number of patients included in that class.ACEI = angiotensin converting enzyme inhibitors, ARB = angiotensin receptor blockers, ARNI = angiotensin receptor/neprilysin inhibitor, DOAC = direct oral anticoagulant, GLP1 = glucagon-like peptide-1 agonist, SGLT2i = sodium-glucose cotransporter-2 inhibitors.
Medications and outcomes
The outcome of interest, death or transplant, occurred in 55 patients (12.8%). Overall transplant-free survival 5, 10, and 15 years after establishing ACHD care was 88% (84%-91%), 80% (73%-85%), and 66% (52%-76%), respectively.
Univariable analysis showed increased hazard of death or transplant after the first ACHD encounter in patients prescribed loop diuretic agents (HR: 25.81; P < 0.001), MRA (HR: 5.87; P < 0.001), pulmonary vasodilators (HR: 3.31; P < 0.001), anticoagulants (HR: 2.63; P = 0.001), antiarrhythmics (HR: 2.36; P = 0.002), digoxin (HR: 2.30; P = 0.002), and nonantiarrhythmic beta blockers (HR: 2.21; P = 0.013). DOAC prescriptions trended toward decreased hazard of death or transplant (HR: 0.51; P = 0.095) (Table 4).Table 4. Association Between Medication Class Prescribed and Transplant-free Survival From First ACHD EncounterMedication ClassHR95% CIP ValueUnivariable regressions Superclasses MRA5.873.24-10.62<0.001 Pulmonary vasodilator3.311.92-5.71<0.001 Anticoagulant2.631.45-4.770.001 Antiarrhythmic2.361.38-4.020.002 Digoxin2.301.34-3.940.002 Other beta blockers2.211.19-4.120.013 Metoprolol1.430.84-2.430.192 ACEi/ARB/ARNI0.870.51-1.500.617 Classes Loop diuretic25.818.06-82.66<0.001 Warfarin3.411.96-5.92<0.001 Other antiarrhythmic3.031.78-5.16<0.001 Antiarrhythmic beta blockers0.980.44-2.180.967 ACEi0.850.50-1.440.547 ARB0.810.34-1.900.628 DOAC0.510.23-1.120.095Multivariable regression Loop diuretic15.454.43-53.89<0.001 MRA1.540.81-2.950.192 Digoxin1.540.88-2.670.128 Pulmonary vasodilator1.390.79-2.450.247 Other antiarrhythmic1.370.76-2.480.292 Other beta blocker1.020.53-1.960.950 Anticoagulant1.010.53-1.940.972MRA = mineralocorticoid receptor; other abbreviations as in Table 3.
A multivariable Cox regression model was developed to evaluate the relationship between several medications that were independently associated with transplant-free survival (Table 4). In this model, loop diuretic prescription remained significant (HR: 15.45; P < 0.001). To account for patients establishing care at different ages, age at the first ACHD visit was incorporated into the models, which did not significantly change these results (Supplemental Table 4).
To better account for patient characteristics and comorbidities associated with prescription of loop diuretic agents, sensitivity analysis was performed using logistic regression, incorporating clinically appropriate variables significant on univariable regression into the multivariable model (Supplemental Table 5). Factors significantly associated with prescription of loop diuretic agents on multivariable logistic regression were incorporated into the Cox regression multivariable model (Table 5). The association between loop diuretic agents and transplant-free survival remained significant (HR: 9.49; P < 0.001). Systolic and/or diastolic heart failure (HR: 2.63; P = 0.005) was also significant in the final loop diuretic agents model, whereas chronic kidney disease and protein losing enteropathy approached significance (Table 5). Survival curves were generated for patients prescribed loop diuretic agents with and without these comorbidities (Figure 1).Table 5. Association Between Loop Diuretics and DOAC and Transplant-free Survival From First ACHD Encounter Incorporating Patient Characteristics and ComorbiditiesHR95% CIP ValueLoop diuretic agents9.492.69-33.55<0.001Heart failure2.631.33-5.180.005Chronic kidney disease1.770.94-3.310.076PLE1.720.89-3.340.109Cirrhosis1.540.75-3.190.239Cyanosis1.250.72-2.180.435Age at first ACHD visit, y1.0090.979-1.0400.579PLE = protein losing enteropathy; other abbreviations as in Table 1.Figure 1. Transplant-Free Survival for Patients Prescribed Loop Diuretic AgentsTransplant-free survival is decreased in patients prescribed loop diuretic agents (dashed lines) compared with those never prescribed loop diuretic agents (solid lines), even when accounting for presence of heart failure (HF), protein losing enteropathy (PLE), and chronic kidney disease (CKD). Log-rank test P < 0.001. ACHD = adult congenital heart disease.
Medication burden and outcomes
The number of medication classes prescribed to patients throughout their follow-up in ACHD clinic is summarized in Figure 2. It was most common for patients to be prescribed 2 classes of medications.Figure 2. Number of Medication Classes PrescribedHistogram representing number of medication classes prescribed to adult patients with Fontan palliation. Most patients were prescribed 2 medication classes during the follow-up in ACHD clinic
On univariable analysis, there was an association between burden of medications and transplant-free survival (Table 6). Patients prescribed 3 to 4 (HR: 10.20; P = 0.026) or 5 or more medication classes had an increased hazard of transplant or death (HR: 33.22; P = 0.001).Table 6. Association Between Medication Burden and Transplant-Free Survival From First ACHD EncounterMedication Classes PrescribedHR95% CIP Value0-2---3-410.201.32-79.050.0265 or more33.224.57-2420.001Abbreviations as in Table 1.
The logistic regression sensitivity analysis was repeated to identify patient characteristics and comorbidities associated with medication burden (Supplemental Table 6). Factors found to be significantly associated with medication burden were included in a final multivariable Cox model (Table 7). Following adjustment for significant confounders, there was no association between increased mediation burden and transplant-free survival. However, the comorbidities of systolic and/or diastolic heart failure (HR: 6.02, P < 0.001) and cirrhosis (HR: 2.64, P = 0.014) were significant.Table 7. Association Between Medication Classes Prescribed and Transplant-Free Survival Incorporating Patient Characteristics and ComorbiditiesHR95% CIP ValueNumber of medications (reference = 0-2) 3-47.450.92-60.530.060 5 or More7.210.83-62.850.074Race (reference = White) Asian- Black1.620.69-3.800.271 Unknown2.130.74-6.140.161 Other2.930.79-10.900.108Diagnosis (reference = tricuspid atresia) HLHS2.190.98-4.900.057 DORV0.970.39-2.400.946 DILV1.880.77-4.580.167 Unbalanced atrioventricular canal1.510.60-3.780.379 PA/IVS- Other0.820.17-3.850.799Arrhythmia0.760.35-1.630.478Heart failure6.022.74-13.25<0.001Stroke/transient ischemic attack1.110.60-2.040.750Cirrhosis2.641.21-5.760.014Venous thromboembolism1.490.75-2.950.256Diabetes1.510.51-4.460.459Abbreviations as in Table 1.
Discussion
This retrospective study reports one of the first large-scale studies of prescription patterns within the population of adults living with Fontan circulation at a single ACHD center (Central Illustration). We demonstrate a significant negative association between loop diuretic prescriptions and transplant-free survival. When accounting for patient comorbidities, no other medication class showed a significant association with transplant-free survival.Central IllustrationPercentage of Patients in Cohort of 429 Adults With Fontan Palliation Prescribed Specified Medication ClassesOf medications studied, only patients prescribed loop diuretic agents have an increased hazard of heart transplant or death (HR: 9.49; P < 0.001) when accounting for other medications and patient comorbidities. In this model, heart failure also has a significant association with heart transplant or death. ACEi = angiotensin-converting enzyme inhibitor; ACHD = adult congenital heart disease; ARB = angiotensin receptor blocker; ARNI = angiotensin receptor/neprilysin inhibitor; MRA = mineralocorticoid receptor.
In the pediatric Fontan population, there are a limited number of reports describing medication use, including analysis of claims databases and larger single-center studies to determine prevalence of medication use. A large study of claims data from over 4,000 pediatric patients with hypoplastic left heart syndrome or tricuspid atresia6 demonstrated that patients were prescribed fewer medications than in our study; over half of the pediatric population were not prescribed any medications, excluding antiplatelet agents. In that study, the most prescribed medications were ACEi and ARB (38%), diuretic agents (15%) and pulmonary vasodilators (6%); older patients (13-19 years old) were even less likely to be prescribed these medication classes than younger patients.6 This result contrasts with our study, where over 40% of patients were prescribed diuretic agents and over 15% were prescribed pulmonary vasodilators. This is likely in large part due to differences in both overall patient morbidity in the pediatric vs adult population and prescriber practices between pediatric and adult congenital cardiologists.
In addition to the most frequently prescribed medications, it is important to highlight less frequently used medications in this population. Without established guidelines for adults living with congenital heart disease and heart failure, we find a low proportion of patients prescribed more novel heart failure therapies, such as angiotensin receptor/neprilysin inhibitor (4, 0.9%) and sodium-glucose cotransporter-2 inhibitors (8, 1.9%), mainstays of acquired heart failure treatment, despite just over 20% of our population having heart failure. It is possible that these low proportions of patients treated with these more novel therapies is center-specific, although there are limited data about their use in patients living with Fontan circulation, largely case series.7^,^8 Evaluating practices at multiple centers in a prospective fashion could build on this work and provide more insight into how best to use these medications in this patient population.
Medications prescribed and outcomes
There are few studies examining the relationship between medication prescriptions and outcomes in adults with Fontan circulation. In this study, although a cause-and-effect relationship cannot be inferred between medication use and outcomes, the relationship between loop diuretic agents and transplant-free survival supports the concept of the Fontan circulation as one of chronic circulatory failure, which may include systolic or diastolic dysfunction as well as Fontan obstruction, increased pulmonary arterial pressures and/or pulmonary vascular resistance, and/or lymphatic complications.
Although older patients and those with comorbidities such as cirrhosis and protein losing enteropathy are more likely to be prescribed loop diuretic agents, these comorbidities alone do not explain this observed association. Patients who develop congestive symptoms, even without these comorbidities, are likely to be prescribed diuretic agents, which can improve symptoms.9 Uniquely, patients with Fontan failure have increased systemic congestion due to passive systemic venous return and pulmonary blood flow.3^,^10 Diuretic agents are used to alleviate venous congestion and the associated symptoms even in the absence of other comorbidities. This likely represents a sicker patient population with clinically worse prognosis. Conversely, those lacking these symptoms, and as a result who are not prescribed diuretic agents, likely represent a healthier cohort of patients.
We find that patients prescribed medications used to target other results of Fontan circulatory failure, including increased pulmonary vascular resistance (pulmonary vasodilators) and systolic dysfunction (MRA and beta blockers), have a significantly increased risk of transplant or death on univariable analysis. However, these associations do not hold when accounting for multiple medication classes. This suggests that the prescription of loop diuretic agents and presence of congestive symptoms are the most strongly associated with the sickest group of patients living with Fontan circulation when compared with other manifestations of Fontan circulatory failure.
Unlike all other medications studied, the only medication class that trended toward a decreased risk of transplant or death on univariable analysis was DOAC. Patients with Fontan circulation have an increased risk of thromboembolism that confers great morbidity and mortality.11, 12, 13 DOAC have been considered an option for anticoagulation in patients living with Fontan circulation more recently due to studies demonstrating their noninferiority compared with warfarin in adult patients living with Fontan circulation.14^,^15 However, there is still much debate on the efficacy of this class.15^,^16 Our findings may reflect the recent adoption of DOAC medications and the smaller number of patients prescribed them in our cohort. As their use increases and becomes more widespread, it will be important to see if this trend toward increased transplant-free survival persists or if it is attributable to the recent adoption of this medication.
Medication burden and outcomes
We found that increased medication burden (regardless of class) was adversely associated with transplant-free survival on univariable analysis. However, patients who are prescribed more medications also have increased comorbidities, such as heart failure and cirrhosis (Supplemental Table 6), compared with those prescribed fewer medication classes. These comorbidities were significantly associated with transplant-free survival on multivariable analysis, whereas the number of medication classes prescribed was not. This emphasizes the importance of controlling for patient characteristics and comorbidities that may be associated with prescription practices.
Study Limitations
This study is limited by being retrospective in nature. It also was performed at a single quaternary referral center, which may not be generalizable to other practice settings. Because it was performed in an adult-based setting, there is selection bias as only patients who survive to adulthood are included in the study. The justification for why specific patients were prescribed specific medication classes was not captured by this analysis, and medications may be prescribed for multiple indications. We are unable to assess patient adherence to prescribed medications. It also does not speak to what medications may improve patient outcomes. Although many clinical variables were captured, there is the potential for additional, unmeasured confounders. A significant association between medications prescribed and outcomes does not imply causality. Several models and associations were investigated without P value adjustment for multiple comparisons. For this reason, our findings, including CIs, should be interpreted with caution and serve as motivation for future refined questions. Nevertheless, this important work will inform future retrospective cohort studies, as well as prospective studies, in improving treatment for patients living with ACHD.
Conclusions
This is one of the first large-scale studies of medications prescribed in adults living with Fontan circulation. The most common medications prescribed were antiplatelet agents, ACEi/ARB, anticoagulants, antiarrhythmics, and diuretic agents. Loop diuretic agents had the strongest association with transplant-free survival. Patients prescribed loop diuretic agents had significantly worse transplant-free survival, with and without adjustment for patient comorbidities.PerspectivesCOMPETENCY IN MEDICAL KNOWLEDGE: Adult patients living with Fontan circulation are treated with a wide variety of cardiac medications; of these, loop diuretic agents has the strongest association with decreased transplant-free survival.TRANSLATIONAL OUTLOOK: This study can inform future prospective studies to determine changes in laboratory or clinical testing after therapy initiation as well as form the basis for guideline-directed therapy for patients with Fontan circulation.
Funding support and author disclosures
This study was funded by Matthew Hearts of Hope Foundation. This work was supported in part by the Cardiac Center Clinical Research Core at the Children’s Hospital of Philadelphia. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fontan F.Baudet E.Surgical repair of tricuspid atresia Thorax 261971240508948910.1136/thx.26.3.240PMC 1019078 · doi ↗ · pubmed ↗
- 2Anderson P.A.W.Breitbart R.E.Mc Crindle B.W.The Fontan patient: inconsistencies in medication therapy across seven pediatric heart network centers Pediatr Cardiol 312010121912282093865510.1007/s 00246-010-9807-5PMC 3050513 · doi ↗ · pubmed ↗
- 3Rychik J.Atz A.M.Celermajer D.S.Evaluation and management of the child and adult with Fontan circulation: a scientific statement from the American Heart Association Circulation 1402019 e 234e 2843125663610.1161/CIR.0000000000000696 · doi ↗ · pubmed ↗
- 4Goldberg D.J.Zak V.Goldstein B.H.Results of the Fontan udenafil exercise longitudinal (FUEL) trial Circulation 1412019641651
- 5Clift P.Berger F.Sondergaard L.The efficacy and safety of macitentan in Fontan-palliated patients: results of the 52-week randomised, placebo-controlled RUBATO trial Eur Heart J 432022 ehac 544.156010.1016/j.jtcvs.2024.08.03939216715 · doi ↗ · pubmed ↗
- 6O'Byrne M.L.Faerber J.A.Katcoff H.Prevalent pharmacotherapy of US Fontan survivors: a study utilizing data from the Market Scan Commercial and Medicaid claims databases Am Hear J 243202215816610.1016/j.ahj.2021.09.012PMC 881962534582777 · doi ↗ · pubmed ↗
- 7Yan L.Loh J.K.Tan J.L.Sacubitril/valsartan for heart failure in patients with complex adult congenital heart disease – experience from a tertiary centre in Singapore Int J Cardiol Congenit Hear Dis 62021100268
- 8Muneuchi J.Sugitani Y.Kobayashi M.Ezaki H.Yamada H.Watanabe M.Feasibility and safety of sodium glucose cotransporter-2 inhibitors in adults with heart failure after the Fontan procedure Case Rep Cardiol 20222022524359410.1155/2022/5243594 PMC 975793436530388 · doi ↗ · pubmed ↗