Network Meta-Analysis of Randomized Controlled Trials Comparing Safety and Efficacy of Pharmacological Treatments in Reducing Pain During Intrauterine Device Insertion
Ahmed Ashour, Ahmed H. Saad, Iman Elzahaby

TL;DR
This study compares different medications to reduce pain during intrauterine device insertion, finding lidocaine 4% gel to be the most effective.
Contribution
A network meta-analysis ranks pharmacological treatments for pain reduction during IUD insertion using data from 71 RCTs.
Findings
Lidocaine 4% gel (5 mL) was the most effective for pain relief during IUD insertion (SMD = –4.5).
Lidocaine 4% gel also ranked highest for reducing pain during tenaculum placement.
Misoprostol 400 mcg improved the ease of IUD insertion.
Abstract
Conflicting evidence exists regarding the effectiveness of pharmacological interventions in reducing pain during intrauterine device (IUD) insertion. This study aimed to evaluate the safety and efficacy of various analgesics and to rank their effectiveness. A total of 71 randomized controlled trials (RCTs) involving 10,870 women were included. Data were sourced from PubMed, Cochrane Library, Scopus, and other databases up to September 2023. Analyses were performed using the Netmeta package in R, with results reported as standardized mean differences (SMDs) and risk ratios (RRs), each with corresponding 95% confidence intervals (CIs). Lidocaine 4% gel (5 mL) emerged as the most effective option for pain relief during IUD insertion (SMD = –4.5; 95% CI: –5.9– –3.0; low-quality evidence), followed by lidocaine 1% solution (10 mL; SMD = –3.20). Lidocaine 4% gel also ranked highest for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
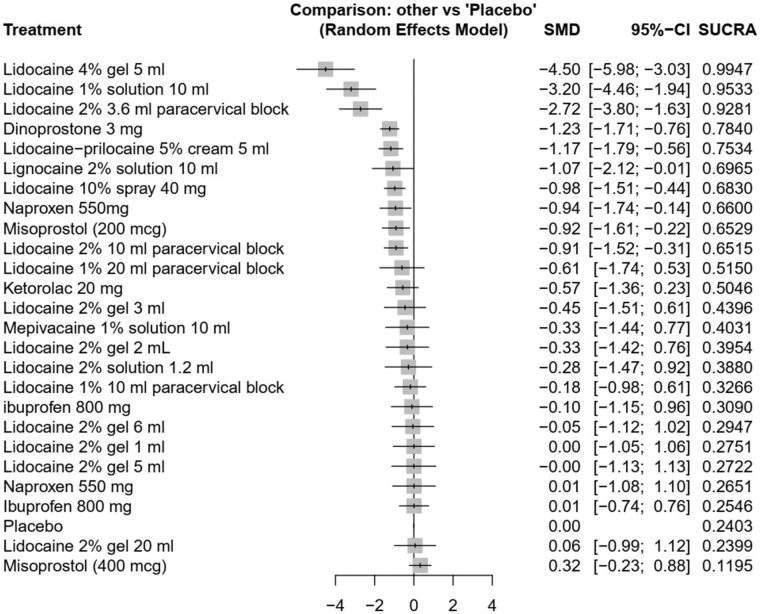 Fig. 1
Fig. 1| Author and Publication year | Groups | Population | Study Design | Sample Size | Type of IUD | Analgesic Type and Dose | Site of Application | Findings | Age, mean ± SD | GRADE assessment |
|---|---|---|---|---|---|---|---|---|---|---|
| Abbas | Analgesic | Parous women | Double-blind RCT | 60 | Copper T380A | Lidocaine-prilocaine 5% cream 5 mL | Cervical canal | The use of cervical LP cream before copper T380A IUD insertion may alleviate the IUD insertion pain among parous women. | 31.1 ± 6.2 | +++° Quality: Moderate - We rated down the quality of evidence (by 1) because of the presence of publication bias. |
| Control | 60 | Placebo | 31.4 ± 6.7 | |||||||
| Hashem | Analgesic | Parous women with no prior vaginal delivery | Double-blind RCT | 70 | LNG IUD | Lidocaine-prilocaine 5% cream 5 mL | Cervical | LP cream and misoprostol could reduce the intensity of pain experienced before, during, and after the insertion of the LNG IUD. | 28.5 ± 6.1 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Analgesic | 70 | Misoprostol (200 mcg) | 27.4 ± 4.5 | |||||||
| Control | 70 | Placebo | 28.5 ± 5.3 | |||||||
| Tavakolian | Analgesic | Nulliparous or multiparous adult women | Triple-blind RCT | 46 | Cooper IUD | Lidocaine-prilocaine 5% cream 5 mL | Cervix and external os | Topical Application of EMLA 5% cream as a topical anesthetic on the cervix before insertion of IUD reduced the pain during this procedure. | 26.8 ± 4.1 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 46 | Placebo | 26.4 ± 4.5 | |||||||
| Maguire | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 100 | Cooper T380A or LNG | Lidocaine 2% gel 1 mL | Intracervical | Intracervical 2% lidocaine gel does not decrease IUD insertion pain. | 27.1 ± 6.0 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 100 | Placebo | 27.6 ± 6.0 | |||||||
| Abbas | Analgesic | Parous women | Double-blind RCT | 50 | Copper T380A | Lidocaine 2% gel 2 mL | Anterior lip (1 mL), cervical canal (1 mL) | The use of lidocaine gel before copper T380A IUD insertion could partially reduce the pain during tenaculum placement and uterine sounding. | 30.58 ± 5.28 | +++° Quality: Moderate - We rated down the quality of evidence (by 1) because of the presence of publication bias. |
| Control | 50 | Placebo | 30 ± 7.76 | |||||||
| McNicholas | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 99 | Cooper T380A or LNG | Lidocaine 2% gel 3 mL | Intracervical | Topical or intracervical 2% lidocaine gel before IUD insertion does not decrease pain scores. | 26–45: 51 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 100 | Placebo | 26–45: 53 | |||||||
| Kazemi | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 31 | Copper T380A | Lidocaine 2% gel 6 mL | Cervical canal | The use of 2% lidocaine gel in the cervical canal does not affect reducing overall pain during IUD insertion. | 29.1 ± 6.7 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 33 | Placebo | 26.7 ± 6.0 | |||||||
| Allen | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 75 | Cooper T380A or LNG | Lidocaine 2% gel 6 mL | 3 mL anterior lip of the cervix, 3 mL cervical canal | Among first-time IUD users, including both nulliparous and multiparous women, 6 mL of 2% lidocaine gel placed on the anterior lip of the cervix and at the internal os for 3 min did not reduce pain with tenaculum placement and IUD insertion compared to placebo gel. | 26.2 ± 5.3 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 75 | Placebo | 25.2 ± 5.0 | |||||||
| Conti | Analgesic | Women 18 years old or older. | Double-blind RCT | 108 | Cooper T380A or LNG | Lidocaine 2% gel 20 mL | Vaginally | Lidocaine gel could not reduce pain during IUD insertion, but it helps with the process of speculum insertion. | 28.9 (18–48) | +°°° Quality: Very low - We rated down the quality of evidence (by 3) because of the presence of risk of bias, the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 107 | Placebo | 27.0 (18–51) | |||||||
| Abd Ellah | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 24 | Copper-T 380A | lidocaine 4% gel 5 mL | Vaginally | Lidocaine dual responsive in situ gel can be effectively used in the prevention of pain during IUD insertion. | - | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 24 | Placebo | - | |||||||
| Tornblom-Paulander | Analgesic | Nulliparous adult women | Double-blind RCT | 108 | Cooper T380A or LNG | Lidocaine 4% gel 8.5 mL | Portio (1 mL), cervical canal (2 mL) and uterine cavity (5.5 mL) | Lidocaine provides pain relief lasting for 30–60 minutes for women undergoing IUD insertion, without any safety concerns. | 23.4 ± 4.1 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 110 | Placebo | 23.9 ± 4.9 | |||||||
| Elsafty | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 100 | Cooper T380A or LNG | Lidocaine 10% spray 20 mg | Cervica | Application of lidocaine spray to the cervix before IUCD insertion was effective in reducing the pain associated with grasping and traction of the cervix with a tenaculum. | 27 (23–32) | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 100 | Placebo | 26 (23–30) | |||||||
| Aksoy | Analgesic | Multiparous women | Double-blind RCT | 100 | Copper T380A | Lidocaine 10% spray 40 mg | Cervical | Significant pain reduction during IUD insertion can be achieved by using 10% lidocaine spray alone. Lidocaine spray can be accepted as a non-invasive, easy, and more comfortable local anesthetic method for IUD insertion. | 30.19 ±7.51 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 100 | Placebo | 29.62 ±7.42 | |||||||
| Hajiesmaello | Analgesic | Multiparous women of reproductive age | Double-blind RCT | 40 | Cooper T380A | Lidocaine 10% spray 40 mg | Cervical | 10% lidocaine spray can be applied as a non-invasive, inexpensive, easy-to-use, and accessible method to decrease IUD insertion pain. | 28.8 ± 7.5 | +°°° Quality: Very low - We rated down the quality of evidence (by 3) because of the presence of risk of bias, the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 40 | Placebo | 30.6 ± 6.8 | |||||||
| Karasu | Analgesic Spray | Multiparous women of reproductive age | Open-label RCT | 51 | Copper T IUD | Lidocaine 10% spray 40 mg | cervical canal and cervix | The three methods were effective in reducing pain during IUD insertion. However, paracervical block is not well tolerated as it is a painful process. | 30.6 ± 7.4 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Analgesic Cream | 53 | Lidocaine 2g cream | 30.2 ± 7.1 | |||||||
| Analgesic injection | 47 | Lidocaine para-cervical block 200 mg | Para-cervical | 28.8 ± 8.2 | ||||||
| Control | 49 | Placebo | cervical canal and cervix | 29.2 ± 7.2 | ||||||
| Panichyawat | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 62 | Cooper T380A | Lidocaine 10% spray 40 mg | Cervical | 10% lidocaine spray was found to be an effective local anesthetic method for reducing pain during the insertion of an IUD. | 31.2 ± 6.7 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 62 | Placebo spray | 30.6 ± 6 | |||||||
| Nelson and Fong, | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 20 | Cooper T380A or LNG | Lidocaine 2% solution 2 mL | Cervical | The use of 2% lidocaine administered through an endometrial aspirator did not significantly reduce IUD insertion pain scores in this pilot study. | 32.06 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 20 | Saline | 32.05 | |||||||
| Elsersy, | Analgesic | Multiparous women | Double-blind RCT | 121 | Cooper T380A | Lignocaine 2% solution 10 mL | Cervical | Intrauterine instillation of 2% lignocaine was useful for pain relief during intrauterine device application. | 30.36 ± 7.64 | +°°° Quality: Very low - We rated down the quality of evidence (by 3) because of the presence of risk of bias, the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 125 | Placebo | 32 ± 7.5 | |||||||
| Envall | Analgesic | Nulliparous women | Double-blind RCT | 41 | LNG IUD | Mepivacaine 1% solution 10 mL | Cervical | Intrauterine mepivacaine instillation before IUD insertion modestly reduces pain, but the effect size may be clinically significant. | 22 (19.5–25.5) | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 40 | Placebo | 22 (20–25.8) | |||||||
| Cirik | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 34 | Cooper T | Lidocaine 1% 10 mL paracervical block | Para-cervical | Paracervical block is an easy, safe, and effective way of pain control during intrauterine device insertion. | 28.5 (19–42) | +°°° Quality: Very low - We rated down the quality of evidence (by 3) because of the presence of risk of bias, the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 30 | Placebo | 27 (20–43) | |||||||
| Fahmy | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 50 | Cooper T380A | Lidocaine 1% 10 mL paracervical block | Para-cervical | 1% lidocaine paracervical block, as well as NSAIDs, before IUD insertion does not decrease pain scores. | 27 ± 4.3 | +°°° Quality: Very low - We rated down the quality of evidence (by 3) because of the presence of risk of bias, the wide confidence interval (Imprecision), and the presence of publication bias. |
| Analgesic | 50 | Naproxen 550 mg | 27.4 ± 4.8 | |||||||
| Control | 50 | Placebo | 28.9 ± 3.9 | |||||||
| Mody | Analgesic | Nulliparous or multiparous adult women | Open-label RCT | 26 | Cooper T380A or LNG | Lidocaine 1% 10 mL paracervical block | Para-cervical | Compared with no anesthetic, a 1% lidocaine paracervical block did not result in a statistically significant decrease in perceived pain with IUD insertion. | 31.9 ± 5.9 | +°°° Quality: Very low - We rated down the quality of evidence (by 3) because of the presence of risk of bias, the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 24 | Placebo | 33.2 ± 6.2 | |||||||
| Mody | Analgesic | Nulliparous adult women of reproductive age | Single-blinded RCT | 33 | Cooper T380A or LNG | Lidocaine 1% 20 mL paracervical block | Para-cervical | Lidocaine paracervical block could decrease pain with IUD insertion. Although the process is painful, the perception of IUD insertion pain was lower compared to placebo. | 26.1 ± 3.9 | +°°° Quality: Very low - We rated down the quality of evidence (by 3) because of the presence of risk of bias, the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 31 | Placebo | 24.8 ± 3.4 | |||||||
| De Nadai | Analgesic | Nulliparous adult women | Double-blind RCT | 99 | LNG IUD | Lidocaine 2% 3.6 mL paracervical block | Para-cervical | A 3.6 mL 2% lidocaine intracervical block decreased pain at tenaculum placement and levonorgestrel-releasing intrauterine system insertion among nulligravidas. | 25 ± 4 | +++° Quality: Moderate - We rated down the quality of evidence (by 1) because of the presence of publication bias. |
| Control | 101 | Intracervical dry-needling | 24.7 ± 4.5 | |||||||
| Control | 102 | Placebo | 25 ± 4.2 | |||||||
| Dogan and Simsek, | Analgesic | Multiparous women | Double-blind RCT | 42 | Cooper T380A | Lidocaine 2% 10 mL paracervical block | Para-cervical | Paracervical block was an effective method for pain relief during copper IUD insertion. | 33.1 ± 7.3 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the presence of risk of bias, and the presence of publication bias. |
| Control | 46 | Placebo | 33 ± 8.3 |
| Author and Publication year | Groups | Population | Study Design | Sample Size | Type of IUD | Analgesic Type and Dose | Site of Application | Findings | Age, mean ± SD | GRADE assessment |
|---|---|---|---|---|---|---|---|---|---|---|
| Abdellah | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 70 | Copper T380A | Misoprostol (400 mcg) | Vaginally | Misoprostol 400 mcg vaginally before IUD insertion eases and increases the success of insertion with reduction of pain among women who had delivered only by elective CD. | 28 ± 6 | +++° Quality: Moderate - We rated down the quality of evidence (by 1) because of the presence of publication bias. |
| Control | 70 | Placebo | 26.6 ± 4.5 | |||||||
| Dijkhuizen | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 102 | Cooper T380A or LNG | Misoprostol (400 mcg) | Vaginally | The study showed no benefit for the use of misoprostol before IUD insertion. However, there is a tendency to possible harm regarding side effects. Therefore, we would not recommend standard pretreatment with misoprostol. | 31.6 ± 8.6 | +++° Quality: Moderate - We rated down the quality of evidence (by 1) because of the presence of publication bias. |
| Control | 97 | Placebo | 30.7 ± 8.4 | |||||||
| Edelman | Analgesic | Nulliparous adult women | Double-blind RCT | 20 | Cooper T380A or LNG | Misoprostol (400 mcg) | Sublingual | Prophylactic misoprostol before IUD placement in nulliparous women did not reduce patient-perceived pain, but it did appear to increase pre-insertion side effects. | 25 ± 5 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 20 | Placebo | 27 ± 6 | |||||||
| Espey | Analgesic | Nulliparous adult women | Double-blind RCT | 42 | Cooper T380A or LNG | Misoprostol (400 mcg) | Oral | Misoprostol for nulliparous women did not decrease pain or improve the ease of insertion of an IUD. | 24.1 ± 4.3 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 40 | Placebo | 24.1 ± 4.6 | |||||||
| Heikinheimo | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 43 | LNG | Misoprostol (400 mcg) | Sublingual | Sublingual misoprostol did not have a significant effect on the ease of insertion in subjects having a repeat insertion of the LNG-IUD. | 37.6 ± 4.8 | +++° Quality: Moderate - We rated down the quality of evidence (by 1) because of the presence of publication bias. |
| Control | 46 | Placebo | 39.1 ± 4.8 | |||||||
| Lathrop | Analgesic | Nulliparous adult women | Double-blind RCT | 37 | Cooper T380A or LNG | Misoprostol (400 mcg) | Oral | Misoprostol was not helpful for cervical ripening before insertion of IUDs or decreased reported pain for those women. Moreover, it may increase women's pain experience with insertion. | 26 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 36 | Placebo | 25.5 | |||||||
| Radwan, | Analgesic | Adult women with cervical stenosis | Double-blind RCT | 32 | Cooper T380A | Misoprostol (400 mcg) | Vaginally | The administration of vaginal misoprostol and intramuscular diclofenac sodium before IUCD insertion in women with cervical stenosis facilitates the IUCD insertion, decreases failure of insertion, and reduces pain sensation during IUCD insertion. | 26.6 ± 6.1 | +°°° Quality: Very low - We rated down the quality of evidence (by 3) because of the presence of risk of bias, the wide confidence interval (Imprecision), and the presence of publication bias. |
| Analgesic | 32 | Diclofenac sodium 75 mg | Intra-muscular | 26 ± 6.4 | ||||||
| Analgesic | 32 | Misoprostol + Diclofenac | . | 26.4 ± 6.2 | ||||||
| Control | 32 | Placebo | 26.6 ± 4 | |||||||
| Scavuzzi | Analgesic | Nulliparous adult women | Double-blind RCT | 86 | Copper T380A | Misoprostol (400 mcg) | Vaginally | misoprostol may be used before IUD insertion both in nulligravidas and in any woman with cervical stenosis irrespective of parity. | 25.4 + 5.5 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 93 | Placebo | 25.2 + 5.5 | |||||||
| Swenson | Analgesic | Nulliparous adult women | Open-label RCT | 54 | Cooper T380A or LNG | Misoprostol (400 mcg) | Oral or vaginal | Self-administered misoprostol before IUD insertion does not ease IUD insertion or reduce patient-perceived pain in nulliparous women. | 24.6 ± 3.8 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 54 | Placebo | 24.8 ± 4.2 | |||||||
| Bahamondes | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 55 | Cooper T380A or LNG | Misoprostol (200 mcg) | Vaginally | The use of misoprostol before IUC insertion after failure of insertion at the first attempt is significantly better than placebo. | 34.2 + 5.2 | +++° Quality: Moderate - We rated down the quality of evidence (by 1) because of the presence of publication bias. |
| Control | 45 | Placebo | 35.3 + 6 | |||||||
| Mansy, | Analgesic | Parous women with no prior vaginal delivery | Double-blind RCT | 50 | Cooper IUD | Misoprostol (200 mcg) | sublingual | The use of sublingual misoprostol to facilitate IUD insertion in women with tight cervix or in whom vaginal delivery was not experienced, has no role in pain reduction or increase the ease of IUD insertion. | Range: 18–35 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the presence of risk of bias and the presence of publication bias. |
| Control | 50 | Placebo | ||||||||
| Ashour | Analgesic | Nulliparous adult women | Double-blind RCT | 43 | Cooper T380A | Misoprostol (200 mcg) | Vaginally | Vaginal misoprostol or dinoprostone effectively lowered pain during IUD insertion. However, this reduction was only clinically significant in women who received dinoprostone. | 21.2 ± 2.3 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Analgesic | 43 | Dinoprostone 3 mg | 20.9 ± 2.2 | |||||||
| Control | 43 | Placebo | 20.4 ± 1.7 | |||||||
| Ashour | Analgesic | Multiparous women | Double-blind RCT | 80 | Cooper T380A | Dinoprostone 3 mg | Vaginally | Self-administered 3 mg dinoprostone vaginally before copper IUD insertion in parous women reduces pain scores during IUD insertion, making insertion easier and increasing women's satisfaction, with tolerable side effects. | 28.6 ± 4.6 | +++° Quality: Moderate - We rated down the quality of evidence (by 1) because of the presence of publication bias. |
| Control | 80 | Placebo | 29.4 ± 4.5 | |||||||
| Analgesic | Parous women with no prior vaginal delivery | Double-blind RCT | 100 | LNG IUD | Dinoprostone 3 mg | Vaginally | Dinoprostone administration reduced pain during insertion and 30 minutes post-procedure. | 28.8 ± 4.5 | +++° Quality: Moderate - We rated down the quality of evidence (by 1) because of the presence of publication bias. | |
| Control | 100 | Placebo | 28 ± 5.5 | |||||||
| Samy | Analgesic | Nulliparous adult women | Double-blind RCT | 100 | Cooper T380A | Dinoprostone 3 mg | Vaginally | There was no clinically significant difference between the two groups. | 26.6 ± 6.3 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 100 | Placebo | 26.9 ± 6.9 | |||||||
| Samy | Analgesic | Nulliparous adolescents and young women | Double-blind RCT | 65 | LNG IUD | Dinoprostone 3 mg | Vaginally | Dinoprostone reduced pain during insertion and increased women's satisfaction and ease of insertion. | 20.5 ± 1.1 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 65 | Placebo | 20.6 ± 1.1 |
| Author year, and protocol registration number | Groups | Population | Study Design | Sample Size | Type of IUD | Analgesic Type and Dose | Site of Application | Findings | Age, mean ± SD | GRADE assessment |
|---|---|---|---|---|---|---|---|---|---|---|
| Bednarek | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 101 | Cooper T380A | Ibuprofen 800 mg | Oral | Administration of ibuprofen 800 mg before IUD insertion does not reduce pain associated with the procedure for U.S. women. | 27 (18–41) | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 101 | Placebo | 26 (18–44) | |||||||
| Chor | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 44 | LNG | Ibuprofen 800 mg | Oral | Administration of ibuprofen prophylaxis for LNG-IUS insertion does not decrease pain at the time of insertion. | 24.7 ± 5.4 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 37 | Placebo | 27.9 ± 6.5 | |||||||
| Hubacher | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 1010 | Cooper T380A | Ibuprofen 800 mg | Oral | Prophylactic ibuprofen as used in this protocol does not reduce IUD insertion pain. | Range: 18–49 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 1008 | Placebo | ||||||||
| Crawford | Analgesic | Nonpregnant adult women desiring an IUD for contraception | Double-blind RCT | 35 | Cooper T380A or LNG | Ketorolac 20 mg | Oral | Oral ketorolac given 40 to 60 minutes before IUD insertion is effective in reducing pain during IUD deployment, overall pain, and pain 10 minutes after IUD placement. | 31.9 ± 6.7 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 36 | Placebo | 30.7 ± 8.9 | |||||||
| Ngo | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 33 | Cooper T380A or LNG | Ketorolac 20 mg | Intramuscular injection | Ketorolac does not reduce pain with IUD placement but does reduce pain at 5 and 15 minutes after placement. | 26.6 ± 5.1 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 34 | Placebo | 27.3 ± 5.4 | |||||||
| Karabayirli | Analgesic | Multiparous adult women | Double-blind RCT | 34 | Multiload-Cu 375 | Naproxen 550 mg | Oral | Prophylactic analgesia using 50 mg tramadol and 550 mg naproxen, delivered orally, can be used to relieve pain during IUD insertion. | 35 ± 4 | +++° Quality: Moderate - We rated down the quality of evidence (by 1) because of the presence of publication bias. |
| Analgesic | 35 | Tramadol 50 mg capsule | 36 ± 4 | |||||||
| Control | 34 | Placebo | 37 ± 6 | |||||||
| Ngo | Analgesic | Women 18 years or old presenting for insertion of any IUD type available in the clinic | Double-blind RCT | 58 | Cooper T380A or LNG | Naproxen 550 mg | Oral | Oral naproxen sodium does not reduce pain with IUD insertion but does reduce pain after insertion and should be considered as a premedication. | 23.2 ± 3.9 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 60 | Placebo | 24.3 ± 4.2 |
| Author and Publication year | Groups | Population | Study Design | Sample Size | Type of IUD | Analgesic Type and Dose | Site of Application | Findings | Age, mean ± SD | GRADE assessment |
|---|---|---|---|---|---|---|---|---|---|---|
| Rapkin | Analgesic | Nulliparous adult women | Double-blind RCT | 30 | Cooper T380A or LNG | 2% lidocaine gel | Vaginally | For nulliparous women, self-administered vaginal lidocaine gel does not reduce pain with IUD insertion but does decrease pain with tenaculum placement. | 23 (19–25) | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 29 | Placebo | 24 (21–28) | |||||||
| Akers | Analgesic | Nulliparous adolescents and young women | Single-blind RCT | 47 | LNG IUD | Lidocaine 1% 10 mL paracervical block | Para-cervical | A 10-mL 1% lidocaine paracervical nerve block reduces pain during IUD insertion in adolescents and young women. | Range: 18–22; 79% | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the presence of risk of bias and the presence of publication bias. |
| Control | 48 | Placebo | Range: 18–22; 81% | |||||||
| Goldthwaite | Analgesic | Nulliparous or multiparous adult women | Single-blind RCT | 35 | Cooper T380A or LNG | Lidocaine 1% paracervical block | Paracervical Cervical | The mean tenaculum placement pain score was lower in the paracervical block group compared to the lidocaine gel group. However, satisfaction scores were similar. | 34.6 ± 12.2 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Analgesic | 35 | Lidocaine 2% gel | 33.7 ± 7.3 | |||||||
| Castro | Analgesic | Parous women with no prior vaginal delivery | Open parallel-group clinical trial | 50 | LNG IUD | Lidocaine 2% paracervical block | Paracervical | There was no significant difference between lidocaine paracervical injection or oral ibuprofen in terms of pain and discomfort associated with LNG-IUS insertion or the ease of insertion. | 30.4 ± 5.6 | +°°° Quality: Very low - We rated down the quality of evidence (by 3) because of the presence of risk of bias, the wide confidence interval (Imprecision), and the presence of publication bias. |
| Analgesic | 48 | Ibuprofen 400 mg | Oral | 30.6 ± 6.3 | ||||||
| de Oliveira | Analgesic | Nulliparous or multiparous adolescents and young women | Double-blind RCT | 51 | LNG IUD | Lidocaine 2% paracervical block | Paracervical | Lidocaine intracervical block was found to be more effective than naproxen in reducing LNG-IUD insertion pain. | Range: 15–24 | +°°° Quality: Very low - We rated down the quality of evidence (by 3) because of the presence of risk of bias, the wide confidence interval (Imprecision), and the presence of publication bias. |
| Analgesic | 49 | Naproxen 550 mg | Oral | |||||||
| Fouda | Analgesic | Multiparous adult women | Double-blind RCT | 45 | Copper T380A | Lidocaine 2% gel + Diclofenac potassium 100 mg | Paracervical and oral | Diclofenac potassium combined with 2% lidocaine gel slightly reduced pain scores during tenaculum application and copper IUD insertion in parous women, but with no clinical significance. | 33.4 ± 6.7 | +++° Quality: Moderate - We rated down the quality of evidence (by 1) because of the presence of publication bias. |
| Control | 45 | Placebo | 30.9 ± 8.4 | |||||||
| Miles | Analgesic | Nulliparous and multiparous adult women | Double-blind RCT | 39 | Cooper T380A or LNG | Lidocaine 2% solution + naproxen 375 mg | Intrauterine Oral | Naproxen with or without intrauterine lidocaine does not reduce pain with IUD placement. | 31 ± 8.5 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Analgesic | 39 | Lidocaine 2% solution + placebo | 31 ± 7.4 | |||||||
| Analgesic | 40 | Naproxen 375 mg + placebo | 31 ± 6.5 | |||||||
| Control | 39 | Placebo tablet and solution | 30 ± 6.9 | |||||||
| Sakna | Analgesic | Multiparous adult women | Non-blind RCT | 70 | Cooper T380A | Lidocaine spray 10% 40 mg | Cervical | Pain from IUCD insertion may be effectively managed with 10% local lidocaine spray, which is more convenient than ibuprofen pills and acts quickly. Women chose lidocaine spray over ibuprofen pills. | 32.3 ± 3.7 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the presence of risk of bias and the presence of publication bias. |
| Analgesic | 70 | Ibuprofen 400 mg | Oral | 31.6 ± 4.4 | ||||||
| Ibrahim | Analgesic | Parous women with no prior vaginal delivery | Single-blind RCT | 130 | Cooper T380A | Misoprostol (400 mcg) + Diclofenac 100 mg | Sublingual | Sublingual administration of misoprostol does not facilitate the procedure and may cause undesirable side effects. | 29 ± 5.6 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Analgesic | 125 | Diclofenac 100 mg | Oral | 30 ± 6.5 | ||||||
| Saav | Analgesic | Nulliparous adult women | Single-blind RCT | 39 | Cooper T380A | Misoprostol (400 mcg) + diclofenac 100 mg | Sublingually | Misoprostol facilitates the insertion of an IUD and reduces the number of difficult and failed attempts of insertions in women with a narrow cervical canal. | 22.7 ± 3.1 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Analgesic | 40 | Diclofenac 100 mg | 23.1 ± 2.9 | |||||||
| Abbas | Analgesic | Parous women | Double-blind RCT | 70 | Copper T380A | Ketoprofen 150 mg | Oral | The use of ketoprofen 150 mg before the insertion of copper IUD was effective in reducing pain perception and increasing satisfaction in parous women. | 26.6 ± 4.6 | +++° Quality: Moderate - We rated down the quality of evidence (by 1) because of the presence of publication bias. |
| Control | 70 | Placebo | 25.7 ± 3.9 | |||||||
| Abbas | Analgesic | Parous women | Double-blind RCT | 53 | Copper T380A | Diclofenac potassium 50 mg | Oral | Oral diclofenac potassium slightly reduced the insertional pain and duration compared to oral Hyoscine n-butyl bromide with no adverse effects. | 30.7 ± 6.7 | +++° Quality: Moderate - We rated down the quality of evidence (by 1) because of the presence of publication bias. |
| Analgesic | 54 | Hyoscine n-butyl bromide 20 mg | 30 ± 6.3 | |||||||
| Abo Gharam | Analgesic | Adult women with cervical stenosis | Double-blind RCT | 30 | Copper T380A | Diclofenac sodium 75 mg | Intramuscular | Misoprostol could facilitate the introduction of the copper IUD and diclofenac sodium is useful for pain reduction during this process. | 26.3 ± 5.5 | +°°° Quality: Very low - We rated down the quality of evidence (by 3) because of the presence of risk of bias, the wide confidence interval (Imprecision), and the presence of publication bias. |
| Analgesic | 30 | Misoprostol (400 mcg) | Vaginally | 26.5 ± 6.7 | ||||||
| Buttram | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 17 | Cooper or LNG IUD | Naproxen sodium 550 mg | Oral | Naproxen sodium was favorable over placebo in alleviating cramping pain associated with IUD insertion. | 26.4 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 16 | Placebo | 24.7 | |||||||
| Daykan | Analgesic | Nulliparous women | Double-blind RCT | 22 | LNG IUD | Tramadol 50 mg | Oral | There was no benefit in using oral tramadol for analgesia before IUD insertion among nulliparous women. Verbal analgesia can be a suitable technique for this process and clinicians should become more familiar with its use. | 24.8 ± 3.5 | +°°° Quality: Very low - We rated down the quality of evidence (by 3) because of the presence of risk of bias, the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 32 | Verbal analgesia | 25 ± 2.7 | |||||||
| Peerananrangsee and Thamkhantho, | Analgesic | Nulliparous and multiparous adult women | Double-blind RCT | 65 | Cooper T380A | Etoricoxib 120 mg | Oral | Etoricoxib 120 mg does not help in relieving pain as preemptive analgesia for IUD insertion. But it may be more effective for women with no previous vaginal delivery. | 34.6 ± 7.4 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 65 | Placebo | 36.1 ± 6.8 | |||||||
| Abbas | Analgesic | Multiparous adult women | Double-blind RCT | 50 | Copper T380A | Nitroglycerin cream 1 mL | Cervical lip | Application of cervical GTN cream before IUD insertion seems to reduce the induced pain with subsequent easy insertion. | 29.6 ± 6.4 | +++° Quality: Moderate - We rated down the quality of evidence (by 1) because of the presence of publication bias. |
| Control | 50 | Placebo cream | 30 ± 7.8 | |||||||
| Micks | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 12 | LNG IUD | Nitroglycerin gel 0.5 mg | Vaginally | Vaginal administration of 0.5-mg nitroglycerin gel 30 min before IUD placement does not appear to decrease patient-reported procedural pain among nulliparous women or ease of insertion for providers. | Range: 18–45 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 12 | Placebo | ||||||||
| Bednarek | Analgesic | Nulliparous adult women | Double-blind RCT | 13 | LNG IUD | Nitroprusside gel 10 mg | Cervical | Intracervical administration of 10-mg nitroprusside gel immediately before IUD insertion does not appear to provide a clinically relevant improvement in patient-reported pain with IUD insertion among nulliparous women. | 24.4 ± 4 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 11 | Placebo | 24.2 ± 4 | |||||||
| Erdoğan and Yardımcı, | Analgesic | Multiparous adult women | Double-blind RCT | 36 | Copper T380A | Bilateral LI4 acupuncture | . | Bilateral LI4 acupuncture provides significant pain relief at both cervical and fundal components. Acupuncture before IUD insertion is a significant predictor of lowering overall VAS scores of individuals. | 29.2 ± 6.4 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the presence of risk of bias and the presence of publication bias. |
| Control | 36 | No intervention | 27.1 ± 4.5 | |||||||
| Hylton | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 66 | Cooper T380A or LNG | Cold compress 5 mins before and throughout IUD placement | . | Although a cold compress is a simple, inexpensive, and safe method of pain control, this study shows no reduction in insertional pain for IUD placement. | 30 ± 6.7 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the presence of risk of bias and the presence of publication bias. |
| Control | 72 | Placebo | 31 ± 8.6 | |||||||
| Shahnazi | Analgesic | Nulliparous or multiparous adult women | Double-blind RCT | 53 | Cooper T380A or LNG | Lavender scent | Nasal Mask | Aromatherapy with lavender inhalation was effective in decreasing anxiety in IUD procedures, and this method can be used in health care centers as a complementary treatment. | 28 ± 5.4 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the presence of risk of bias and the presence of publication bias. |
| Control | 53 | Placebo | 28 ± 6.3 | |||||||
| Singh | Analgesic | Nulliparous women | Double-blind RCT | 40 | Cooper T380A or LNG | N2O/O2 | Nasal Mask | N2O/O2 did not reduce the pain of IUD insertion among nulliparous women. | 24.9 ± 5.9 | ++°° Quality: Low - We rated down the quality of evidence (by 2) because of the wide confidence interval (Imprecision), and the presence of publication bias. |
| Control | 40 | O2 | 26.3 ± 5.6 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive Health and Contraception · Pharmaceutical industry and healthcare · Opioid Use Disorder Treatment
1. Introduction
Unplanned pregnancies can be effectively reduced through the use of long-acting reversible contraceptives (LARCs).^1^ Among these, the intrauterine device (IUD) is the most widely used method due to its high cost-effectiveness, favorable safety profile, ease of use, and high patient satisfaction.^2^ It provides a noninvasive alternative to surgical sterilization while offering comparable contraceptive efficacy.^3^ Commonly used IUDs consist of a plastic framework and release either copper or progestin to enhance contraceptive effectiveness.^134^
Globally, the IUD is the most frequently used form of reversible contraception, accounting for approximately 23% of female contraceptive users.^5^ Although the safety profile is generally excellent, complications can occur during and after insertion. These include pain, irregular bleeding, pelvic inflammatory disease, contraceptive failure with a higher risk of ectopic pregnancy, expulsion, and uterine perforation.^6^
Pain during IUD insertion may deter some women from choosing this contraceptive method.^7^ Concerns regarding insertional pain, infection, and a variety of barriers and misconceptions may contribute to its underutilization.^8^ Additionally, healthcare providers may be reluctant to recommend IUDs due to concerns about pain during insertion, technical difficulties, and risk of failure.^9^ Studies have shown that approximately 50% of women experience moderate to severe pain during IUD insertion.^1011^ This pain may result from the use of a tenaculum, insertion of a hysterometer, or placement of the IUD itself. Identified risk factors for increased pain scores include nulliparity, previous cesarean delivery, older age, not currently breastfeeding, anxiety, high anticipated pain, extended time since the last pregnancy, and a history of dysmenorrhea.^12^
Evidence regarding the effectiveness of pharmacological interventions for pain management during IUD insertion remains inconsistent. Pain may be alleviated using various strategies, including conscious sedation, nonsteroidal anti-inflammatory drugs (NSAIDs), local cervical anesthetics (e.g., gels and sprays), cervical ripening agents, nitrous oxide, and paracervical blocks.
Several studies have assessed pharmacological strategies to manage pain during IUD insertion. A recent systematic review and network meta-analysis concluded that lidocaine-prilocaine cream was the most effective intervention.^13^ A meta-analysis by Abu-Zaid et al. found that dinoprostone was both safe and effective for analgesia during IUD insertion.^14^ However, misoprostol has yielded inconsistent results, with some reports indicating increased discomfort and abdominal cramping.^15^ Furthermore, even high-dose oral ibuprofen (800 mg) failed to significantly reduce insertion-related pain.^16^
Given these conflicting findings, the objective of this systematic review and network meta-analysis is to evaluate the safety and efficacy of various pharmacological interventions for pain reduction during IUD insertion and to rank their effectiveness for clinical practice. This review aims to determine which pharmacological interventions are most effective and safe in reducing pain during IUD insertion.
2. Methods
This review was conducted in accordance with the PRISMA extension statement for reporting systematic reviews incorporating network meta-analyses.^17^ The protocol, including full methodological details, was pre-registered in PROSPERO.
2.1. Literature search
A comprehensive literature search was performed across five major databases: PubMed, the Cochrane Central Register of Controlled Trials, Scopus, Web of Science, and Google Scholar, from their inception through September 2023. The search strategy utilized Medical Subject Headings (MeSH) and Boolean operators, adapted for each database. The terms used included: (“pain management” [MeSH] OR “anesthetics, local” [MeSH] OR “anti-inflammatory agents, nonsteroidal” [MeSH] OR “misoprostol” [MeSH] OR “analgesics, opioid” [MeSH] OR “lidocaine” [MeSH] OR “naproxen” [MeSH] OR “diclofenac” [MeSH] OR “ibuprofen” [MeSH] OR “ketorolac” [MeSH]) AND “intrauterine devices” [MeSH]. No restrictions were placed on race, country of origin, or publication date.
Duplicate records were removed using EndNote X7 (Clarivate Analytics, Philadelphia, PA, USA). The remaining studies were imported into Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) for screening. Titles and abstracts were initially screened for relevance, followed by full-text review of potentially eligible articles. The reference lists of included studies were also manually screened to identify any additional relevant publications. Two reviewers independently conducted all screening steps. Discrepancies were resolved by discussion, and when necessary, by consultation with a senior author.
2.2. Eligibility criteria and study selection
Randomized controlled trials (RCTs) were included if they met the following PICO criteria: (1) Population—nulliparous and multiparous women undergoing copper intrauterine device (Cu-IUD) or levonorgestrel-releasing intrauterine device (LNG-IUD) insertion for contraception; (2) Intervention—any pharmacological agent administered for pain relief during IUD insertion; (3) Comparison—placebo, an active comparator, or no medication; and (4) Outcomes—pain during IUD insertion and tenaculum placement as primary outcomes, with secondary outcomes including post-insertion pain, pain at uterine sounding and speculum placement, ease of insertion, need for additional analgesia, procedure duration, and women's satisfaction.
Pain scores were assessed using a 10-centimeter or 100-millimeter visual analogue scale (VAS), where 0 represented no pain and 10 indicated the worst imaginable pain. Ease of insertion was measured using a similar VAS-like scale, with 0 indicating easy insertion and 100 indicating very difficult insertion.^18^ Women's satisfaction was likewise assessed using a VAS-like scale, with 0 denoting no satisfaction and 10 denoting maximum satisfaction.^18^ Safety outcomes included both medication-related side effects (e.g., nausea, vomiting, diarrhea, abdominal cramping, shivering, fever, headache) and procedural complications (e.g., failed insertion, post-insertion bleeding, IUD expulsion, and vasovagal symptoms).
Exclusion criteria were: non-randomized studies, articles not published in English, conference proceedings, review articles, theses, and studies for which full texts were unavailable. RCTs comparing two active drugs directly were excluded from the meta-analysis but included in the qualitative synthesis.
2.3. Data extraction
Four authors independently extracted data on study characteristics, baseline characteristics of participants, risk of bias domains, and outcomes related to efficacy and safety. Disagreements were resolved through discussion, with the involvement of a senior author when necessary. Efficacy outcomes included pain at various time points, ease of insertion, need for additional analgesia, procedure duration, and satisfaction. Safety outcomes included both medication side effects and procedure-related complications.
2.4. Risk of bias assessment and grading of evidence
The methodological quality of each study was assessed using the Cochrane Risk of Bias (RoB) tool, as described in the Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0 (updated March 2011, Chapter 8).^19^ The tool assesses the following domains: sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other sources of bias. Each domain was rated as having a low, high, or unclear risk of bias. All assessments were performed independently, and disagreements were resolved through consensus.
The overall quality of evidence was evaluated using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) criteria.^20^ This approach begins with the assumption that RCTs are high-quality evidence but allows downgrading based on limitations in risk of bias, inconsistency (unexplained heterogeneity), indirectness (e.g., limited generalizability), imprecision (e.g., wide confidence intervals or small sample sizes), and potential publication bias.
2.5. Data synthesis
A frequentist network meta-analysis (NMA) was conducted using the netmeta package in R (R Foundation for Statistical Computing, Vienna, Austria). Standardized mean differences (SMDs) were used to report continuous outcomes derived from VAS scores (e.g., pain, ease of insertion, satisfaction), while mean differences (MDs) were applied to procedure duration. Binary outcomes, such as need for additional analgesics and adverse events, were expressed as risk ratios (RRs). All effect estimates were presented with 95% confidence intervals (CIs). When outcomes were reported as medians with ranges or interquartile ranges (IQRs), these were converted to means and standard deviations using the method described by Wan et al.^18^
Statistical significance was defined as a 95% CI not including zero (for SMDs and MDs) or one (for RRs). A back-calculation method was used to estimate indirect effects from direct pairwise comparisons, following the frequentist NMA framework.^19^ Heterogeneity was assessed using generalized Cochran's Q statistics for multivariate meta-analysis, as described by Krahn et al.^20^ A P value <0.1 and an I^2^ statistic of 50% or greater indicated significant heterogeneity.^21^ The Netsplit function in R, which tests consistency between direct and indirect estimates, could not be applied in this analysis because it requires triangular treatment comparisons. However, no significant inconsistency was observed between direct and indirect comparisons, supporting the validity of the network.
The random-effects model was used throughout. Paired treatment comparisons were presented in league tables. Treatment groups were ranked using the P-score, which ranges from 0 to 1, with higher values indicating greater efficacy or safety. P-scores are derived from standard errors and point estimates and are interpreted similarly to the surface under the cumulative ranking curve (SUCRA).^2223^
2.6. Publication bias
For outcomes with ten or more contributing studies, publication bias was evaluated using Egger's test, and the results were visualized using funnel plots. A P value of <0.05 was considered indicative of potential publication bias.^24^
3. Results
3.1. Results of the literature search and characteristics of included studies
The systematic literature search identified 1,117 unique records. Following the exclusion of ineligible articles based on title and abstract screening, 174 articles proceeded to full-text review. Ultimately, 48 randomized controlled trials (RCTs) were deemed eligible for inclusion in the network meta-analysis (N = 8,656 patients).^252627282930313233343536373839404142434445464748495051525354555657585960616263646566676869707172^ An additional 23 articles were included in a narrative synthesis due to ineligibility for meta-analysis (N = 2,214 patients) [Supplementary Figure 1 and Supplementary Table 1].^7374757677787980818283848586878889909192939495^
3.2. Characteristics of included studies
The included studies enrolled nulliparous and multiparous women aged 15 to 51 years undergoing copper or levonorgestrel-releasing IUD insertion. Among the included interventions, three studies evaluated lidocaine-prilocaine cream (5%),^304772^, and eight studies investigated lidocaine gel,^3349575859606467^ both of which demonstrated variable efficacy in reducing IUD insertion pain [Table 1,Table 2,Table 3,Table 4].
Five studies reported that lidocaine spray was effective in decreasing insertion-related pain,^2631344452^ while results were mixed for lidocaine paracervical block.^384548505154^ nesthetic solutions containing lignocaine or mepivacaine demonstrated efficacy, whereas lidocaine in this form did not.^295772^ One study found that lidocaine spray, cream, and paracervical block all provided pain relief during IUD insertion.^52^
Twelve RCTs evaluated the use of misoprostol at doses of either 200 mcg or 400 mcg, administered orally, sublingually, or vaginally, for cervical ripening prior to IUD insertion.^272832363741435661626569^ These studies demonstrated inconsistent results. Four trials reported significant pain reduction during insertion,^41436569^ whereas the remainder found no effect.^2728323637566162^ Reported side effects of misoprostol included nausea,^27283762^ abdominal cramping,^37^ IUD expulsion,^36^ failed insertion,^36^ and vaso-vagal reaction.^32^ In contrast, dinoprostone was found to reduce insertion-related pain while maintaining an acceptable side-effect profile.^2829404255^
Regarding NSAIDs, three studies concluded that 800 mg oral ibuprofen was ineffective in reducing IUD insertion pain.^636670^ Intramuscular ketorolac (20 mg) did not reduce insertion pain but did relieve pain at 5 and 15 minutes post-insertion,^39^ whereas oral ketorolac (20 mg) was more effective, reducing insertion pain, overall pain scores, and pain at 10 minutes post-procedure.^71^ Naproxen (550 mg orally) was effective in one study but showed no effect in another.39,50 Diclofenac sodium (75 mg intramuscularly) and tramadol (50 mg orally) were both reported as effective in reducing insertion pain.^4369^
Reasons for excluding certain studies from the network meta-analysis included use of head-to-head comparisons of analgesics,^737479818290919394^ unique pharmacological interventions without comparison,^7677808387888995^ reporting only changes in pain scores,^7578^ or not reporting VAS score [Supplementary Table 2].^86^ Baseline characteristics of the included study populations are summarised in detail [Table 1,Table 2,Table 3,Table 4].
3.3. Quality and risk of bias assessment
The overall risk of bias in included studies ranged from low to moderate. Most studies adequately reported randomization and allocation procedures; however, 11 studies lacked sufficient detail in these areas.^2545505156657374818288^ Four studies were conducted as open-label trials,^50748182^ and five employed single blinding limited to study personnel.^3445485269^ Seven studies did not confirm blinding of outcome assessors [Supplementary Figure 2].^48545978828390^
According to GRADE criteria, most included studies were of low quality, scoring 2 out of 4 possible points. Downgrading of evidence was primarily due to imprecision (i.e., wide confidence intervals), risk of bias as determined by the Cochrane RoB tool, and possible publication bias associated with small sample sizes [Table 1,Table 2,Table 3,Table 4].
3.4. Study outcomes and ranking study medications
3.4.1. Efficacy outcomes
ain during intrauterine device (IUD) insertion was reported in 42 studies (n = 7,079). The network meta-analysis (NMA) demonstrated significant pain reduction with lidocaine 4% gel, lidocaine 1% solution, lidocaine 2% paracervical block, dinoprostone, lidocaine-prilocaine cream, lignocaine solution, lidocaine spray, naproxen, misoprostol, and lidocaine 2% paracervical block (10 mL) [Fig. 1, Supplementary Table 3]. Treatment rankings are presented in Supplementary Table 4. Considerable heterogeneity was observed (I^2^ = 87.4%); however, inconsistency could not be assessed due to the absence of a closed-loop comparison.
Pain during intrauterine device insertion.
Pain at tenaculum insertion was reported in 29 studies (n = 3,267). The NMA revealed significant pain reduction with lidocaine 4% gel, lidocaine 1% solution, lidocaine-prilocaine 5% cream, lidocaine 2% gel, lidocaine 10% spray, ketorolac, and dinoprostone, compared to placebo [Supplementary Figure 3, Supplementary Table 3]. Substantial heterogeneity was identified (I^2^ = 72.3%), and inconsistency could not be tested due to the absence of a closed-loop.
Pain after IUD insertion was assessed in 28 studies (n = 3,147). Compared to placebo, significant pain reduction was observed with lidocaine 4% gel, lidocaine 1% solution, and ketorolac [Supplementary Figure 4, Supplementary Table 3]. High heterogeneity was detected (I^2^ = 94.2%).
Pain during uterine sounding was evaluated in 12 trials (n = 1,253). The analysis showed that lidocaine 4% gel, lidocaine-prilocaine cream, lidocaine 2% gel, and lidocaine 10% spray significantly reduced pain compared to placebo [Supplementary Table 3]. The degree of heterogeneity was substantial (I^2^ = 73.5%).
Ease of IUD insertion was examined in 10 studies (n = 1,507). Misoprostol 400 mcg, lidocaine-prilocaine 5% cream, and dinoprostone 3 mg significantly improved ease of insertion [Supplementary Table 3]. Heterogeneity was high (I^2^ = 94.8%).
The need for additional analgesia was assessed in seven trials (n = 927). Lidocaine-prilocaine 5% cream, misoprostol 400 mcg, and dinoprostone 3 mg significantly reduced the requirement for further analgesia [Supplementary Table 3]. No heterogeneity was detected (I^2^ = 0%).
Patient satisfaction was evaluated in six studies (n = 866). Misoprostol 400 mcg, lidocaine-prilocaine 5% cream, and dinoprostone 3 mg were associated with higher satisfaction scores compared to placebo [Supplementary Table 3]. Substantial heterogeneity was identified (I^2^ = 95.3%).
Pain during speculum insertion was measured in 10 trials (n = 798). The NMA found no significant differences in pain reduction between active treatments and placebo [Supplementary Table 3]. Rankings are shown in Supplementary Table 4. No heterogeneity was detected (I^2^ = 0%).
Procedure duration was reported in six studies (n = 802). No significant differences in insertion time were observed across treatments compared to placebo [Supplementary Table 3]. Treatment rankings are available in Supplementary Table 4. Considerable heterogeneity was observed (I^2^ = 97.9%).
The effect estimates, 95% confidence intervals, and the corresponding level of evidence for all efficacy outcomes are summarised in Supplementary Table 5.
3.5. Safety outcomes
The NMA indicated that ketorolac 20 mg (95% CI: 0.01–5.66) and naproxen 550 mg (95% CI: 0.10–2.77) were associated with a lower risk of nausea, with significant heterogeneity detected (P = 0.02). Naproxen 550 mg (95% CI: 0.01–4.22) and lidocaine-prilocaine 5% cream (5 mL; 95% CI: 0.04–3.72) demonstrated the lowest risk of vomiting. Diarrhea was reported less frequently with lidocaine-prilocaine 5% cream (5 mL; 95% CI: 0.06–8.76) and misoprostol 400 mcg (95% CI: 0.45–3.24), with no significant heterogeneity observed (P = 0.71 and P = 0.84, respectively) [Supplementary Table 6].
Abdominal cramping was reduced with lidocaine-prilocaine 5% cream (5 mL; 95% CI: 0.16–2.90) and lidocaine 2% gel (95% CI: 0.40–2.68), though significant heterogeneity was present (P = 0.015). Shivering was less common with lidocaine-prilocaine 5% cream (5 mL; 95% CI: 0.02–7.41) and misoprostol 200 mcg (95% CI: 0.21–5.15), with no heterogeneity detected (P = 0.89).
Fever was lower with lidocaine-prilocaine 5% cream (5 mL; 95% CI: 0.09–10.43) and misoprostol 200 mcg (95% CI: 0.81–10.92), whereas dinoprostone 3 mg was associated with a higher incidence (95% CI: 1.55–9.32; P = 0.98). Headache occurred least frequently with lidocaine-prilocaine 5% cream (5 mL; 95% CI: 0.01–2.72), followed by ketorolac 20 mg (95% CI: 0.01–2.74), with no heterogeneity (P = 0.68).
Failure of IUD insertion was assessed only for misoprostol, with misoprostol 200 mcg (95% CI: 0.04–2.64) and 400 mcg (95% CI: 0.16–3.19) associated with lower risk and no significant heterogeneity (P = 0.15). Post-insertion bleeding was least frequent with lidocaine-prilocaine 5% cream (5 mL; 95% CI: 0.25–1.30) and misoprostol 200 mcg (95% CI: 0.34–1.64). IUD expulsion occurred less frequently with lidocaine 2% gel (95% CI: 0.03–2.22) and lidocaine-prilocaine 5% cream (95% CI: 0.21–7.75).
Vasovagal symptoms were reduced with dinoprostone 3 mg (95% CI: 0.35–1.93) and misoprostol 400 mcg (95% CI: 0.68–2.29). Other interventions showed no significant differences from placebo, and no heterogeneity was detected (P >0.1) [Supplementary Table 6]. Effect estimates, confidence intervals, and P-scores for safety outcomes are summarised in Supplementary Table 5.
3.6. Publications bias
No publication bias was detected for diarrhea (P = 0.03). Funnel plot asymmetry was observed for pain during IUD insertion (P = 0.67), pain after IUD insertion (P = 0.07), pain during tenaculum placement (P = 0.07), pain during uterine sounding (P = 0.26), ease of insertion (P = 0.36), vomiting (P = 0.62), abdominal cramping (P = 0.49), and post-insertion bleeding (P = 0.60) [Supplementary Table 7].
4. Discussion
4.1. Main findings
This systematic review and network meta-analysis of 71 randomized controlled trials involving 10,870 women identified lidocaine 4% gel (5 mL) as the most effective intervention for reducing pain during IUD insertion, tenaculum placement, uterine sounding, and post-insertion, in addition to achieving the shortest procedural duration. Lidocaine spray (10%; 40 mg) was most effective for pain relief during speculum placement, while lidocaine-prilocaine 5% cream (5 mL) was associated with the lowest need for additional analgesia. Misoprostol 400 mcg facilitated insertion most effectively, and lidocaine 2% gel (2 mL) was linked to the highest patient satisfaction.
In terms of safety, lidocaine-prilocaine 5% cream (5 mL) showed the lowest incidence of common side effects, including gastrointestinal symptoms, headache, and post-insertion bleeding. Fewer instances of nausea and vomiting were associated with ketorolac 20 mg and naproxen 550 mg, respectively. Reduced rates of insertion failure, IUD expulsion, and vasovagal symptoms were noted with misoprostol 200 mcg, lidocaine 2% gel (3 mL), and dinoprostone 3 mg.
Lidocaine acts by blocking voltage-gated sodium channels, thereby inhibiting nociceptive signal transmission.^99^ Its topical formulation offers rapid absorption and broad mucosal coverage, contributing to its analgesic superiority, particularly in the cervix, which is innervated by pelvic splanchnic nerves and the uterovaginal plexus.
4.2. Comparison with existing literature
Perez-Lopez et al. reviewed 11 RCTs involving 1,458 women and reported that intrauterine or paracervical lidocaine significantly reduced pain during tenaculum placement, IUD insertion, and up to 20 minutes post-procedure, without severe adverse effects.^96^ Similarly, a 2015 meta-analysis^16^ found that topical lidocaine 4% gel, 10% spray, and lidocaine-prilocaine cream were more effective than placebo in reducing IUD insertion pain.^16^
Lidocaine-prilocaine (LP) cream is an emulsion containing 2.5% of each component. The combined effect may enhance analgesia at the uterine level.^13^ In the present NMA, LP 5% cream was the most effective in reducing the need for additional analgesia, ranked second in improving ease of insertion and reducing pain during uterine sounding, and third in relieving pain at tenaculum placement. However, it ranked fifth for reducing pain during and after IUD insertion.
These findings contrast with those of Samy et al., where LP cream was ranked as the most effective intervention for pain reduction during and after insertion and during tenaculum placement.^13^ Both analyses, however, found LP cream to be the most effective in lowering the need for additional analgesia. A discrepancy also exists with Perez-Lopez et al., who concluded that LP cream offered superior pain control compared to lidocaine alone.^96^ Differences in sample size and study inclusion criteria—particularly the broader categorisation of drug formulations, concentrations, and administration volumes—may explain these inconsistencies.
The present findings align with Samy et al. in ranking misoprostol last for IUD insertion pain reduction.^13^ Misoprostol was also ineffective for reducing pain post-insertion and at tenaculum placement. The 200 mcg dose demonstrated greater effectiveness than 400 mcg for these outcomes. Conversely, misoprostol 400 mcg ranked highest for improving ease of insertion and second in reducing the need for additional analgesia. As a cervical ripening agent, misoprostol may facilitate insertion, particularly in nulliparous women. However, its analgesic effect remains limited. In one study, nulliparous women treated with misoprostol showed no significant change in VAS scores.^97^ Tassi et al. reported increased pain scores following sublingual and buccal misoprostol, although it lowered the need for cervical dilation and insertion failure rates in patients with a history of caesarean section or failed IUD insertion.^4^ Nonetheless, its prostaglandin activity is associated with side effects such as abdominal cramping.
Nonsteroidal anti-inflammatory drugs (NSAIDs) have been investigated extensively with mixed outcomes. In the current analysis, naproxen 550 mg reduced insertion pain, and ketorolac 20 mg was effective for post-insertion and tenaculum-related pain. However, both medications were associated with increased nausea, vomiting, and headache. Samy et al. reported no significant analgesic benefit of NSAIDs over placebo.^13^ Similarly, a 2015 meta-analysis found that naproxen reduced pain in only one of two trials, oral ibuprofen was ineffective across four trials, and intramuscular ketorolac relieved pain post-insertion only in nulliparous women.^16^
Findings related to dinoprostone align with those of Abu Zaid et al., who reported that dinoprostone significantly reduced pain during IUD insertion, tenaculum placement, and uterine sounding, while also decreasing the need for additional analgesia, improving satisfaction, and facilitating insertion.^14^ Although the current analysis also confirmed its efficacy, dinoprostone was associated with a significantly higher incidence of diarrhea, vomiting, and abdominal cramping.
Farrar et al. proposed a clinically important difference (CID) threshold of 2 on the VAS scale (equivalent to 20 mm) as a benchmark for meaningful pain improvement.^98^ Applying this criterion, local anaesthetics were the only class of interventions that consistently achieved a clinically significant reduction in pain during all procedural stages: tenaculum placement, uterine sounding, IUD insertion, and post-insertion.
Given the subjective nature of pain, outcomes such as patient satisfaction and self-reported pain scores were prioritised in this analysis. These patient-centred measures provide critical insights into the perceived effectiveness of interventions. However, psychological and physiological factors such as anxiety, tension, and individual pain thresholds likely influenced these outcomes. Although such confounding variables could not be controlled in the current analysis, future studies are encouraged to incorporate psychological assessment tools to account for their potential effects.
4.3. Strengths and weaknesses
This systematic review and network meta-analysis has several notable strengths. It adheres to PRISMA-NMA and Cochrane Handbook guidelines, representing the largest and most comprehensive analysis to date on analgesic interventions for IUD insertion. Study quality was moderate, as assessed by the Risk of Bias (RoB) tool and the GRADE framework. Only randomized, placebo-controlled trials were included, thereby minimizing the risk of selection bias and confounding. A wide range of efficacy and safety outcomes was assessed, allowing for a more holistic evaluation of the interventions.
However, several limitations must be acknowledged. Substantial statistical heterogeneity was observed, likely attributable to clinical heterogeneity in participant characteristics, procedural differences in IUD insertion techniques, variations in drug formulation and administration timing, inconsistency in the timing of pain assessment, and sociocultural influences. Subjective pain evaluations may also have been affected by unreported psychological factors such as pre-procedural anxiety, relaxation ability, and individual pain thresholds, which were not consistently accounted for and may represent potential sources of bias.
In addition, limitations related to imprecision, risk of bias, and possible publication bias contributed to the overall low quality of evidence in many comparisons. Future studies should prioritise large-scale, high-quality randomised controlled trials evaluating the most promising analgesic interventions. The incorporation of validated anxiety assessment tools—such as the State-Trait Anxiety Inventory or the Visual Analogue Anxiety Scale—prior to IUD insertion may help identify psychological confounders. Furthermore, research into adjunct strategies including anxiolytics, guided relaxation techniques, and cognitive-behavioural approaches may clarify their role in modulating procedural pain.
An individual participant data meta-analysis (IPDMA) was not conducted due to resource and time constraints.^99^ Although IPDMA offers several methodological advantages, the anticipated benefit over aggregate data meta-analysis (ADMA) in this context may not justify the additional demands. As previous research suggests comparable outcomes between the two approaches, an ADMA was deemed appropriate for the objectives of this review.
5. Conclusion
Lidocaine 4% gel (5 mL) emerged as the most effective pharmacological intervention for reducing pain during and after intrauterine device (IUD) insertion, tenaculum placement, and uterine sounding, while also contributing to shorter procedure duration and demonstrating no reported side effects. Lidocaine 1% solution (10 mL) ranked second, providing significant analgesia during IUD insertion and tenaculum placement. Both formulations produced clinically meaningful pain reduction; however, the quality of evidence remains low, with a GRADE rating of 2 out of 4. In patients at risk of difficult insertion, agents such as misoprostol and dinoprostone may be beneficial for improving procedural ease and lowering the risk of insertion failure.
Authors' Contribution
Ahmed Ashour: Conceptualization, Methodology, Supervision, Formal analysis, Writing – Review & Editing. Ahmed H. Saad: Data Curation, Software, Investigation, Writing – Original Draft Preparation. Iman Elzahaby: Validation, Visualization, Resources, Writing – Review & Editing.
Acknowledgement
The authors would like to acknowledge Dr. Ahmed Said Ali and Dr. Mahmoud Alalfy for their valuable contributions to specific stages of this work, including data verification and methodological discussions. Their input enriched the quality of the manuscript.
Data Availability
Data is available upon reasonable request from the corresponding author.
Supplementary Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Winner B Peipert JF Zhao Q Effectiveness of long-acting reversible contraception. New England Journal of Medicine 2012; 366(21):1998–2007. doi: 10.1056/NEJ Moa 1110855.10.1056/NEJ Moa 111085522621627 · doi ↗ · pubmed ↗
- 2Akers AY Harding J Perriera LK Schreiber C Garcia-Espana JF Sonalkar S Satisfaction with the intrauterine device insertion procedure among adolescent and young adult women. Obstetrics & Gynecology 2018; 131(6):1130–1136. doi: 10.1097/AOG.0000000000002596.29742656 PMC 6104388 · doi ↗ · pubmed ↗
- 3Buhling KJ Zite NB Lotke P Black K Worldwide use of intrauterine contraception: A review. Contraception 2014; 89(3):162–173. doi: 10.1016/j.contraception.2013.11.011.10.1016/j.contraception.2013.11.01124369300 · doi ↗ · pubmed ↗
- 4Tassi A Parisi N Londero AP Misoprostol administration prior to intrauterine contraceptive device insertion: a systematic review and meta-analysis of randomised controlled trials. The European Journal of Contraception & Reproductive Health Care 2020; 25(1):76–86. doi: 10.1080/13625187.2019.1706079.31914331 · doi ↗ · pubmed ↗
- 5Buhling KJ Zite NB Lotke P Black K Group IW Worldwide use of intrauterine contraception: a review. Contraception 2014; 89(3):162–173. doi: 10.1016/j.contraception.2013.11.011.10.1016/j.contraception.2013.11.01124369300 · doi ↗ · pubmed ↗
- 6Bliss Kaneshiro B Long-term safety, efficacy, and patient acceptability of the intrauterine Copper T-380A contraceptive device. Int J Womens Health 2010; 2:211–20. doi: 10.2147/ijwh.s 6914.10.2147/IJWH.S 691421072313 PMC 2971735 · doi ↗ · pubmed ↗
- 7Gemzell-Danielsson K Jensen JT Monteiro I Interventions for the prevention of pain associated with the placement of intrauterine contraceptives: An updated review. Acta Obstet Gynecol Scand 2019; 98(12):1500–1513. doi: 10.1111/aogs.13662.10.1111/aogs.1366231112295 PMC 6900125 · doi ↗ · pubmed ↗
- 8Black K Lotke P Buhling KJ Zite NB A review of barriers and myths preventing the more widespread use of intrauterine contraception in nulliparous women. Eur J Contracept Reprod Health Care 2012; 17(5):340–350. doi: 10.3109/13625187.2012.700744.10.3109/13625187.2012.70074422834648 PMC 4950459 · doi ↗ · pubmed ↗