Giant cell tumor of bone in the mandible presenting without typical histological features: a case report
Kaori Oya, Kouhei Kawamura, Ryou Akiyama, Hiroki Kiyokawa, Toshihiro Uchihashi, Hiroaki Shimamoto, Tadashi Sasai, Shin-Ichiro Hiraoka, Shumei Murakami, Satoru Toyosawa

TL;DR
A rare case of giant cell tumor of bone in the jaw was diagnosed using a specific marker, H3.3G34W, despite lacking typical histological features.
Contribution
Demonstrates the utility of H3.3G34W immunostaining in diagnosing atypical giant cell tumor of bone in the jaw.
Findings
The tumor lacked conventional histological features of giant cell tumor of bone.
H3.3G34W positivity confirmed the diagnosis despite atypical morphology.
Giant cell tumor of bone can occur in the jaw, though it is rare.
Abstract
Giant cell tumor of bone is a locally aggressive bone tumor characterized by the proliferation of round-to-oval mononuclear cells and uniformly distributed osteoclast-type giant cells. Giant cell tumor of bone typically arises in long bones, whereas craniofacial involvement is rare. Atypical histological and clinical presentations can complicate diagnosis. This study presents a challenging case of giant cell tumor of bone in the mandible. A Japanese man in his 70s presented with a slowly expanding radiolucent lesion in the left mandible, first noted a decade ago, with no subjective symptoms. Cone-beam computed tomography revealed a 27 mm × 12 mm × 23 mm radiolucent lesion with irregular borders and discontinuity of the mandibular canal. Excisional biopsy showed the proliferation of bland spindle cells with small multinucleated cells, which indicated central giant cell granuloma.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
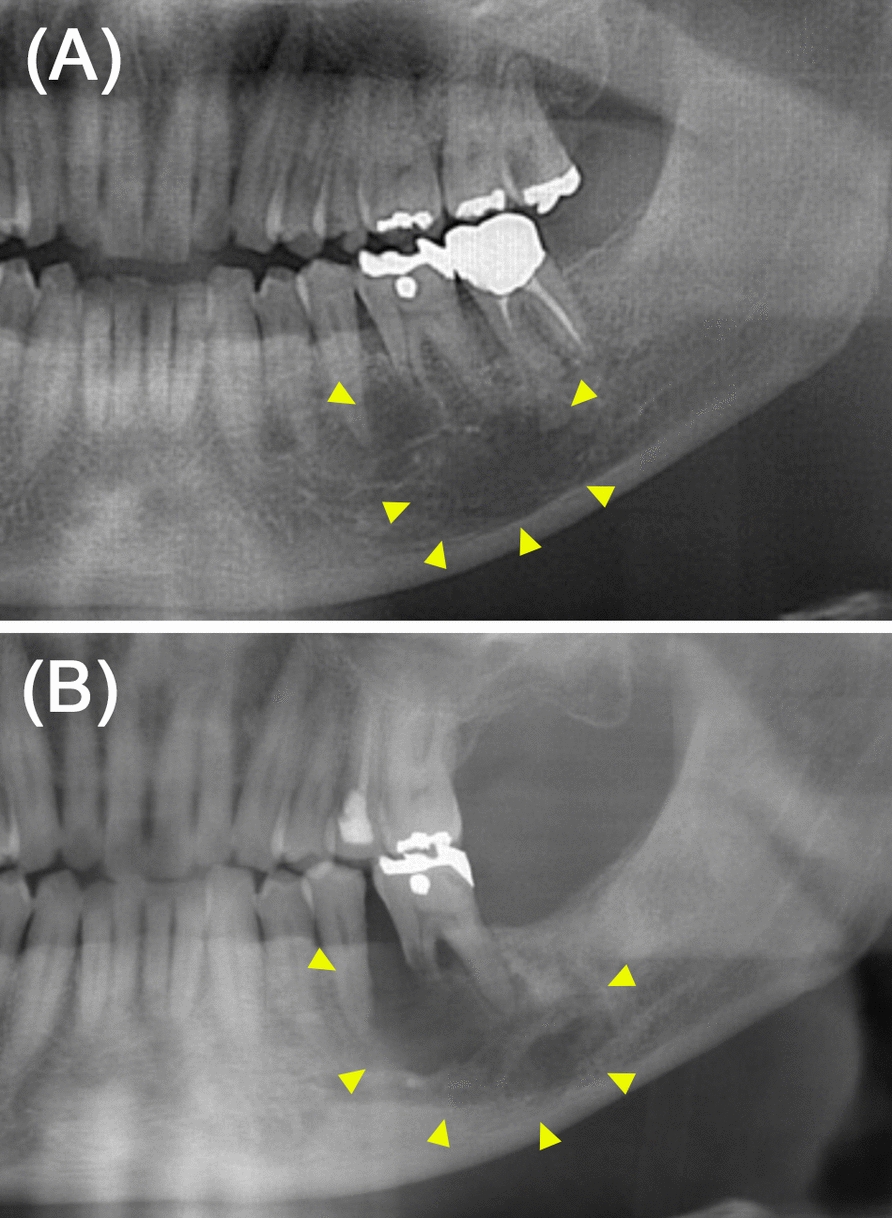 Figure 1
Figure 1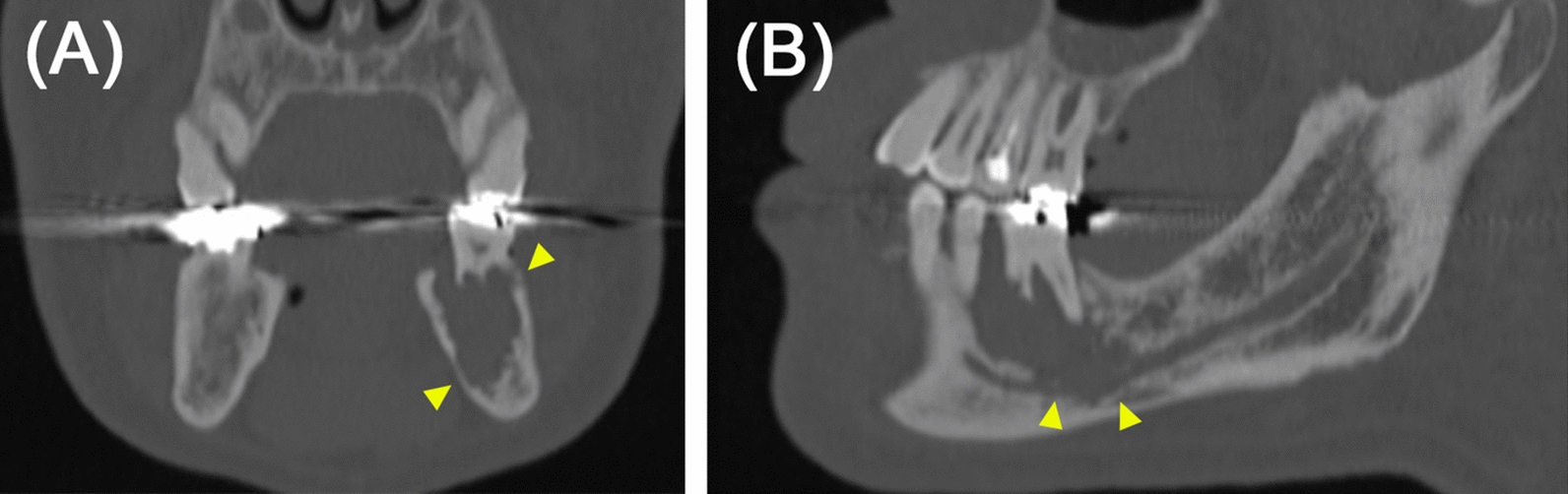 Figure 2
Figure 2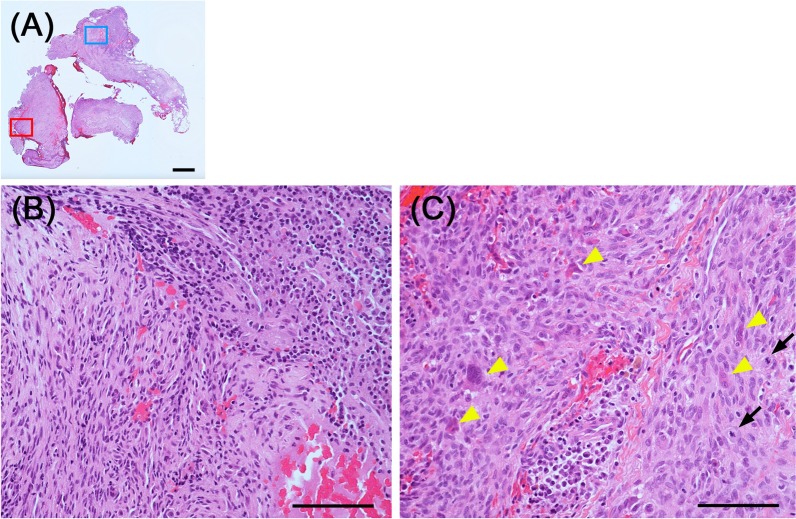 Figure 3
Figure 3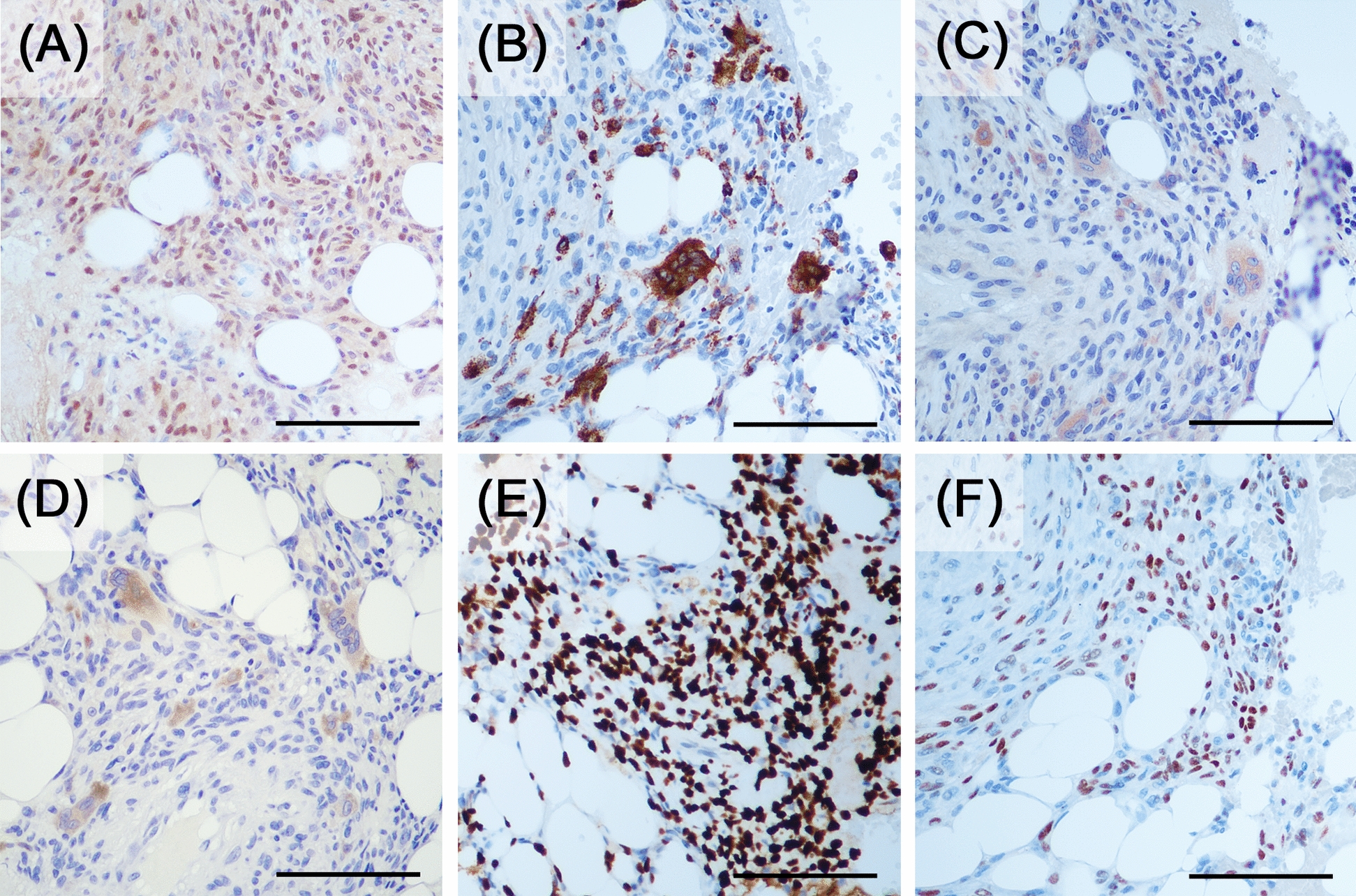 Figure 4
Figure 4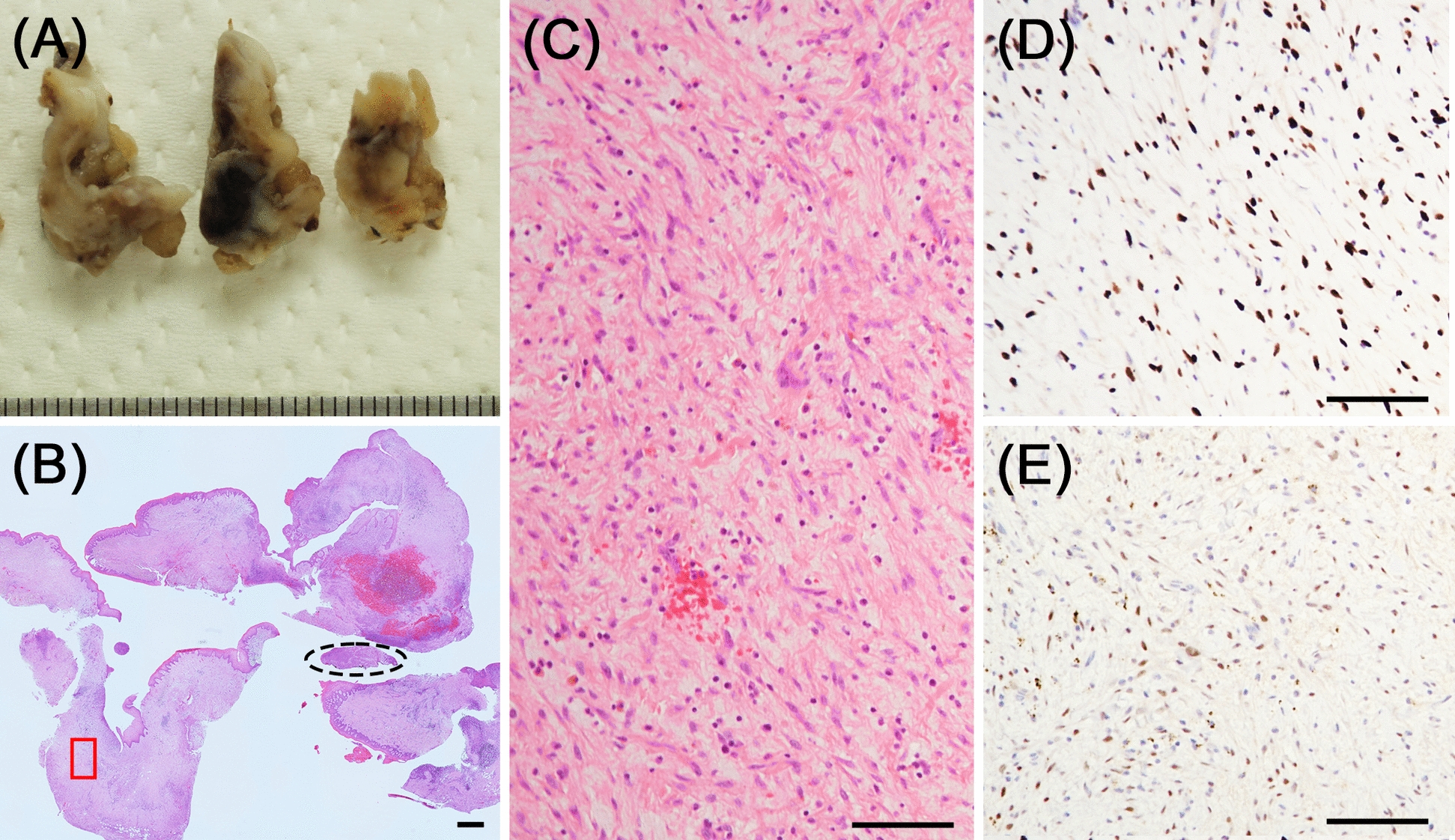 Figure 5
Figure 5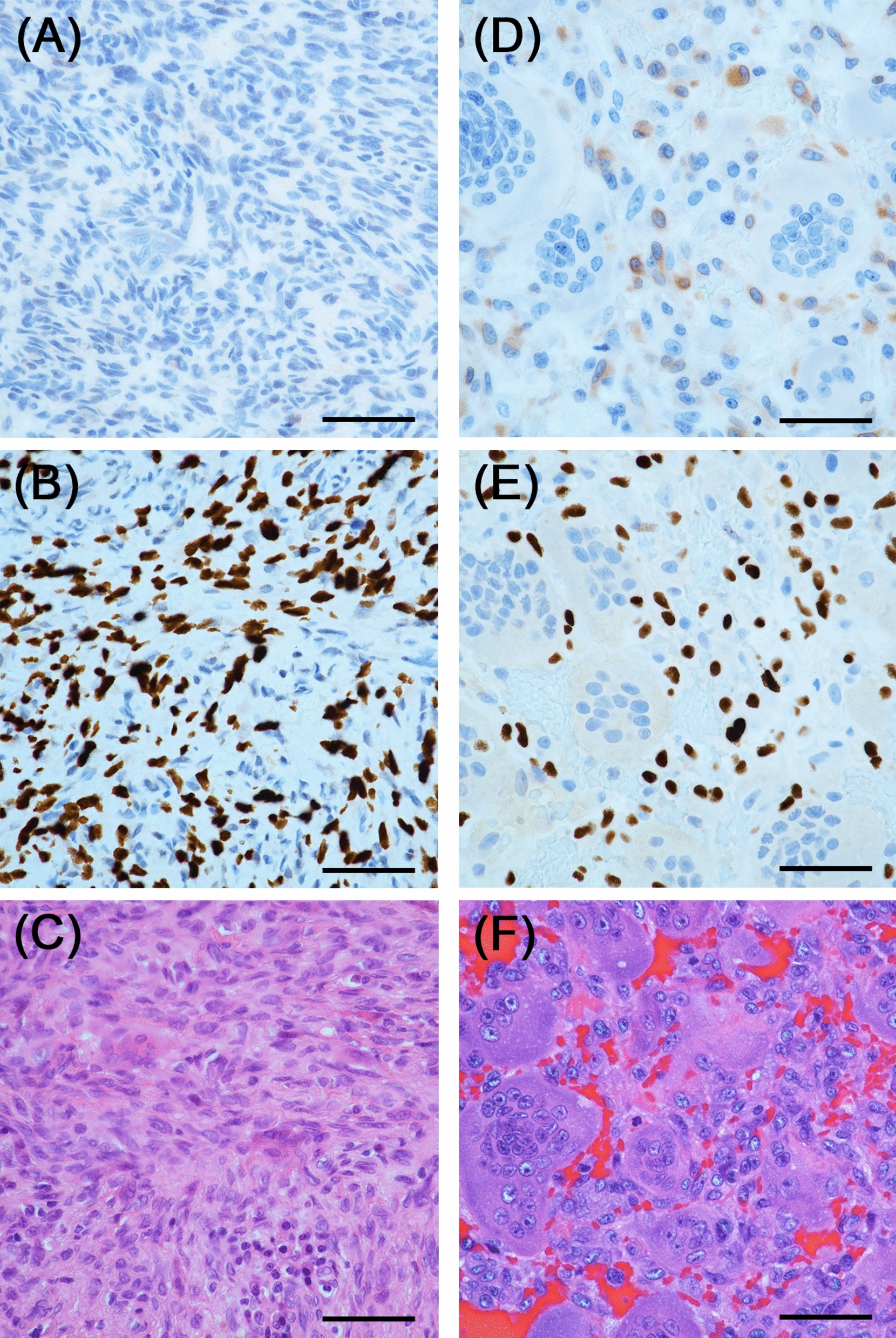 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone Tumor Diagnosis and Treatments · Oral and Maxillofacial Pathology · Sarcoma Diagnosis and Treatment
Background
Giant cell tumor of bone (GCTB) is a locally aggressive, intermediate malignancy of the bone, characterized by the proliferation of round-to-oval mononuclear cells and uniformly distributed osteoclast-type giant cells with numerous (50–100) nuclei [1, 2]. The neoplastic mononuclear cells of GCTB highly express the receptor activator of nuclear factor kappa B (RANK) ligand (RANKL), which binds to RANK expressed on mononuclear osteoclast precursors. The RANK–RANKL interaction results in giant cell formation and the osteolytic nature of the tumor [3]. GCTB represents 4–5% of all primary bone tumors, with a peak incidence in individuals of 20–45 years of age [1, 4]. The tumor typically arises at the ends of long bones in the mature skeleton, and craniofacial skeleton involvement is rare [1, 2, 5, 6].
Along with the classic GCTB morphology, atypical morphological patterns include fibrosis, bone or cartilage formation, cystic changes, necrosis, and secondary aneurysmal bone cyst (ABC) formation. Mitoses ranging from 0 to 35 per ten high-power fields have been observed [5, 7]. Additionally, the disease can occur in diverse age groups. Previous studies indicate that GCTB occurs in 8.9% of patients younger than 18 years and 4.8% of those older than 55 years [5, 7]. Moreover, case reports of craniofacial skeleton involvement exist, albeit with rarity or information deficiency [8–10]. Diagnostic challenges may arise when GCTB without typical and classical histological features develops at unusual sites or in uncommon age groups. Herein, we present a challenging case of GCTB involving the mandible.
Case presentation
A Japanese man in his 70s presented to our hospital for a close examination of an expanding radiolucent lesion in the left mandible, first noted approximately a decade ago, with no symptoms (Fig. 1). His medical history included hypertension, gout, and hyperlipidemia, for which he was on medication. Cone-beam computed tomography (CBCT) revealed a radiolucent lesion measuring 27 mm × 12 mm × 23 mm with an irregular border and discontinuity of the mandibular canal (Fig. 2). His serum level of the squamous cell carcinoma antigen was elevated at 3.4 ng/mL (1.5 ng/mL). These findings suggest the possibility of a primary intraosseous carcinoma; however, a prolonged course and absence of symptoms were unsupportive for this diagnosis. Extraction of the affected first molar and excisional biopsy were performed. Hematoxylin and eosin (HE)-stained sections of the biopsied specimens showed that most of the tissue consisted of inflammatory granulation tissue with hemorrhage (Fig. 3A, B). However, the proliferation of the spindle cells with small multinucleated cells was also observed (Fig. 3C). Cellular atypia was absent in spindle cells, and a few mitoses were also observed (two per ten high-power fields). Central giant cell granuloma (CGCG) was the most likely diagnosis because of the histology and site of origin, although the possibility of reactive lesion was considered due to the high proportion of granulation tissue. The differential diagnosis also included ABC because of its histological similarities and hemorrhagic properties. Although GCTB was considered unlikely because its occurrence in the craniofacial skeleton is quite rare, it was listed to be ruled out because the histological findings of the present case were similar to one of the histological variants of GCTB.Fig. 1. Comparison of panoramic radiographs. Panoramic radiographs taken A 10 years ago at the family dental clinic and B during the first visit to this hospital. The unclear radiolucent lesion around the root apex of the left first molar of the mandible (A, arrowhead) became clear with medial root absorption of the first molar (B, arrowhead)Fig. 2. Imaging findings of the primary lesion. Coronal cone-beam computed tomography image shows a radiolucent lesion with an irregular border and no expansion of the cortical bone (A, arrowhead). Sagittal cone-beam computed tomography image shows the disappearance of the mandibular canal wall (B, arrowhead)Fig. 3. Histological findings of the biopsied specimen. A Low magnification image of the hematoxylin and eosin-stained specimen (2× magnification). B High magnification image of the blue box in (A). It consisted mainly of inflammatory granulation tissue with hemorrhage. C High magnification image of the red box in (A). The proliferation of spindle cells with small multinucleated cells (arrowhead) was observed. Cellular atypia was absent in the spindle cells. Two mitoses (arrow) were observed (20× magnification). Scale bar: (A) 1000 μm, (B) and (C) 100 μm
Spindle cells were positive for runt-related transcription factor 2 (RUNX2), a marker of osteogenesis. Low proliferative activity was confirmed using Ki-67 immunostaining (< 3%). The small multinucleated cells were positive for cluster of differentiation 68 (CD68), tartrate-resistant acid phosphatase (TRAP), and cathepsin K, which are markers of osteoclasts. These results were consistent with the characteristics of CGCG. However, the spindle cells were also positive for H3.3G34W and p63, which are markers of GCTB (Fig. 4). Therefore, a final diagnosis of GCTB was establishedFig. 4Immunohistochemical staining results. (A) RUNX2, (B) CD68, (C) TRAP, (D) cathepsin K, (E) H3.3G34W, and (F) p63 (20× magnification). Scale bar: (A–F) 100 μm
Under general anesthesia, curettage was performed, and the specimen was subjected to histopathological examination. After formalin fixation, the lesion appeared as a soft white mass with partial bleeding (Fig. 5A). Histological examination with HE staining revealed that the main component had a granulation tissue-like appearance (Fig. 5B, C). Spindle cell proliferation with high cellular density was observed in only a very small area (Fig. 5B). At first glance, it appeared that the lesion had not been scraped out; however, immunostaining for H3.3G34W and p63 revealed that most of the tissue consisted of tumor cells. Many fibroblast-like spindle cells in the granulation tissue-like area were positive for them (Fig. 5C–E). Typical histological features of GCTB were not observed.Fig. 5. Gross appearance and histological findings of the resected specimen. A Macroscopically, the lesion appeared as a white soft mass with partial bleeding. B Low magnification image of the hematoxylin and eosin-stained specimen. Spindle cell proliferation with high cell density was observed only in a very small area (dotted line frame) (2× magnification). C High magnification image of the red box in (B). The main component showed a granulation tissue-like appearance (10× magnification). D and E Immunohistochemical staining results for (D) H3.3G34W and (E) p63 corresponding to (C). Fibroblast-like spindle cells in the granulation tissue-like area were positive for them (10× magnification). Scale bar: (A) 1000 μm, (C) and (D) 100 μm
Follow-up CBCT examination at 18 months post-surgery showed no evidence of recurrence, and the patient showed satisfactory progress.
Discussion and conclusion
The recent finding of H3.3 histone A (H3F3A) gene mutations in 92% of GCTB cases [11] has improved GCTB diagnostic ease and certainty, with the detection of the mutated proteins H3.3G34W, G34R, and G34V using immunostaining [3]. Particularly, the usefulness of immunostaining for H3.3G34W, the most frequent variant, has been reported. A specificity and positive predictive value of 100% has been demonstrated [12], with sensitivities ranging from 85% to 90.6% [13, 14].
GCTB can typically be diagnosed through histological examination of the entire lesion site, as most GCTB cases exhibit conventional morphology, although several histological variants have been reported [5, 6]. A previous report of a GCTB lesion predominantly composed of spindle cells with no giant cell involvement was introduced in the Armed Forces Institute of Pathology atlases, although the patient was initially misdiagnosed as having benign fibrous histiocytoma [2]. Herein, we present a case of GCTB without typical histological features. In ours as well as in the previously reported case, immunohistochemical staining for H3.3G34W proved crucial for diagnosing GCTB. Similar to ours, other cases may be misdiagnosed due to the lack of typical features and examination for H3F3A gene mutations [2]. Therefore, H3.3G34W immunostaining should be performed even if the diagnosis is considered to be CGCG and others showing spindle cell proliferation. Although the reason why giant cells are less obvious in these cases remains undetermined, a reduction of RANKL expression is one possible reason. The presented case showed a significant reduction in RANKL positivity compared with typical GCTB cases in immunostaining (Fig. 6). Identifying similarities among such cases can help elucidate the mechanism.Fig. 6. Comparison of the present case (A–C) and typical giant cell tumor of bone case (D–F). A Receptor activator of nuclear factor kappa B ligand expression scarcely be observed in the present case, but (D) mononuclear cells in typical giant cell tumor of bone case clearly express receptor activator of nuclear factor kappa B ligand. B and E Immunostaining results for H3.3G34W and (C) and (F) hematoxylin and eosin-stained images corresponding to (A) and (D), respectively. (40× magnification). Scale bar: (A–D) 50 μm
H3F3A mutations or H3.3G34W immunopositivity have not been observed in giant cell lesions and bone cysts of the jaw [12, 14, 15], which supports the rarity of GCTB in the jawbone. However, our case report involved the incidence of GCTB in the mandible. The possibility of GCTB should not be ruled out on the basis of its site of occurrence, as GCTB can occur in any bone [3].
The most common differential diagnoses of giant cell lesion include CGCG, ABC, and non-ossifying fibroma (NOF), in addition to GCTB [1, 16]. Morphological similarities complicate diagnosis; however, immunohistochemical staining, genetic testing, and clinical information aid in achieving accuracy. Aside from H3.3G34W, other useful markers exist. p63 immunopositivity is observed in GCTB but not CGCG [17], although both share common features such as high RUNX2 expression [18]. As approximately 75% of ABC cases harbor a chromosomal translocation involving the USP6 gene with various fusion partners [19, 20], fluorescence in situ hybridization testing for USP6 rearrangements can be used for diagnosis. NOF exclusively arises in skeletally immature individuals, with a peak incidence in the second decade of life, and affects the metaphyses of long bones [1, 16]. Compatible imaging findings, including well-defined, lobulated radiolucent lesions centered in the cortical bone with sclerotic and scalloped borders, are essential for the diagnosis of NOF [1].
The standard treatment for GCTB is curettage [2], although recurrence has been observed in 15–50% of cases [1]. Wide resection is associated with a lower recurrence rate than intralesional surgery [21] but can cause significant morbidity [3]. Polymethylmethacrylate may reduce local recurrence risk [21]. Denosumab, an inhibitor of RANKL, may be considered for unresectable and advanced cases [1]. It suppresses bone resorption by inhibiting the formation of osteoclast-like giant cells by blocking the RANK–RANKL interaction. Hayashida et al. reported that local recurrence cannot be reduced by denosumab treatment [22]; however, no consensus regarding its use exists [1]. Denosumab changes the histomorphology of GCTB; complete elimination of osteoclast-like giant cells, fascicular and storiform patterns of spindle-shaped mononuclear cells, sometimes mixed with foam cells, and reticular woven bone formation, have been observed [23]. Thus, it is crucial to refer to clinical history in the diagnosis of such cases to prevent misidentification of other fibro-osseous lesions or spindle cell sarcoma [24]. In this case, only intralesional curettage was performed. As a risk of recurrence exists, we intend to follow up on the case closely.
In conclusion, we report a case of GCTB resembling CGCG of the mandible. Morphological analysis alone is insufficient for diagnosis; detecting H3F3A mutations or mutated proteins is essential. H3.3G34W immunostaining is valuable for distinguishing GCTB from other giant cell lesions in daily clinical practice. Although rare, GCTB should remain a differential consideration in jaw lesions.