Assessing Morbidity and Malignancy Risk in Patients Presenting with Pulmonary Embolism in an Ambulatory Care Setting
Muhammed Memon, Eram Anwar, Kamran Shakir, Chafik Bouhaddioui, Mueed Akram, Shakeel Awan, Muhammad Khalil, Muhammad Usama, Adnan Agha

TL;DR
This study evaluates the risk of morbidity, mortality, and new cancer diagnoses in patients with pulmonary embolism managed in an outpatient setting.
Contribution
The study introduces a classification tree method to predict new cancer sites with high specificity using age and cancer history.
Findings
High sPESI scores correlate with increased 90-day mortality in pulmonary embolism patients.
A classification tree model predicted new cancer sites with 97% specificity using age and cancer history.
Unprovoked pulmonary embolism was observed in 52.4% of patients.
Abstract
Venous thromboembolism (VTE), especially pulmonary embolism (PE), can be treated in an outpatient setting after appropriate risk assessment. However, front-door physicians may be resistant to follow this practice. The possibility of cancer-associated VTE complicates the outpatient management of PE. This study aimed to assess the morbidity and mortality in patients with PE who were managed in an emergency/acute medicine-led outpatient clinic as per risk stratification as well as detecting diagnoses of new cancer sites (NCSs) in these patients. This retrospective study included all patients with confirmed PE managed in an acute medicine outpatient setting at Queens Hospital, Burton-on-Trent, United Kingdom, from 2019 to 2022. Biochemical findings, radiological findings, mortality and morbidity rates, treatment administered, simplified Pulmonary Embolism Severity Index (sPESI) scores,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
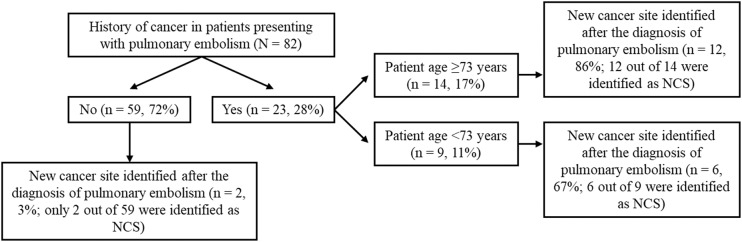 Fig. 1
Fig. 1| Data | Mean ± SD or n (%) |
|---|---|
| Age in years | 63.3 ± 16.7 |
| Male sex | 46 (56.1) |
| Heart rate in beats/min | 88.4 ± 15.9 |
| Blood pressure systolic in mmHg | 145.3 ± 20.7 |
| Blood pressure diastolic in mmHg | 84.7 ± 12.9 |
| Respiratory rate in breaths/min | 17.8 ± 1.7 |
| Oxygen saturation in % | 97.0 ± 1.9 |
| Body mass index | 31.7 ± 9.6 |
| Weight in kg | 94.9 ± 30.1 |
| White blood cells × 109/L | 8.9 ± 3.7 |
| Neutrophils × 109/L | 6.2 ± 3.1 |
| Electrocardiogram changes present | 17 (20.8) |
| Creatinine in μmol/L | 81.9 ± 18.7 |
| Glomerular filtration rate in mL/min | 78.2 ± 21.7 |
| Wells score ≤4 (2-tier) | Unlikely PE = 60 (73.2) |
| Wells score ≤2 (3-tier) | Low risk PE = 43 (52.4) |
| Unprovoked pulmonary embolism | 43 (52.4) |
| D-dimer level raised | 62 (75.6) |
| D-dimer level not raised/normal | 5 (6.1) |
| Characteristic | Present, n (%) |
|---|---|
| History of cancer | 23 (28) |
| Previous venous thromboembolism | 7 (8.5) |
| High body mass index ≥30 kg/m2 | 5 (6.1) |
| Presence of diabetes, hypertension or heart disease | 10 (12.2) |
| Reduced mobility/recent surgery | 5 (6.1) |
| Simplified Pulmonary Embolism Severity Index score ≥1 | 11 (13.4) |
|
| |
| Left | 12 (14.6) |
| Right | 27 (32.9) |
| Bilateral | 43 (52.4) |
|
| |
| Subsegmental | 7 (8.5) |
| Segmental | 34 (41.5) |
| Lobar | 31 (37.8) |
| Main/trunk | 10 (12.2) |
|
| |
| Low molecular weight heparin followed by direct oral anticoagulant | 8 (9.8) |
| Direct oral anticoagulant | 52 (63.4) |
| Low molecular weight heparin | 18 (22) |
| Warfarin with bridging therapy | 4 (4.9) |
| Predictor | Intercept | Estimated slope | |
|---|---|---|---|
| Age | –6.36 | 0.073 | 0.0018 |
| History of cancer (yes) | –3.35 | 3.98 | 0.000 |
| sPESI (low) | –3.807 | 3.887 (Med) | 0.00035 |
| PE class (unprovoked) | –0.36 | –3.375 | 0.0015 |
| Mortality (alive >90 days) | 1.0986 | –2.844 | 0.0012 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management
1. Introduction
Venous thromboembolism (VTE) is a broad term comprising of 2 related diagnoses: deep venous thrombosis (DVT) and pulmonary embolism (PE). VTE affects almost 5% of the population at least once in their lifetime and has shown an increase in the worldwide incidence of approximately 80% in the last decade.^12^ Treating patients with VTE in an inpatient setting can lead to a significant financial burden on the limited healthcare resources. To minimise the cost of VTE related admissions, there has been a push for identifying patients suitable for outpatient treatment of VTE after careful risk stratification at the front door/emergency department (ED).^34^ Although the outpatient treatment for DVT has been successfully utilised in EDs in the USA, similar to the rest of the Western world, with 50% of patients discharged from the ED, the same approach has not been observed in the management of low-risk PE (haemodynamically stable patients with a low 30-day predicted mortality rate) with a discharge from ED to follow-up in outpatient rate of only 10%.^56^ Various clinical tools have been validated to identify low-risk PE with reasonable accuracy, including the Pulmonary Embolism Severity Index (PESI), Hestia criteria and the often used simplified PESI (sPESI).^78^ There is a noticeably higher risk of VTE in patients with cancer than in those without, depending on the site/type of cancer and chemotherapy/hormonal therapy. Life expectancy and quality of life are important considerations when deciding the need for hospitalisation.^910^
The treatment options for PE have become simpler with the availability and safety profile of direct oral anticoagulants (DOACs) which can be utilised as an outpatient treatment option for VTE especially DVT and low-risk PE.^11^ The European Society of Cardiology suggests using PESI or sPESI along with biomarkers and radiological evidence of right ventricular strain in identifying low-risk PE and choosing between outpatient and inpatient management of PE.^12^ However, the treatment of low risk PE in patients with cancer can be more complex. Several systematic reviews and meta-analyses of cancer-associated VTE treatment with DOACs have demonstrated similar efficacy and safety as with vitamin K agonists (VKAs). However, low molecular weight heparin (LMWH) is not only more effective than VKAs in reducing the risk of recurrent VTE in patients with cancer but is also associated with a lower risk of bleeding, especially in gastrointestinal and genitourinary cancers.^1314^ Patients with high risk of PE or ongoing extensive DVT who are unable to use anticoagulation therapy may benefit from inferior vena vein filters as a therapeutic option.^15^ Currently, the VTE guidelines of the American Society of Clinical Oncology propose that physicians should utilise the available clinical risk scores to identify high-risk patients and administer either DOACs or LMWH to haemodynamically stable patients with cancer and VTE.^16^ However, there are no tools to identify the risk of new cancer sites (NCSs) in patients presenting with PE.
This study aimed to assess the outcome of patients suspected of having PE, who were referred via the ED and managed in an outpatient clinic service called same-day medical emergency care (SDMEC) and to assess for complications, such as readmission to the hospital and diagnosis of a NCS after the diagnosis of PE. The secondary objectives were to determine whether PE risk stratification corresponded to the observed morbidity and mortality rates at 30 days and 90 days and to assess the treatment response to an outpatient anticoagulation regimen.
2. Methods
This retrospective study reviewed the medical records of all patients with PE who were initially referred to the SDMEC service via the Accident and Emergency/Acute Medicine Department at Queens Hospital, University Hospitals of Derby and Burton Foundation Trust, Burton-on-Trent, United Kingdom, from 2019 to 2022. All patients who were confirmed to have a diagnosis of PE via computed tomography (CT) pulmonary angiography were discharged within 24 hours of presenting to the ED and completed follow-up in an outpatient SDMEC clinic setting were included in this study. The decision to discharge was based on consultant-led clinical decision regarding suitability for outpatient follow-up and management of each patient. All patients who required oxygen therapy, had ongoing significant chest pain, new reduced mobility/functional status requiring additional support or lacked necessary social support at home were excluded from this study as all these patients were admitted for further inpatient management. The demographic, biochemical and radiological data of the selected patient were collected and reviewed. The main outcomes, including mortality, readmission and morbidity rates at 30 and 90 days, and the risk stratification scores (sPESI) were calculated. Data on treatment administered and complications, such as bleeding, as well as discovery of any NCS diagnosis, were obtained. Patients with evidence of right heart strain, oxygen requirements or decreased mobility were hospitalised and excluded from the study.
Statistical analyses were performed using R (Microsoft Corp., Redmond, Washington, USA), Version 4.3.1 for Windows. Logistic regression analysis (Package MASS) and classification tree method (rpart package) were used in this study to classify patients readmitted within 30 days or died within 90 days. Both methods were used to predict the outcome variable NCS based on different individual independent covariates of the patient.
3. Results
A total of 82 patients with confirmed PE were included in this study. Outpatient management of patients with PE accounted for 67.8% (n = 82/121) of the total patients with PE with 39 patients requiring admission according to clinical needs. The mean age of the included patients was 63.3 ± 16.7 years and 56.1% (n = 46) of the patients were male. Nearly a quarter of these patients (n = 21) presented with new shortness of breath, while 19.5% (n = 16) had pleuritic chest pain; these were the most common symptoms. Tachycardia, a common feature normally seen in PE and is part of PE diagnostic risk assessment, was observed in less than one-third of the patients (n = 22, 26.8%). Unprovoked PE was observed in 52.4% (n = 43) of patients. The calculated Wells score indicated a low risk for PE in 52.4% (n = 43) of patients and the D-dimer level remained normal in 6.1% (n = 5) of patients [Table 1].
Evaluation of various associated features of the patients with confirmed PE showed that 28% (n = 23) had a history for cancer. The risk stratification of the patients based on the sPESI scores was as follows: sPESI score 0 was found in 56.1% (n = 46) patients; sPESI score 1 in 30.5% (n = 25) patients; sPESI score 2 in 10.9% (n = 9) patients; and sPESI score 3 in 2.4% (n = 2) patients [Table 2].
None of the patients with an sPESI score of 0 were readmitted within 30 days or died within 90 days. On the other hand, among 43.9% (n = 36) of patients with an sPESI score ≥1, 16.7% (n = 6) of patients required readmission (2 patients within 30 days and 4 patients within 90 days), while 22.2% (n = 8) of patients died within 90 days. The mortality rate within 90 days was 50% in patients with an sPESI score of 3. The sPESI scores of 1, 2 and 3 were associated with morbidity (NCS diagnosis) in 20% (n = 5/25), 33.3% (n = 3/9) and 100% (n = 2/2) of patients, respectively.
Logistic regression analysis was carried out to determine which variables correlated with prediction of NCS. The outcome variable Y represented the NCS, which was a binary variable with 0 used for those who were not readmitted or died within 90 days and 1 for readmission or mortality within 90 days. Using all covariates, X_i_, i = 1, ..., 10 (25), which are found in Table 2, the estimated logistic regression for the probability of success π (x) = P(Y = 1|X = x) was calculated (estimated) as follows:
where π(x) = P(Y = 1|X = x) and b_i_ are the estimated coefficients for the covariates given in Table 1. Using all variables, the model was not significant. Using individual variables, only the predictors age, history of cancer, sPESI, PE class and mortality were significant [Table 3]. It should be noted that for the variable sPESI, only the medium risk level is significant comparatively to low risk. The other two levels are insignificant.
The refined model with the smallest Akaike information criterion and the largest pseudo-coefficient of determination (pseudoR^2^ = 0.646 was estimated as follows:
where HC indicates history of cancer and the odds ratios are oddsAge = 1.09 and oddsHC= 54.02. A history of cancer was the main factor in predicting the NCS outcome, while age had only a 9% higher risk for every additional year of age. Using the confusion matrix, the accuracy for the presence of NCS was 76.5%, whereas that for its absence was 93.8%.
The classification tree showed that a history of cancer predicted that an NCS would occur in 72% of the patients, of which 97% had NCS and only 3% did not. For the 28% of patients without a history of cancer, the variable ‘age’ helped in categorising the patients into those aged <73 years and ≥73 years. The category of age <73 years predicted that 67% of the patients would not show an NCS, whereas the category of age (≥73 years) predicted that 86% of patients would show an NCS. The classification tree results were similar to those of the logistic regression analysis and gave a threshold for the age where the risk to show an NCS is higher [Fig. 1]. The prediction accuracy of the classification tree was 70.6% and 97% for the presence and absence of an NCS, respectively. Using this classification tree, patients at a high risk of NCS development can be identified and differentiated from those at a low risk. The anticoagulation in patients with NCS was well tolerated with no major bleeding reported, despite 45.5% (n = 5/11) of them having an NCS diagnosis of either gastrointestinal or genitourinary cancer.
Classification tree using age and history of cancer to predict new cancer site(s).NCS = new cancer site.
4. Discussion
This study represents a unique cohort of cancer-associated VTE patients, as 13.4% of the patients had an NCS diagnosis. The classification tree developed in this study identified patients at a high risk of NCS development with a sensitivity of 76%, thus differentiating them from patients who were at low risk of NCS development (specificity = 97%). In addition, high sPESI scores were associated with high morbidity and mortality rates. Compared to the 0% readmission rate and mortality rate of patients with an sPESI of 0, those with an sPESI score >1 showed a 16.7% readmission rate and 22.2% mortality rate within 90 days. Moreover, the incidence of NCS was associated with an increase in the sPESI score. No major bleeding was reported in the current cohort, including in those with cancer-associated VTE, despite nearly half of them having a malignancy associated with higher risk of bleeding like gastrointestinal or genitourinary cancer. The classification tree-based machine learning model is a useful decision-making tool used for identification and validation and can be developed for specific variables/conditions such as for diagnosing malnutrition in cancer patients.^17^
Western guidelines have promoted outpatient management of PE using DOACs in patients identified as low-risk, utilising indices such as sPESI and Hestia criteria along with biomarkers markers/radiological indicators of right ventricular strain. However, there is no consensus on treating cancer-associated VTE in outpatient settings due to the paucity of research evidence because most studies available in the literature include only incidentally discovered PE.^1516^ Almost 25% of patients with VTE may have under-lying cancer-related aetiology and the treatment of cancer-associated VTE is accompanied by a high thrombosis recurrence as well as increased risk of major bleeding and mortality; hence, managing these cases becomes even more challenging.^1819^ A recent observational study on VTE therapy in patients with cancer-associated VTE showed only a slight difference in the incidence of VTE-related adverse events between the home treatment and inpatient treatment groups, with no increase in all-cause mortality in the former at 90 days. Thus, it was considered a suitable option for select patients with cancer-associated VTE.^20^
Investigating cancer in patients with VTE has been debated for decades. A systematic review has suggested that up to 10% of NCSs/malignancies can be identified within 1 year of unprovoked VTE.^21^ However, other recent studies have suggested that imaging, such as CT of the abdomen/pelvis for cancer screening, is neither cost-effective nor beneficial for NCS diagnosis in patients with VTE.^2223^ Notably, the current study's classification tree could help distinguish high-risk patients who should undergo extensive investigations, from low-risk patients who do not benefit from CT screening for cancer in outpatient settings. This classification may be useful for physicians practising emergency medicine, family medicine/general medicine, or ambulatory care/acute medicine. A recent randomised controlled trial showed that low risk PE patients allocated into three different groups (group 1 with active cancer treated at home, group 2 without active cancer treated at home and group 3 with active cancer treated in the hospital) had similar outcomes in terms of current venous thromboembolism, major bleeding and all-cause death.^24^ There was a slightly higher risk of complications in group of patients with active cancer treated at home.^24^
This study was subject to certain limitations. This was a retrospective study which was underpowered with a small sample size of only 82 patients and this hinders the generalisability of the results. Although the sample size is small, this classification tree shows promise for use in clinical practice in outpatient to identify the patients with PE who may have underlying malignancy, and such patients could be offered more extensive cancer screening. Large-scale prospective studies should be conducted to validate the application of the classification tree in clinical practice.
5. Conclusion
This study suggests that patients with confirmed PE can be discharged on the same day via the SDMEC consultant-led outpatient follow-up model. However, an sPESI score >1 can be associated with an increased risk of morbidity, readmission, NCS diagnosis and mortality. A classification tree with the 2 variables (history of cancer and age > 73 years) can be used as a predictive tool to identify patients with newly diagnosed VTE who are at a high risk of NCS development.
Authors' Contribution
Muhammed Memon: Conceptualization, Validation, Resources, Data Curation, Writing - Original Draft, Writing - Review & Editing, Supervision, Project administration. Eram Anwar: Conceptualization, Methodology, Software, Validation, Writing - Original Draft, Writing - Review & Editing, Visualization. Kamran Shakir: Validation, Investigation, Resources, Data Curation, Writing - Original Draft, Writing - Review & Editing, Project administration. Chafik Bouhaddioui: Methodology, Software, Validation, Formal analysis, Writing - Original Draft, Writing - Review & Editing, Visualization. Mueed Akram: Investigation, Resources, Data Curation, Writing - Original Draft, Writing - Review & Editing. Shakeel Awan: Investigation, Resources, Data Curation, Writing - Original Draft, Writing - Review & Editing. Muhammad Khalil: Investigation, Resources, Data Curation, Writing - Original Draft, Writing - Review & Editing. Muhammad Usama: Investigation, Resources, Data Curation, Writing - Original Draft, Writing - Review & Editing. Adnan Agha: Conceptualization, Methodology, Validation, Formal analysis, Investigation, Resources, Data Curation, Writing - Original Draft, Writing - Review & Editing, Visualization, Supervision.
Ethics Statement
United Arab University Human Research and Ethics approval was obtained with United Arab University Human Research and Ethics approval was obtained, Approval reference number ERH_2024_4335. NHS England research and Ethics committee exemption was obtained as it was deemed as retrospective Audit/quality improvement project. Approval from the local hospital Queens Hospital Burton-on-Trent, University Hospitals of Derby and Burton audit committee was obtained (QHB UHDB NHS QIP 2023).
Conflict of Interests
The authors declare no conflicts of interest.
Funding
No funding was received for this study.
Data Availability
Data is available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tagalakis V Patenaude V Kahn SR Suissa S Incidence of and mortality from venous thromboembolism in a real-world population: the Q-VTE Study Cohort. Am J Med 2013; 126:832.e 13–21. https://doi.org/10.1016/j.amjmed.2013.02.024.10.1016/j.amjmed.2013.02.02423830539 · doi ↗ · pubmed ↗
- 2Keller K Hobohm L Ebner M Kresoja KPMünzel T Konstantinides SV Trends in thrombolytic treatment and outcomes of acute pulmonary embolism in Germany. Eur Heart J 2020; 41:522–9. https://doi.org/10.1093/eurheartj/ehz 236.10.1093/eurheartj/ehz 23631102407 · doi ↗ · pubmed ↗
- 3Dalen J Dalen J Unnecessary hospitalizations for pulmonary embolism: impact on US health care costs. Am J Med 2016; 129:899–900. https://doi.org/10.1016/j.amjmed.2016.03.041.10.1016/j.amjmed.2016.03.04127143322 · doi ↗ · pubmed ↗
- 4Fanikos J Rao A Seger AC Carter D Piazza G Goldhaber SZ Hospital costs of acute pulmonary embolism. Am J Med 2013; 126:127–32. https://doi.org/10.1016/j.amjmed.2012.07.025.10.1016/j.amjmed.2012.07.02523331440 · doi ↗ · pubmed ↗
- 5Singer AJ Thode HC Jr Peacock W 4th Admission rates for emergency department patients with venous thromboembolism and estimation of the proportion of low risk pulmonary embolism patients: a US perspective. Clin Exp Emerg Med 2016; 3:126–31. https://doi.org/10.15441/ceem.15.096.10.15441/ceem.15.09627752630 PMC 5065336 · doi ↗ · pubmed ↗
- 6Westafer LM Shieh MS Pekow PS Stefan MS Lindenauer PK Outpatient management of patients following diagnosis of acute pulmonary embolism. Acad Emerg Med 2021; 28:336–45. https://doi.org/10.1111/acem.14181.10.1111/acem.1418133248008 PMC 8221072 · doi ↗ · pubmed ↗
- 7Elias A Mallett S Daoud-Elias M Poggi JN Clarke M Prognostic models in acute pulmonary embolism: a systematic review and meta-analysis. BMJ Open 2016; 6:e 010324. https://doi.org/10.1136/bmjopen-2015-010324.10.1136/bmjopen-2015-01032427130162 PMC 4854007 · doi ↗ · pubmed ↗
- 8Jimenez D Aujesky D Moores L Gomez V Lobo JL Uresandi F Simplification of the pulmonary embolism severity index for prognostication in patients with acute symptomatic pulmonary embolism. Arch Intern Med 2010; 170:1383–9. https://doi.org/10.1001/archinternmed.2010.199.10.1001/archinternmed.2010.19920696966 · doi ↗ · pubmed ↗