Airway Abnormalities in Children Operated for Congenital Heart Disease: Clinical characteristics and risk factors from a case-control study
Fatma Al Kindi, Rand Al Harthy, Saif Awlad Thani, Hamood Al Kindi, Hussain Mohsin

TL;DR
This study finds that airway abnormalities are common in children with congenital heart disease and are linked to factors like prematurity.
Contribution
The study identifies risk factors and clinical characteristics of airway abnormalities in children with CHD through a case-control design.
Findings
Airway abnormalities occurred in 5.5% of children with CHD.
Vascular compressions were the most common type of airway abnormality.
Prematurity was a significant risk factor for airway abnormalities.
Abstract
Congenital heart disease (CHD) is the most common congenital defect, with airway abnormalities (AAs) representing significant comorbidities that contribute to increased morbidity and clinical complexity. This study aimed to identify the most common AAs, associated risk factors, and clinical outcomes in children with CHD. This case-control study included children aged under 13 years with CHD who underwent cardiothoracic surgery between 1 January 2016 and 31 December 2018 at the National Genetic Centre in Oman. Cases were children with concurrent AAs, while controls were age- and gender-matched children with CHD but without AAs. The prevalence of concomitant AAs in children with CHD in the cohort was 5.5%. The most common AAs were vascular compressions (47.4%), followed by airway malacia (23.1%). Chest computed tomography was the most frequently utilised diagnostic modality. Prematurity…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
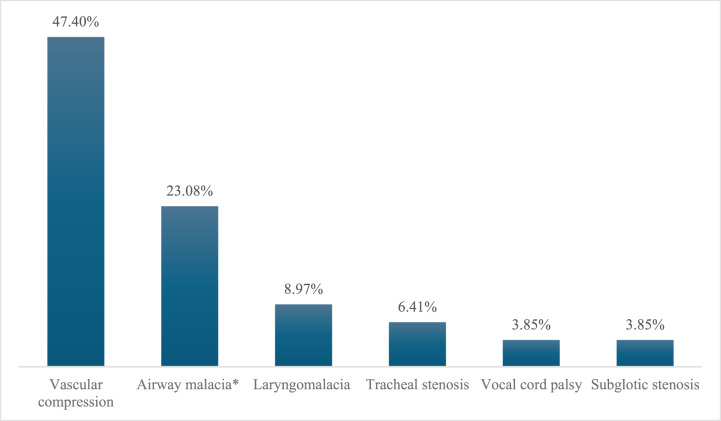 Fig. 1
Fig. 1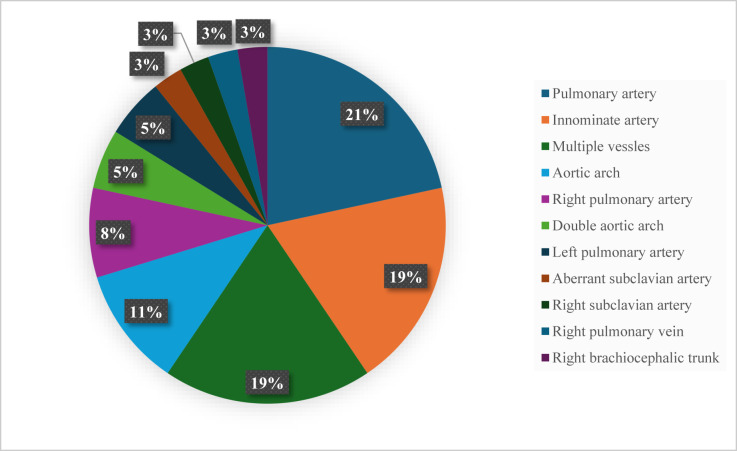 Fig. 2
Fig. 2| Cases (n = 78) | Control (n = 78) | |||
|---|---|---|---|---|
|
|
| |||
| Variable | n (%) | Odd ratio (95% CI) | ||
| Gender | Females: 44 (56) | Females: 39 (50) | ||
| Age in months (mean ± SD) | 13 ± 16.7 | 12.8 ± 16.7 | 0.94 | |
| Weight in kg (mean ± SD) | 6.4 ± 3.8 | 7.5 ± 3.4 | 0.25 | |
| Cyanotic heart disease | 43 (55) | 50 (64) | 0.26 | 0.69 (0.34–1.37) |
| Lung collapse | 50 (64.1) | 49 (62) | 0.87 | 1.05 (0.53–2.08) |
| Prematurity | 18 (23) | 7 (8.9) | 0.016 | 3.2 (1.12–11.16) |
| Dysmorphism | 30 (39) | 25 (32) | 0.38 | 1.35 (0.64–2.92) |
| Down syndrome | 9 (11.5) | 13 (16) | 0.37 | 0.66 (0.23–1.77) |
| Congenital Heart Disease type | n (%) |
|---|---|
| Enlarged pulmonary artery | 53 (34) |
| Tetralogy of Fallot | 28 (17.9) |
| Single ventricle – Enlarged Aorta | 23 (14.7) |
| Aortic Arch Anomaly/Coarctation of Aorta | 21 (13.5) |
| Transposition of Great Arteries | 13 (8.3) |
| Miscellaneous | 12 (7.7) |
| Vascular Ring | 6 (3.8) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Tracheal and airway disorders · Airway Management and Intubation Techniques
1. Introduction
Congenital Heart Disease (CHD) is the most common congenital defect, with a global prevalence of 5 to 8 per 1,000 live births.^1^ In Oman, the incidence has been reported at 7.1 per 1,000 births.^2^ Advances in healthcare have substantially reduced the mortality associated with CHD, shifting clinical focus towards comorbidities such as airway abnormalities (AAs), which can significantly influence outcomes.^3^ AAs are associated with CHD due to the parallel development of the cardiac and respiratory systems during the embryonic period, during which intrauterine insults may affect both.^3^
Various cardiovascular defects are linked to different AAs. Infants are particularly susceptible to airway compression due to immature support structures and low airway conductance.^4^ International studies from Taiwan, Canada, and China report that approximately 3–4% of children with CHD have concomitant congenital AAs.^3567^ However, regional data on this association are limited.
This study aimed to describe the prevalence of AAs among children undergoing surgery for CHD in Oman. It also sought to identify the most common types of AAs, characterise their clinical presentation, determine the diagnostic modalities used and evaluate risk factors including type of CHD, prematurity, dysmorphism or genetic diagnosis and outcomes such as the duration of mechanical ventilation, need for surgical intervention or tracheostomy and re-hospitalisation.
2. Method
This was a retrospective case-control study involving children under 13 years of age with CHD who underwent surgery at the National Genetic Centre in Oman between 1 January 2016 and 31 December 2018. Cases were children with concurrent AAs confirmed by fibreoptic laryngoscopy (FOL), rigid bronchoscopy, flexible bronchoscopy or chest computed tomography (CT). The cases were either symptomatic preoperatively with respiratory symptoms for which they underwent airway assessment, or asymptomatic, and the AAs were detected from the Chest CT, which was performed to assess their cardiac anatomy preoperatively. Some patients underwent flexible bronchoscopy for high-risk cardiac lesions, such as absent pulmonary valve syndrome, in which all children undergo routine screening flexible bronchoscopy as part of their operative planning. For those who were diagnosed postoperatively, they were assessed for AAs based on clinical suspicion, e.g., persistent or recurrent lung collapse and failure of extubation. These patients were assessed as follows: first, their previous Chest CT was evaluated for AA. This was followed by either flexible bronchoscopy performed by pediatric pulmonology or otolaryngology assessment using FOL or rigid bronchoscopy. Some patients required a repeated Chest CT. This was guided by the clinical presentation and the patient's clinical stability to undergo these investigations. Controls were children with CHD who underwent surgery during the same period but had no AAs. Both groups were matched for age (±3 months) and gender in a 1:1 ratio.
Control selection was conducted using simple random sampling. For each case, a list of all eligible controls meeting the matching criteria were generated and one control was randomly selected. This process was repeated until 78 matched controls were identified. As the controls had no clinical signs or symptoms suggestive of airway pathology, it was assumed they did not have AAs, even if they had not undergone airway imaging or bronchoscopy.
Data was collected from the hospital's electronic health records. Variables included age, gender, weight at diagnosis, surgery date, presenting symptoms or signs of airway involvement, type of CHD, type of AA, prematurity (defined as gestational age <37 weeks), presence of associated symptoms, genetic diagnoses or comorbidities, diagnostic methods used (chest CT, bronchoscopy, FOL), airway interventions, length of hospital stay and duration of non-invasive and invasive ventilation. Data quality was maintained through continuous oversight of data collection.
Statistical analysis was performed using STATA version 17 (StataCorp LLC, Texas, USA). Categorical data were summarised as frequencies and percentages, and continuous data as means and standard deviations. Comparisons between matched continuous variables were conducted using paired Student's t-tests, while McNemar's test was used for categorical variables. Odds ratios (OR) with 95% confidence intervals (CI) were reported. A P-value of <0.05 was considered statistically significant. Multivariate analysis was not performed as only one significant risk factor emerged in univariate analysis.
3. Results
A total of 1,419 children underwent surgery for CHD at the National Heart Centre in Oman during the study period. Of these, 81 children were confirmed to have AAs; however, 3 cases were excluded due to insufficient data. Thus, 78 children were included in the analysis as cases and 78 age- and gender-matched children included as controls.
The prevalence of AAs among children operated for CHD was 5.5%. Among the 78 cases, 44 (56%) were female. Cyanotic CHD comprised the majority of cardiac lesions in both the case and control groups, accounted for 55% (n = 43) of cases and 64% (n = 50) of controls [Table 1]. The classification of CHD is presented in Table 2.
The most common AA was vascular compression (47.4%, n = 37), followed by airway malacia, including tracheomalacia, bronchomalacia and combined trachea-bronchomalacia (23%, n = 18) [Fig. 1]. In children with vascular compression, the pulmonary artery was the most frequent compressing vessel (21%), followed by the innominate artery (19%) [Fig. 2].
*Airway abnormality diagnoses among children operated for congenital heart disease (N = 78). Airway malacia includes tracheomalacia, bronchomalacia or combined tracheo-bronchomalacia.
Compressing vessels for patients with vascular compression (N = 37).
Most cases were diagnosed after surgery (72.4%, n = 55). Onset of airway-related signs and symptoms occurred postoperatively in 49.4% (n = 38), while 35% (n = 27) presented before surgery. The remaining 15.6% (n = 12) were asymptomatic. Clinical presentations varied, with many patients experiencing multiple symptoms. These included lung collapse (64%), stridor (43.6%), failure of extubation (35.9%), feeding intolerance (34.6%), difficult intubation (15.4%) and voice change (10.3%). Stridor was the most common preoperative symptom, while lung collapse predominated postoperatively. Difficult intubation was attributed to an anterior larynx, tubular epiglottis, micrognathia, retrognathia, cleft palate or subglottic stenosis preventing passage of the endotracheal tube.
Chest CT was the most commonly used diagnostic modality, identified AAs in 50% of cases. Other diagnostic approaches included upper airway assessment by otolaryngology using FOL or rigid bronchoscopy (20%) and flexible bronchoscopy (11%). The remaining 19% were diagnosed using more than one modality. As stated in the methods section, all patients with postoperative clinical suspicion of AA were evaluated in a stepwise approach, which was guided by their clinical presentation and stability to undergo these investigations.
With regard to risk factors, prematurity was significantly more common among cases compared to controls, occurring in 23% versus 8.9%, respectively (OR: 3.2, 95% CI: 1.1–11.1; P = 0.016). Lung collapse, defined as complete right or left lung collapse or lobar collapse, was reported in 64% (n = 50) of cases and 62% (n = 49) of controls (P = 0.87; OR: 1.05). Other factors assessed—including type of CHD (cyanotic versus acyanotic), dysmorphism, Down syndrome and other genetic syndromes—did not differ significantly between groups [Table 1].
The mean duration of invasive ventilation was 11.8 ± 28.5 days in cases and 3.7 ± 4.5 days in controls (P = 0.013). Readmission within 1 month of discharge occurred in 12 cases (16.7%). Most cases (68.8%, n = 53) did not require intervention for the AA. Among the 24 children (31.2%) who did, the most common procedure was vascular-pexy (52.4 %, n = 11), followed by tracheostomy (25%, n = 6), airway surgery (16.7%, n = 4) and combined airway surgery with tracheostomy (12.5%, n = 3).
4. Discussion
This study identified a prevalence of airway abnormalities (AAs) of 5.5% among children who underwent surgery for congenital heart disease (CHD), which is higher than the 3–4% prevalence reported in previous literature.^36^ This elevated rate may be attributed to the study's focus on children who had undergone surgical intervention, whereas other studies have reported prevalence across the entire CHD population, regardless of surgical status. The inclusion of only post-surgical cases likely led to a greater detection of AAs, as these children often represent more complex clinical scenarios compared to the broader CHD population.
The paediatric airway has distinct anatomical and physiological features, making it particularly vulnerable to extrinsic compression and malacia. These include immature airway support structures and reduced airway conductance.^4^ Consequently, even mild airway compression in young children may result in clinically significant obstruction. Early identification and management of such abnormalities are therefore essential to prevent long-term complications, such as bronchiectasis secondary to chronic lung collapse or recurrent respiratory infections.
Vascular compression was the most frequently identified AA in this study (47.4%), followed by airway malacia (23.1%). These findings are consistent with reports from China, where similar patterns were observed.^7^ However, some studies have reported a higher prevalence of airway malacia than vascular compression—for example, one study noted that malacia affected 59.1% of cases.^5^ These discrepancies may be due to differences in underlying CHD types, diagnostic protocols, or regional variations in patient characteristics.
In our cohort, the signs and symptoms of AAs were more frequently observed following surgery (49.4%), with diagnoses made postoperatively in 72.4% of cases. These findings underscore the need for preoperative assessment of potential co-existing AAs in children with CHD, as early recognition could improve perioperative planning and postoperative outcomes.
Chest computed tomography (Chest CT) was the most commonly used diagnostic modality, contributing to 50% of the AA diagnoses. This likely reflects its frequent use in preoperative cardiac evaluations, during which AAs may be detected incidentally. Other diagnostic tools included upper airway assessment via fibreoptic laryngoscopy (FOL) or rigid bronchoscopy (20%) and flexible bronchoscopy (11%). The reliance on CT imaging is consistent with published evidence suggesting its utility in identifying severe airway compression.^8^ Nonetheless, in cases of suspected airway malacia, advanced imaging techniques such as virtual CT bronchoscopy, dynamic inspiratory and expiratory scans, and pulmonary function testing with flow-volume loops may provide added diagnostic value.
In terms of clinical presentations, lung collapse was the most frequently observed symptom (64%), occurring in both cases and controls. While lung collapse is a recognised indication for further evaluation of airway pathology, it may also occur in the absence of AAs. Stridor was the second most common symptom (43.6%). In contrast, another study has identified feeding intolerance as the predominant presentation.^6^ Failure of extubation was noted in 35.9% of cases in this study, which is consistent with findings in the literature.^69^ Voice changes and difficult intubation were seen in 10.3% and 15.4% of cases, respectively, contrasting with one study that reported a higher rate of voice changes (25%).^6^ These discrepancies highlight the heterogeneity in clinical manifestations and reinforce the need for tailored perioperative assessment in children with CHD.
It is important to highlight that children with vascular compression and tracheobronchomalacia can be misdiagnosed with asthma due to overlying symptoms, including cough, noisy breathing, and shortness of breath.^101112^ Hence, it is important to rule out the presence of AA in children with congenital heart disease presenting with respiratory symptoms before attributing that to asthma. This can be achieved with a thorough history and proper physical examination. While asthma is an episodic disease with intermittent symptoms that typically improve with bronchodilators, children with vascular compression or tracheobronchomalacia present with persistent symptoms that may worsen after bronchodilator administration. Wheezing in asthma is musical, diffuse, and high-pitched, while in malacia it is mostly low-pitched, monophonic and centrally located.^10^ In vascular compression, depending on the site and severity of obstruction, they can present with inspiratory, expiratory, or biphasic low-pitched sounds.^12^
This study also explored several risk factors for AAs, including dysmorphism, prematurity, and genetic syndromes. Prematurity emerged as a statistically significant factor, affecting 23% of AA cases versus 8.9% of controls (OR: 3.2). This finding aligns with a Taiwanese study reporting an odds ratio of 1.9 for airway anomalies in premature infants undergoing CHD surgery.^13^ Immature airway architecture in premature infants predisposes them to both malacia and extrinsic compressions. Additionally, prolonged neonatal intubation in this group may increase the risk of acquired abnormalities such as subglottic stenosis or airway malacia.^6^ The relatively high rate of subglottic stenosis observed in our cohort may be partially explained by these factors.
Previous studies have also reported an elevated risk of laryngotracheal anomalies—including subglottic stenosis and vocal cord palsy—among children with CHD.^1415^ Dysmorphism was present in 39% of AA cases and 32% of controls (odds ratio: 1.35). A genetic syndrome or diagnosis was identified in 34.6% of children with AAs, with Down syndrome being the most frequent (11.5%). These observations are consistent with reports showing increased risk of upper and lower airway anomalies in children with Down syndrome, owing to midfacial hypoplasia and related malformations such as laryngomalacia, tracheomalacia, and tracheobronchial anomalies.^161718^
Consanguineous marriage is highly prevalent in Oman. National-level surveys indicate an overall consanguinity rate that ranges from 36% to 49%.^1920^ Rajab A et al reported that 24.1% of marriages are between first cousins and 11.8% are between second cousins.^19^ Parental consanguinity, especially first-cousin unions, has been shown to be a significant risk factor for various congenital heart diseases, particularly associated with septal defects.^212223^ In addition, a systematic review showed that familial congenital laryngotracheal stenosis is higher among products of consanguineous marriage, although the quality of evidence is low.^24^ To date, no published study has shown that consanguinity is a risk factor for AA among children with congenital heart disease. The high prevalence of consanguinity among children with CHD and children with congenital laryngotracheal stenosis makes this link theoretically possible. In our study, data on consanguinity were not obtained so this link was not analysed.
The mean duration of invasive ventilation was significantly longer among cases compared to controls. This finding aligns with previous reports indicating prolonged intubation and ventilation in children with both congenital cardiac/vascular anomalies and AAs.^61325^ Early identification of AAs is therefore essential for optimising preoperative planning and minimising respiratory complications.^2627^
In our cohort, vascular-pexy was the most frequently performed intervention (14.3%), followed by tracheostomy (7.8%) and combined airway surgery with tracheostomy (3.9%). This differs from other studies reporting a higher rate of tracheostomy (up to 50%), likely due to differences in the underlying types of AAs; our cohort had a higher prevalence of vascular compressions, whereas others had more cases of tracheobronchomalacia.^4^
This study has several limitations. As a retrospective study, it is susceptible to missing data, particularly for patients who continued follow-up at other institutions. Additionally, the assumption that all control patients were free of AAs due to the absence of symptoms may not be entirely accurate, as some AAs can be asymptomatic and only identified through imaging performed for other reasons. Despite these limitations, the study contributes important epidemiological insights into AAs in children with CHD in Oman and underscores the importance of early diagnosis and multidisciplinary planning.
5. Conclusion
This study identified a higher-than-expected prevalence of airway abnormalities in children undergoing surgery for congenital heart disease, highlighting the need for heightened clinical vigilance, early detection, and structured postoperative follow-up. Future research should focus on larger prospective studies to refine diagnostic strategies, evaluate the impact of early intervention, and assess long-term outcomes in this population.
Authors' Contribution
Fatma Al Kindi: Conceptualization, Methodology, Data Curation, Writing - Original Draft, Visualization. Rand Al Harthy: Conceptualization, Methodology, Data Curation, Writing - Original Draft, Visualization. Saif A. Thani: Conceptualization, Methodology, Formal analysis, Validation, Writing - Review & Editing, Visualization. Hamood Al Kindi: Conceptualization, Methodology, Resources, Writing - Review & Editing. Hussain Mohsin: Conceptualization, Methodology, Validation, Writing - Review & Editing, Visualization, Supervision.
Acknowledgement
The authors would like to acknowledge Dr. Pranav Subbaraya Kandachar for his assistance with data collection and maintenance.
Ethics Statement
Ethical approval was obtained from the Royal Hospital Scientific Research Committee (Ethical approval No. SRC#27/2022).
Conflict of Interest
The authors declare no conflicts of interest.
Funding
No funding was received for this study.
Data Availability
Data is available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Van der Linde D Konings EE Slager MA Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol 2011; 58:2241–7. https://doi.org/10.1016/j.jacc.2011.08.025.10.1016/j.jacc.2011.08.02522078432 · doi ↗ · pubmed ↗
- 2R Subramanyan Joy JP Venugopalan A Sapru Khusaiby al Incidence and spectrum of congenital heart disease in Oman. Ann Trop Paediatr 2000; 20:337–41. https://doi.org/10.1080/02724936.2000.11748155.10.1080/02724936.2000.1174815511219172 · doi ↗ · pubmed ↗
- 3Lee YS Jeng MJ Tsao PC Soong WJ Chou P Prognosis and Risk Factors for Congenital Airway Anomalies in Children with Congenital Heart Disease: A Nationwide Population-Based Study in Taiwan. P Lo S One 2015; 10:e 0137437. https://doi.org/10.1371/journal.pone.0137437.10.1371/journal.pone.013743726334302 PMC 4559478 · doi ↗ · pubmed ↗
- 4Chen Q Langton-Hewer S Marriage S Hayes A Caputo M Pawade A Influence of Tracheobronchomalacia on Outcome of Surgery in Children With Congenital Heart Disease and Its Management. Ann Thor Surg 2009; 88:1970–4. https://doi.org/10.1016/j.athoracsur.2009.08.039.10.1016/j.athoracsur.2009.08.03919932270 · doi ↗ · pubmed ↗
- 5Riggs KW Zafar F Jacobs ML Tracheal surgery for airway anomalies associated with increased mortality in pediatric patients undergoing heart surgery: Society of Thoracic Surgeons Database analysis. J Thorac Cardiovasc Surg 2021; 161:1112–21.e 7. https://doi.org/10.1016/j.jtcvs.2020.10.149.10.1016/j.jtcvs.2020.10.14933419543 · doi ↗ · pubmed ↗
- 6Guillemaud JP El-Hakim H Richards S Chauhan N Airway Pathologic Abnormalities in Symptomatic Children With Congenital Cardiac and Vascular Disease. Arch Otolaryngol Head Neck Surg 2007; 133:672–2. https://doi.org/10.1001/archotol.133.7.672.10.1001/archotol.133.7.67217638780 · doi ↗ · pubmed ↗
- 7Chen T Qiu L Zhong L Tao Q Liu H Chen L Flexible bronchoscopy in pulmonary diseases in children with congenital cardiovascular abnormalities. Exp Ther Med 2018; 15:5481–6. 10.3892/etm.2018.6113.29904428 PMC 5996711 · doi ↗ · pubmed ↗
- 8An HS Choi EY Kwon BS Kim GB Bae EJ Noh CI Airway Compression in Children With Congenital Heart Disease Evaluated Using Computed Tomography. Ann Thorac Surg 2013; 96:2192–7. https://doi.org/10.1016/j.athoracsur.2013.07.016.10.1016/j.athoracsur.2013.07.01624070697 · doi ↗ · pubmed ↗