Distance to Care and Telehealth Abortion Demand After Dobbs
Amy K. Willerford, Emily M. Godfrey, Caitlin Myers, Rebecca Gomperts, Erin K. Thayer, Anna Fiastro

TL;DR
This study looks at how the 2022 Dobbs decision affected the number of telehealth abortion requests in 18 US states.
Contribution
The study provides new insights into the impact of the Dobbs decision on telehealth abortion demand.
Findings
Telehealth abortion requests increased in states with restrictive abortion laws after the Dobbs decision.
Distance to care was a significant factor influencing telehealth abortion demand.
The study highlights the role of telehealth in addressing access barriers post-Dobbs.
Abstract
This cross-sectional study of public health data in 18 US states examines the change in telehealth medication abortion requests after the 2022 Dobbs v Jackson Women’s Health Organization Supreme Court decision.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
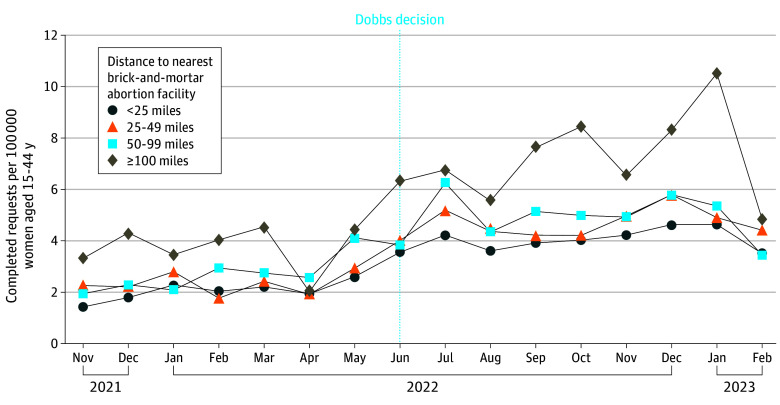 Figure 1
Figure 1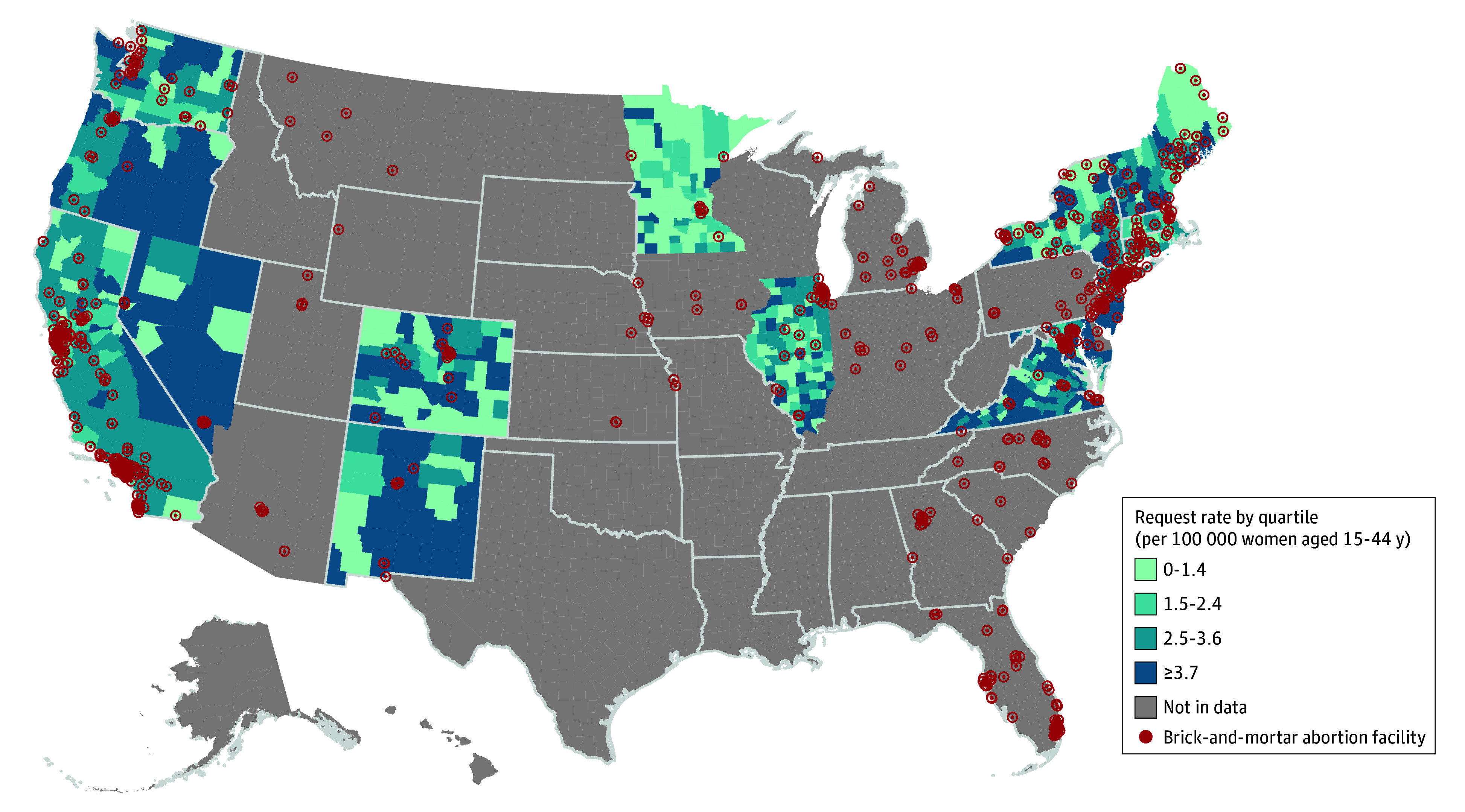 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTelemedicine and Telehealth Implementation · Healthcare Policy and Management
Introduction
Geographic distance has become an increasingly critical determinant of abortion access in the aftermath of the Supreme Court decision Dobbs v Jackson Women’s Health Organization.^1,2^ As distance increases, so do delays in care and the cost of accessing an abortion—factors that may eliminate access altogether.^2,3^ Many patients are turning to telehealth medication abortion (teleMAB) services, citing benefits including lower costs and eliminating travel.^2,4,5^
While the surge in teleMAB is well documented, the extent to which distance from a brick-and-mortar abortion clinic relates to this demand in states that permit abortion post-Dobbs remains unclear.^2,4,6^ We aim to characterize the changes in teleMAB requests before and after Dobbs and examine the association between request rates and distance to an abortion facility over the same period.
Methods
We conducted a repeated cross-sectional study to examine Aid Access asynchronous teleMAB service requests before and after Dobbs, stratified by distance to the nearest abortion facility. We used data from 18 states where teleMAB was legal 8 months before and after Dobbs to ensure comparability across jurisdictions and to minimize legal and reporting variability.
We calculated the number of teleMAB requests per county and month and determined distance to the nearest abortion facility using population-weighted county centroids from the Myers Abortion Facility Database. We used Housing and Urban Development United States Postal Service (HUD-USPS) zip code and county name data to match the Federal Information Processing Standards (FIPS) codes associated with patient records.
We described trends in completed teleMAB requests over time and used Poisson models with a quadratic distance specification to estimate the association between distance to the nearest brick-and-mortar facility and county-level per capita teleMAB requests, including an interaction term for time. We analyzed data using R version 3.6.1 (R Project for Statistical Computing) and StataIC (Stata Inc); this study followed Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines. The University of Washington Human Subjects Division determined this study did not require review or informed consent because it did not involve human participants.
Results
Between November 2021 and February 2023, Aid Access completed 16 154 teleMAB requests across 18 states and 743 counties. Individuals had a median (IQR) age of 26 (22-31) years and most were less than 6 weeks pregnant (9557 [59.2%]) and had no children (9495 [58.8%]). There were 4545 requests pre-Dobbs, and 11 609 after. The average monthly teleMAB request rate rose across all counties post-Dobbs, from 2.4 to 4.5 requests per 100 000 women aged 15 to 44 years per month (Figure 1). On average, this rate increased the further individuals lived from brick-and-mortar facilities (Figure 2). The teleMAB request rate tended to be highest in counties located 100 miles or more from an abortion facility both before and after Dobbs. A 100-mile increase in distance was associated with a 13% increase in requests per capita (95% CI, 7% to 19%) pre-Dobbs and an 8% increase (95% CI, 3% to 13%) post-Dobbs; these increases are not statistically different from one another (−5.5%; 95% CI, −25.6% to 4.5%; P = .59).
US County-Level Trends in Completed Telehealth Medication Abortion Service Requests by Distance to the Nearest Brick-And-Mortar Abortion FacilityVertical line indicates the Dobbs v Jackson Women's Health 2022 Supreme Court decision.
Average Monthly Completed Telehealth Medication Abortion Service Request Rate by US County Between November 2021 and February 2023Red markers indicate the locations of brick-and-mortar abortion facilities as recorded in the Myers Abortion Facility Database.
Discussion
Overall, we observed a doubling in monthly teleMAB requests across 18 states post-Dobbs, with most requests occurring before 6 weeks of pregnancy and the highest rates among individuals living further from in-person abortion care. These results build upon our findings pre-Dobbs, which also demonstrated increased teleMAB requests among individuals living further from brick-and-mortar facilities.^2^
An important study limitation is the reliance on data from states where abortion remained legal post-Dobbs, which may have included persons traveling from restricted states for care. Still, our findings align with growing evidence that teleMAB is essential for those living far from in-person care, and its availability enables individuals to receive treatment at early gestations, thereby reducing complications that can occur with delayed care.^4,6^
The loss of federal abortion protections has significantly disrupted access even in states with robust service provision.^1^ Our results highlight the critical role of teleMAB in reducing geographic barriers to care and underscore the need to expand teleMAB access nationwide.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rader B, Upadhyay UD, Sehgal NKR, Reis BY, Brownstein JS, Hswen Y. Estimated travel time and spatial access to abortion facilities in the US before and after the Dobbs v Jackson Women’s Health decision. JAMA. 2022;328(20):2041-2047. doi:10.1001/jama.2022.2042436318194 PMC 9627517 · doi ↗ · pubmed ↗
- 2Godfrey EM, Fiastro AE, Thayer EK, Gomperts R, Orlando SM, Myers CK. No-test telehealth medication abortion services provided by US-based clinicians in 21 states and the District of Columbia, 2020–2022. Am J Public Health. 2025;115(2):221-231. doi:10.2105/AJPH.2024.30789239778139 PMC 11715571 · doi ↗ · pubmed ↗
- 3Myers CK, Dench DL, Pineda-Torres M. The road not taken: how driving distance and appointment availability shape the effects of abortion bans. National Bureau of Economic Research. National Bureau of Economic Research working paper No. 33548. March 2025. Accessed June 8, 2025. https://www.nber.org/papers/w 33548
- 4Fiastro AE, Zheng Z, Ruben MR, Gipson J, Godfrey EM. Telehealth vs in-clinic medication abortion services. JAMA Netw Open. 2023;6(9):e 2331900. doi:10.1001/jamanetworkopen.2023.3190037656461 PMC 10474522 · doi ↗ · pubmed ↗
- 5Biggs MA, Schroeder R, Kaller S, Grossman D, Scott KA, Ralph LJ. Changes in support for advance provision and over-the-counter access to medication abortion. JAMA Netw Open. 2025;8(1):e 2454767. doi:10.1001/jamanetworkopen.2024.5476739820693 PMC 11739987 · doi ↗ · pubmed ↗
- 6Society of Family Planning. #We Count Report: April 2022 to June 2024. Published online October 22, 2024. Accessed June 8, 2025. doi:10.46621/728122 kflzwf · doi ↗