Appendicitis with Appendicular Phlegmon Secondary to Endometriosis
Rawan Al Balushi, Maiyan Al Hinai, Shihab Al Maawali, Abdullah Al Qari, Sadiq Al Khaboori

TL;DR
This case report describes a rare instance of appendicitis caused by endometriosis in a 34-year-old woman, highlighting the importance of considering endometriosis in similar cases.
Contribution
The novelty lies in documenting a rare case of appendiceal endometriosis presenting as complicated appendicitis, emphasizing diagnostic challenges and management.
Findings
Appendiceal endometriosis was confirmed via histopathology after initial imaging suggested complicated appendicitis.
The case highlights the need for a high index of suspicion in women of childbearing age to prevent complications.
Prompt surgical intervention is recommended for definitive diagnosis and treatment.
Abstract
Acute appendicitis is a common surgical emergency, however endometriosis in an appendix is a rare phenomenon. In this case report, we describe a 34-year-old woman who visited a teaching hospital on 2024, presenting with typical clinical features of appendicitis. Initial imaging revealed complicated appendicitis with perforation and an appendicolith; following conservative management, the patient was scheduled for an interval appendectomy which revealed an appendicular mass. A repeat surgery was scheduled, where extensive adhesions were noted, resulting in an open appendectomy. Histopathological examination confirmed appendiceal Endometriosis and a follow-up by a gynaecologist was arranged. Appendiceal Endometriosis is a rare phenomenon with variable clinical presentations, a high index of suspicion is necessary for women of childbearing age due to the risk of complications. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1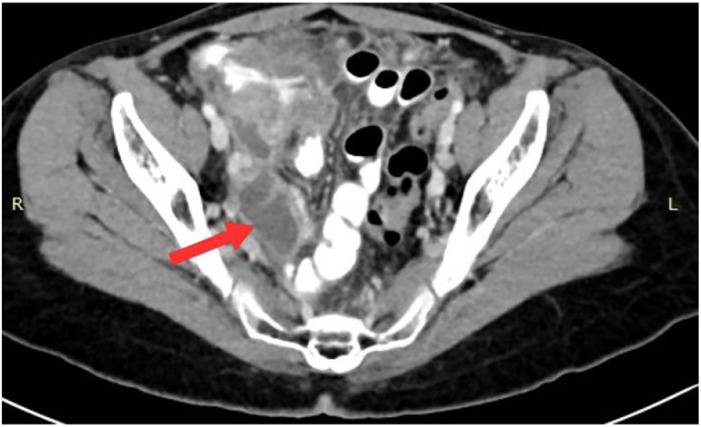 Fig. 2
Fig. 2 Fig. 3
Fig. 3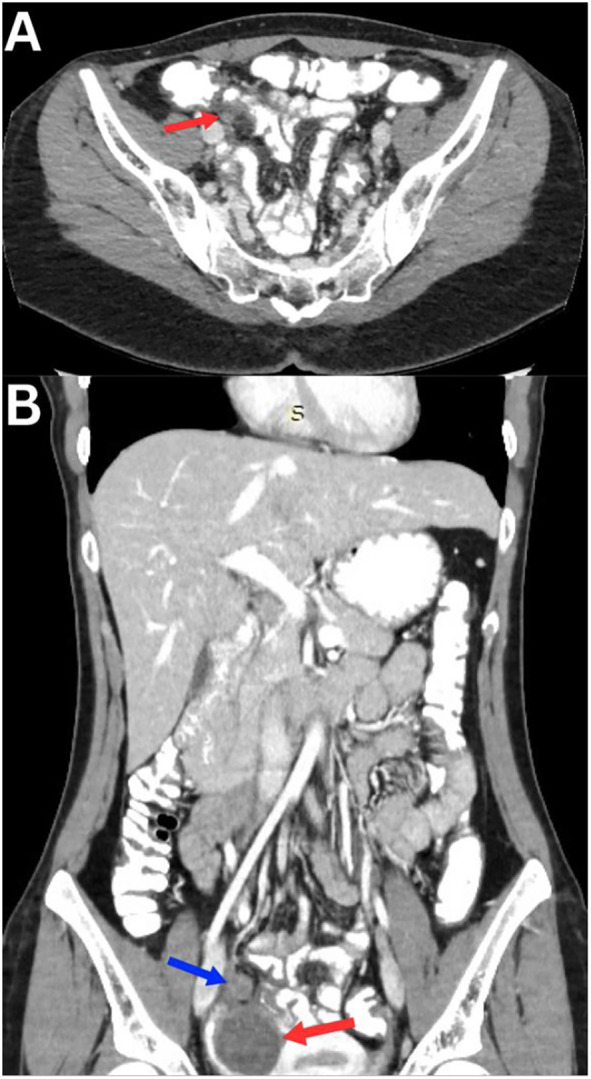 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAppendicitis Diagnosis and Management · Endometriosis Research and Treatment · Intraperitoneal and Appendiceal Malignancies
1. Introduction
Acute appendicitis is a common surgical emergency, diagnosis can be challenging when symptoms deviate from typical presentation.^1^ It is often caused by luminal obstruction (fecaliths, lymphoid hyperplasia, parasites, or neoplasms), leading to increased pressure, bacterial growth, venous congestion, and mucosal ischemia, which may be complicated by perforation. Approximately one-third of cases occur without identifiable obstruction.^2^
Appendicitis is the most common appendiceal disease, with a prevalence of 233 per 100,000 per year and a lifetime risk of 6.7 to 8.6%.^3^ A rare condition that can mimic or complicate appendicitis is the presence of endometriosis in the appendix.^45^ Endometriosis is a chronic, estrogen-dependent inflammatory disease marked by ectopic endometrial-like tissue outside the uterus. It affects 2–10% of reproductive-age women and up to 50% of those with infertility or chronic pelvic pain.^6^ The disease significantly impairs quality of life, with patients experiencing pain, sexual dysfunction, psychological distress, and reduced productivity. Its pathophysiology includes inflammatory, hormonal, and neuropathic components, and it often mimics malignant behavior, requiring multidisciplinary long-term management.^6^ It is typically located within pelvic structures but may involve the gastrointestinal tract, including the appendix contributing to diverse and complex clinical presentations.^567^ The prevalence of appendiceal endometriosis is 0.7% in women undergoing emergency appendectomy for suspected appendicitis.^8^
Appendiceal Endometriosis can present with symptoms similar to acute appendicitis or with severe complications like gastrointestinal bleeding or perforation.^789^ Preoperative diagnosis is challenging due to nonspecific presentation and low prevalence. Most cases are identified only after histopathological examination post-appendectomy.^7^
2. Case report
A 34-year-old female presented with one-week history of periumbilical pain and one day of worsening severe pain, accompanied by vomiting, and intermittent fever visited a teaching hospital in 2024. Earlier that week, she visited her local health institution twice for periumbilical pain and was discharged with analgesia and antibiotics. The patient, on a weekly 2.5 mg dose of Cabergoline for pituitary prolactinoma, had regular menstrual cycles with mild dysmenorrhea. She had no significant family history. Vital signs showed a heart rate of 134 beats per minute, blood pressure of 120/85 mmHg, and a temperature of 37.9°C. Examination revealed dehydration, periumbilical tenderness, and rebound tenderness. Bloodwork showed Haemoglobin (Hb) 11.6 × 10^9^/L, White Blood Cells 13.5 × 10^9^/L, Absolute Neutrophil Count 11.1 × 10^9^/L, and C-reactive protein 344 mg/L.
Pelvic ultrasonography revealed inflammatory changes in the right lower abdomen with echogenic fat and free fluid, but the appendix was not visualised. Computed Tomography (CT) showed fat stranding, fluid in the retrocecal area with 7 and 10 mm appendicoliths, and a localized area of fluid and air (47 × 35 × 50 mm), suggesting sealed perforation [Fig. 1]. Significant caecal and terminal ileum thickening adherent to the inflammatory mass, indicating complicated appendicitis with perforation and mass formation.
Abdominal CT of perforated appendicitis measuring 9.03 mm in diameter.
Admitted under general surgery, the patient received antibiotics for seven days. A follow-up CT one week later showed new pelvic collections [Fig. 2], and an attempted CT-guided aspiration yielded only 4 mL of serous fluid [Fig. 3]. After symptoms resolved and antibiotics were completed, she was discharged. A follow-up CT a month later showed significant improvement, with a slight focus of gas in the appendix (18 × 24 mm) and resolution of pelvic collections. The patient was scheduled for interval laparoscopic appendectomy 9 weeks post initial admission.
Abdominal CT of the appendix measuring 42.74×27.52 mm.
Abdominal CT guided aspiration.
During surgery, haemorrhagic fluid was found in the right lower quadrant, a severely inflamed caecum, and terminal ileum forming a dense inflammatory mass prevented dissection so surgery was abandoned without doing appendectomy. The patient was scheduled for a colonoscopy a week later which appeared to be normal.
Two weeks later, during follow up the patient had no complaints and was scheduled for another follow-up and CT in eight weeks. She presented to the emergency department two weeks before her subsequent follow-up with a three-day history of lower abdominal pain coinciding with her menstrual cycle. Examination showed stable vitals and no significant findings, and she was discharged.
Two weeks later, during follow-up, the patient still complained of lower abdominal pain and was scheduled for CT and laparoscopy possible open appendectomy a month later. The patient was admitted with an active complaint of lower abdominal pain and CT showed decreased inflammatory mass and new bilateral simple adnexal cysts [Fig. 4]. During surgery extensive adhesions were noted between the caecum, terminal ileum, and right ovary. Laparoscopy was converted to open appendectomy due to the appendix being adherent to the caecum, requiring appendectomy with partial caecectomy. Histopathology confirmed multiple foci of Endometriosis. After recovery, the patient was referred to gynaecology for further evaluation.
(A) Abdominal CT showing the inflamed appendix preoperatively (B) Coronal view of an abdominal CT of the inflamed appendix preoperatively (blue arrow) with a large ovarian cyst below it (red arrow).
During her gynaecology visit, the patient had no active complaints. She was scheduled for a Magnetic Resonance Imaging (MRI) pelvis and follow-up three months later.
3. Discussion
Appendicitis is the most common disease of the appendix, with an annual prevalence of 233 per 100,000 and a lifetime incidence of 6.7–8.6%.^3^ It results from luminal obstruction, commonly caused by appendicoliths, lymphoid hyperplasia, or neoplasms.^3^ Rarely, appendicoliths can comprise endometriotic tissue, confirmed only postoperatively via histopathology.^9^ Preoperative detection of appendiceal Endometriosis remains challenging, though detailed histopathological protocols may improve detection rates by 4.6%.^1011^
Endometriosis, an estrogen-dependent chronic inflammatory condition, affects 2–10% of reproductive-age women, typically involving the pelvis but occasionally extending to extrapelvic sites like the appendix.^12^
Mabrouk et al. conducted a comprehensive retrospective analysis of 1,935 patients with histologically confirmed endometriosis undergoing surgical management, identifying Appendiceal endometriosis (AE) in 2.6% of cases.^13^ Although symptoms such as dyschezia, constipation, and right iliac fossa pain were more frequently reported in patients with AE, these did not emerge as independent predictors.^13^
Appendiceal Endometriosis has variable presentations, mimicking classic appendicitis or remaining asymptomatic. Rare complications include caecal intussusception, gastrointestinal perforation, and bleeding.^141516^ In our case, the patient presented with perforated appendicitis, hemorrhagic fluid, and abscesses. Due to intraoperative findings, surgery was initially aborted, and conservative management was pursued. Several weeks later, interval appendectomy with partial caecectomy was performed for adhesions forming a large appendicular mass. Histopathology confirmed endometrial tissue in the appendix, diagnosing appendicitis with Endometriosis.
This case is unique for its combination of abscesses and caecal adhesions. It underscores the importance of considering appendicitis with endometriosis in females presenting with right lower quadrant pain and highlights the need for early intervention to avoid severe complications.
4. Conclusion
This case highlights the importance of recognizing atypical presentation of acute appendicitis, including appendiceal endometriosis. It is crucial to use the entire scope of differential diagnosis when assessing patients with right lower abdomen pain, significantly if the presentation deviates from the typical presentation of appendicitis. Radiological assessment, including MRI, should be considered early, as it provides greater accuracy. Delayed or missed diagnosis causes complications such as perforation, abscess formation, or severe adhesions. That can be avoided with prompt surgical intervention, thorough intra-operative examination of endometriosis deposit and histopathological confirmation.
Authors' Contribution
Rawan Al Balushi: Conceptualization, Resources, Data Curation, Writing - Original Draft. Maiyan Al Hinai: Writing - Original Draft, Resources. Shihab Al Maawali: Writing - Original Draft. Abdullah Al Qari: Resources. Sadiq Al Khaboori: Writing - Review & Editing, Supervision.
Acknowledgement
Would like to acknowledge department of surgery at Sultan Qaboos University Hospital for helping us in managing this Patient.
Conflict of Interest
The authors declare no conflicts of interest.
Ethical Statement
Written consent was obtained from the patient for publication purposes.
Data Availability
Data is available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Siddique M Iqbal P Rajput A Kumar R Atypical presentation of appendicitis: diagnosis and management. J Surg Pak Int 2009; 14(4):157–60.
- 2Akbulut S Dursun P Kocbiyik A Harman A Sevmis S Appendiceal endometriosis presenting as perforated appendicitis: report of a case and review of the literature. Arch Gynecol Obstet 2009; 280:495–7. doi: 10.1007/s 00404-008-0922-y.10.1007/s 00404-008-0922-y 19169700 · doi ↗ · pubmed ↗
- 3Guan L Liu Z Pan G Zhang B Wu Y Gan T The global, regional, and national burden of appendicitis in 204 countries and territories, 1990–2019: A systematic analysis from the Global Burden of Disease Study 2019. BMC Gastroenterol 2023; 23(1):44. doi: 10.1186/s 12876-023-02678-7.10.1186/s 12876-023-02678-736814190 PMC 9945388 · doi ↗ · pubmed ↗
- 4Aragone L Pasquini MT Rebzda VS Talarico MS Mihura M Appendiceal endometriosis: A case report of a rare differential diagnosis of acute appendicitis. Int J Surg Case Rep 2023; 105:107993. doi: 10.1016/j.ijscr.2023.107993.10.1016/j.ijscr.2023.10799336958144 PMC 10053399 · doi ↗ · pubmed ↗
- 5Laskou S Papavramidis TS Cheva A Michalopoulos N Koulouris C Kesisoglou I Acute appendicitis caused by endometriosis: a case report. J Med Case Rep 2011; 5:144. doi: 10.1186/1752-1947-5-144.10.1186/1752-1947-5-14421481248 PMC 3082229 · doi ↗ · pubmed ↗
- 6Raimondo D Raffone A Renzulli F Sanna G Raspollini A Bertoldo L Prevalence and risk factors of central sensitization in women with endometriosis. J Minim Invasive Gynecol 2023; 30(1):73–80. doi:10.1016/j.jmig.2022.10.007.10.1016/j.jmig.2022.10.00736441085 · doi ↗ · pubmed ↗
- 7Gustofson RL Kim N Liu S Stratton P Endometriosis and the appendix: A case series and comprehensive literature review. Fertil Steril 2006; 86(2):298–303. doi: 10.1016/j.fertnstert.2005.12.076. Epub 2006 Jul 7.10.1016/j.fertnstert.2005.12.07616828481 · doi ↗ · pubmed ↗
- 8Schrempf M Kirmair M-A Mair A Hoffmann M Dannecker C Anthuber M Incidence and clinical features of endometriosis in 2484 consecutive female patients undergoing appendectomy for suspected appendicitis: A retrospective analysis. Langenbecks Arch Surg 2024; 409(1):144. doi: 10.1007/s 00423-024-03328-6.10.1007/s 00423-024-03328-638684518 PMC 11059005 · doi ↗ · pubmed ↗