Prevalence of posttraumatic stress symptoms among physicians – A meta-analysis
Jana Reinhardt, Katja Linde, Anette Kersting

TL;DR
This study finds that about 15% of physicians experience PTSD symptoms, with higher rates in middle-income countries and depending on the tools used for measurement.
Contribution
The paper provides a meta-analysis of PTSD prevalence among physicians, identifying regional and measurement tool differences.
Findings
The pooled PTSD prevalence among physicians was 14.9%, higher than general population estimates.
Prevalence was higher in middle-income countries (21.1%) compared to high-income countries (13.6%).
Shorter screening tools reported lower PTSD prevalence (10.2%) than longer instruments (16.4%).
Abstract
The medical profession is associated with high demands and occupational stressors – including confrontation with illness and death, extended work hours, and high workload – which may increase the risk of traumatization and posttraumatic stress disorder (PTSD). This systematic review aimed to synthesize evidence on prevalence of PTSD among physicians and examine potential moderators, including the COVID-19 pandemic, specialties, and geographic regions. A systematic search was conducted in PubMed, Web of Science, PsychINFO, and PubPsych up to April 2025. Included studies were English-language, peer-reviewed, observational studies, reporting PTSD prevalence in physicians, using validated instruments. Studies focusing on preselected PTSD cases or mixed healthcare samples were excluded. Data extraction included study methodology, measurement tools, geographic region, specialty, and survey…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
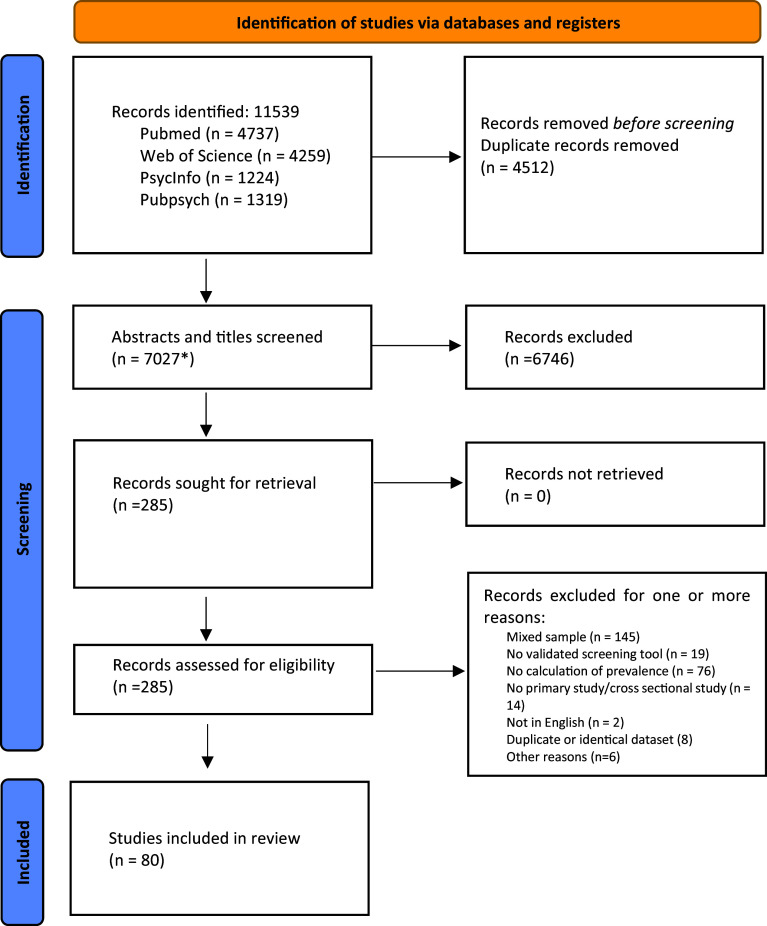 Figure 1
Figure 1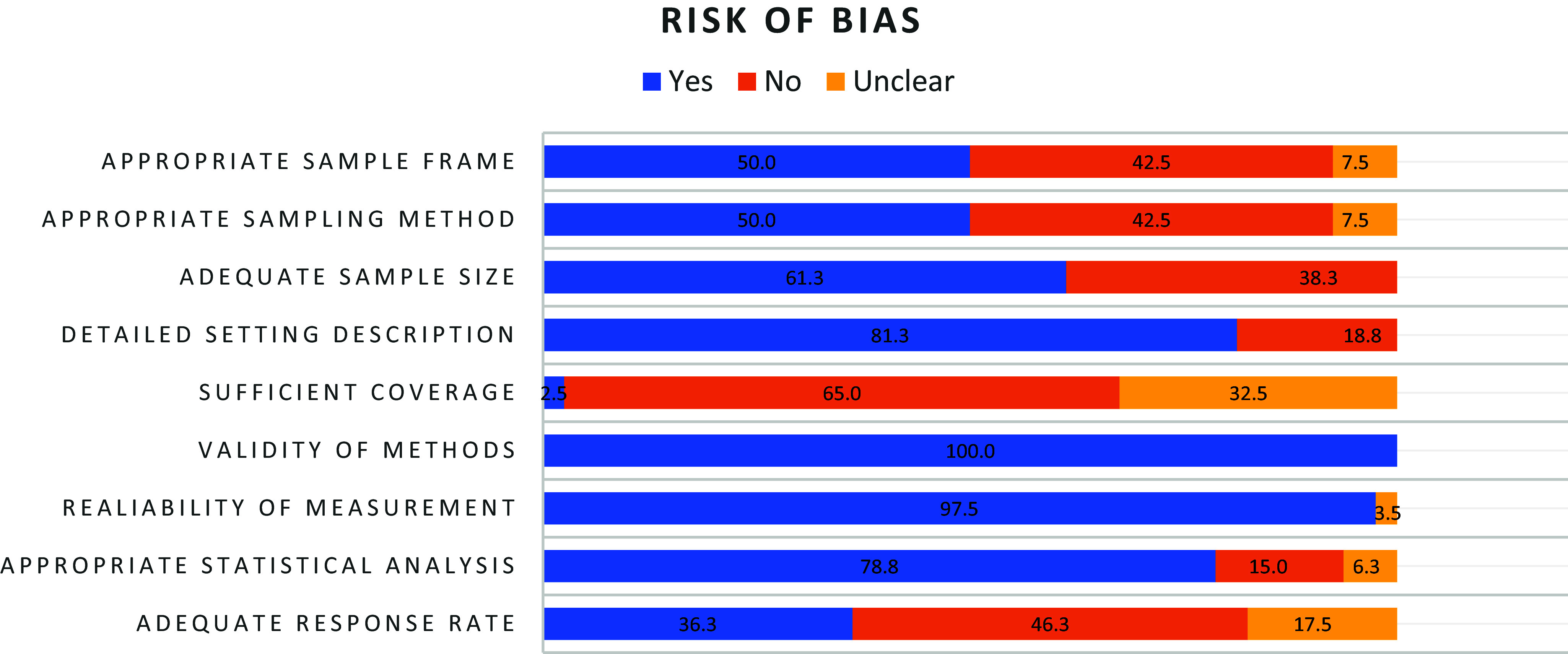 Figure 2
Figure 2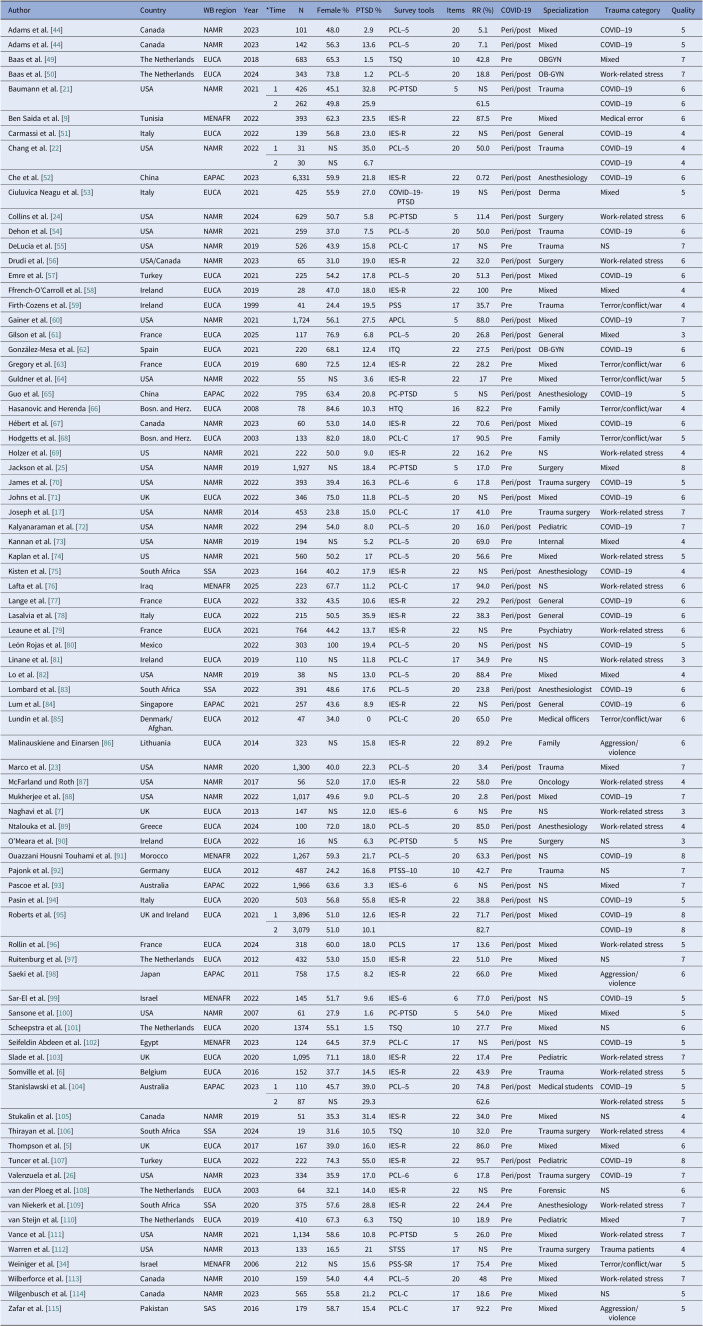 Figure 3
Figure 3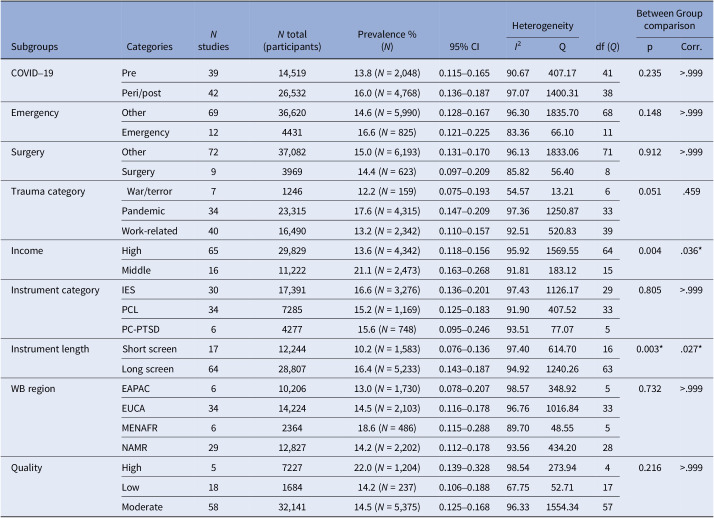 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare professionals’ stress and burnout · Posttraumatic Stress Disorder Research · COVID-19 and healthcare impacts
Theoretical background
Mental health among physicians
The medical profession is associated with high psychological demands, which can have an impact on mental health [1, 2]. Structural stress factors include long, irregular working hours and increasing pressure to perform at a high level at work [3, 4]. High demands – such as excellence and compassion – are inherent in the culture of medicine leading to personal stress factors, that is, an excessive drive for perfection and a sense of responsibility [4, 3].
One occupational stress factor for physicians is an increased risk of experiencing trauma due to constant exposure to suffering, illness, or death [5, 6]. Increased risk of infection [7], experiencing violence [8], and medical errors [9] can also have a traumatizing effect [10, 11].
A common psychological consequence of experiencing trauma is the development of posttraumatic stress disorder (PTSD). According to the DSM-5 [12], PTSD occurs after direct or indirect exposure to a traumatic event (Criterion A) and is characterized by four symptom clusters – intrusion (Criterion B), avoidance (Criterion C), negative alterations in mood and cognition (Criterion D), and hyperarousal (Criterion E) [12]. Meta-analytical data [13] indicate a PTSD prevalence of 14.8% among physicians compared to 3.9% in the general adult population [14]. Individuals who experience significant symptoms of posttraumatic stress may suffer functional impairment [15, 16]. Impaired performance may increase the risk of medical errors [17], creating a cycle in which errors raise the likelihood of traumatic events [18], which in turn exacerbates the distress [19].
Moderators
Various structural factors within the healthcare system may increase the risk of posttraumatic stress disorder among physicians.
One occupational risk is that certain medical specialties, particularly emergency and trauma care, heighten exposure to traumatic situations, such as accidents, serious injuries, and delivering bad news. While some studies suggest no difference in PTSD prevalence between trauma and nontrauma physicians [20], other studies report rates as high as 22–35% in emergency physicians [21–23], indicating a higher degree of vulnerability for the development of PTSD in this group.
Similar to emergency physicians, surgeons encounter difficult and unusual situations on a daily basis [17, 24]. Medical errors in the operating room can have far-reaching, often life-threatening consequences. Therefore, the surgical profession involves a high degree of pressure and responsibility, which makes surgeons similarly susceptible to developing PTSD [17, 25, 26].
Studies suggest that the type of traumatic event can significantly influence the degree of psychological impact and the likelihood of developing PTSD [27, 28]. For example, Guina et al. [28] found that individuals exposed to combat-related trauma exhibited higher levels of posttraumatic stress symptoms. Accordingly, physicians working in conflict regions – particularly those exposed to war or terrorism – may also be at increased risk of developing more severe PTSD symptoms.
The data collection location may also moderate the occurrence of PTSD among physicians. Evidence concerning trauma exposure is inconclusive with some studies reporting a higher trauma exposure and also PTSD prevalence in high-income countries compared to low-income countries [14], others indicating that trauma exposure is higher in low-income countries [29]. In addition, considerable disparities exist in the quality of healthcare systems [18]. These differences may impact job satisfaction, workload, and stress levels among healthcare workers, subsequently affecting their health [30]. PTSD rates among physicians may therefore be higher in countries with a lower healthcare quality and a greater general trauma exposure.
Finally, the COVID-19 pandemic has posed a significant burden on the physical and mental health of healthcare professionals [31]. Increased infection risk, extended working hours due to higher sick leaves, and quarantine during the pandemic are just a few psychological challenges faced by physicians, making them potentially vulnerable to mental disorders such as anxiety, insomnia, depression, and PTSD symptoms [32].
The present study
The current meta-analysis aims to synthesize findings on posttraumatic stress symptoms among physicians. Earlier meta-analytical data [13] indicate that the prevalence of PTSD is higher among physicians (14.8%) than in the general adult population (3.9%) [14]. The meta-analysis by Sendler et al. included studies up to 2014 and faced some methodological limitations. For instance, it did not report key statistical details such as confidence intervals or standard deviations, and it only mentioned the percentage of the population affected by PTSD without specifying the sample size. The search string, coding, and statistical tests used to address subgroup differences were somewhat limited, and the analysis lacked a quality rating of the studies. Notably, one of the included papers [33] was based on the same dataset as another study [34].
Additionally, the meta-analysis of Sendler et al. only included studies using the PTSD Checklist (PCL) [35]. Our study aims to include all research employing standardized and validated screening tools, as we did not expect differences in outcomes based on the screening tool [36]. In addition to the type of instrument, we also considered the length of the screening tool as a potential moderator, as findings reported that shorter instruments performed comparably to longer ones in terms of diagnostic accuracy [36].
While the study by Sendler et al. provides valuable insights, it serves more as a narrative review with some methodological limitations rather than a comprehensive systematic meta-analysis. This underscores the need for an updated evaluation of the prevalence of PTSD among physicians.
Beyond the update prompted by methodological limitations in Sendler et al. [13], a further update on the prevalence of PTSD is necessary due to changes and challenges in the global healthcare system since 2020. Recent meta-analyses have summarized the incidence of mental health problems, particularly PTSD, in healthcare professionals in general [37–40]. To our knowledge, this is the first meta-analysis that directly compares the prevalence of PTSD solely among physicians before and during/“after” the pandemic.
We will also explore the potential moderating factors that may influence the prevalence of PTSD among physicians. We hypothesize that the prevalence during/“after” the pandemic is higher than before 2020. Additionally, we expect that emergency physicians or surgeons will exhibit a higher prevalence of PTSD compared to physicians working in other specialties. Furthermore, we expect differences based on the type of trauma, with physicians affected by war and terrorism showing higher PTSD prevalence rates. We also anticipate differences in PTS prevalence by region, with lower rates in high-income countries compared to low-income countries. We did not expect any differences in prevalence in different screening tools or systematic differences related to instrument length either.
Method
This meta-analysis was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) [41–43]. It was registered with PROSPERO (ID CRD42023401984).
Search strategy and screening procedure
From September 2023 until April 22, 2025, a systematic search of the databases PubMed, Web of Science, PsychINFO, and PubPsych was conducted, including relevant papers published up to the search date. A search string was applied to the search engines of each database searching in title and/or abstract. The search string was composed of terms including (PTSD OR PTS OR posttrauma* OR post-trauma*) AND (doctors OR physicians OR “medical practitioners” OR surgeons). The full list of search terms is included in the supplementary material (see Supplements A).
Duplicates were removed and titles and abstracts were screened by two independent authors. A full-text screening of all remaining articles was conducted by JR, second rater KL screened 25% of the remaining articles. Discrepancies were resolved by discussion. Cohen’s Kappa interrater reliability was calculated for both abstract and full-text screening.
Eligibility criteria
Studies were included if they fulfilled the following criteria: (a) empirical observational study, published in a peer-reviewed journal, (b) studies published in English, (c) studies assessing PTS or PTSD in practising physicians or trainee doctors, (d) PTS/PTSD is assessed via self-report, screening tool, or diagnostic interview with standardized and validated instruments, and (e) studies provided sufficient information to extract or calculate the prevalence of PTSD in %. Prospective studies, including randomized controlled trials (RCT) and quasi-RCTs which included participants required to have preexisting PTSD symptoms, were excluded. Studies in which the study population was healthcare providers in general were excluded, due to missing information about statistical parameters for the subgroup of physicians.
Data extraction and aggregation
The following data were extracted from each included record: source (authors, year of publication), sample size (N), demographic characteristics of each sample (age, gender), study design, time point and country/region of data collection, the prevalence of PTSD, medical specialty, level of training, work environment, type of traumatic event, an instrument to measure PTSD (including cut-off values), and if available, other reported health outcomes. If prevalence rates were not reported in percentages, they were calculated by dividing the number of individuals meeting the criteria for PTSD by the total sample size (N).
Longitudinal studies with multiple data points were treated as a single study with dependent datasets, combining the time points into one composite outcome score. A conservative approach was used, assuming a perfect correlation (1.0) between the data points. One longitudinal study was included in which the authors claimed that both time points were independent [44]. We treated these data as two separate studies.
For the pre-/post-COVID-19 pandemic subgroup division, data collected starting in 2020 were classified as postonset.
To identify subgroups based on regional and income characteristics we used the classification system of the World Bank Group, which categorizes income groups based on the World Bank Atlas Method (low-income, lower middle-income, upper middle-income, and high-income according to 2023 gross national income). Further classification by the World Bank Group is based on region. We used both classifications to test for moderating effects of region and income of countries on prevalence rates.
Additionally, we categorized the measurement instruments according to their length, based on the number of items (short screening tool ≤10 items; long screening tool >10 items).
Risk of bias
The Joanna Briggs Institute (JBI) critical appraisal checklist for studies reporting prevalence data [45] was used to assess the quality of each study. The checklist comprises nine questions, regarding sample frame and size, recruitment, study setting and subjects, response rate, validation and reliability, and statistical analysis (see Supplements B). Questions are answered with “yes,” “no,” or “unclear.” Subgroup analysis was performed based on the criteria met – a score of ≤4 indicating low quality, 5–7 indicating medium quality, and ≥8 indicating high quality. Quality ratings for each study were conducted by JR, the second rater, KL rated 25% of the articles. Discrepancies were resolved by discussion. Cohen’s Kappa was calculated to determine interrater reliability for the risk of bias assessment.
Statistical analysis
Data analysis was conducted using the statistical program Comprehensive Meta-Analysis (CMA) [46]. To assess the pooled prevalence of PTS symptoms, we performed a random-effects meta-analysis. This model was chosen to account for heterogeneity. Prevalence estimates were calculated with 95% confidence intervals. Statistical heterogeneity was evaluated using a Q test and I ^2^ statistics. Sensitivity analysis was performed by examining the relative weight of each study as well as performing a One-Study-Removed analysis.
We did not assess publication bias, as the central assumption – that statistically significant studies are more likely to be published – does not apply to cross-sectional studies reporting prevalence rates [47].
To examine the impact of the abovementioned moderators, subgroup analyses were performed, including only studies for which the relevant data were available. Subgroups were included in the analysis if at least five studies were available for that subgroup. Additionally, metaregressions were performed to account for potential moderating effects of gender (percentage of females) and publication year.
To address the issue of multiple testing in the subgroup analysis, Bonferroni correction was used to adjust for the false discovery rate [48].
Results
The literature search resulted in a total of 11,539 articles (see Figure 1). Of these, 4512 were duplicates and were removed. Of the remaining 7027 articles, abstracts and titles were screened; 285 were suitable for full-text screening, 80 were included in the meta-analysis.Figure 1.PRISMA 2020 flow diagram. Source: Page MJ, et al. BMJ 2021;372:n71. doi: 10.1136/bmj.n71.
Study characteristics
The analysis was based on 80 studies which met the eligibility criteria (see Table 1). Publication dates ranged from 1999 to 2025. Of these, 75 studies used a cross-sectional design, and 5 studies were longitudinal. One longitudinal study stated that its two measurement points were essentially independent datasets rather than a single longitudinal dataset [44]. In the analysis, we treated the results of this study as two independent effect sizes (N = 81 studies). The overall sample size was N = 41,051 (N = 45,011 for longitudinal data). In 42 studies, data were collected after the onset of the COVID-19 pandemic (2020). Nine studies focused on surgeons, while 12 studies examined emergency physicians. Specialties in the remaining studies were mixed. Four studies were from countries with a lower middle-income level, 12 studies were from countries with an upper middle-income level, and 65 studies were from high-income level countries.Table 1.Characteristics of included studiesAuthorCountryWB regionYear*TimeNFemale %PTSD %Survey toolsItemsRR (%)COVID-19SpecializationTrauma categoryQualityAdams et al. [44]CanadaNAMR202310148.02.9PCL–5205.1Peri/postMixedCOVID–195Adams et al. [44]CanadaNAMR202314256.313.6PCL–5207.1Peri/postMixedCOVID–195Baas et al. [49]The NetherlandsEUCA201868365.31.5TSQ1042.8PreOBGYNMixed7Baas et al. [50]The NetherlandsEUCA202434373.81.2PCL–52018.8Peri/postOB-GYNWork-related stress7Baumann et al. [21]USANAMR2021142645.132.8PC-PTSD5NSPeri/postTraumaCOVID–196226249.825.961.5COVID–196Ben Saida et al. [9]TunisiaMENAFR202239362.323.5IES-R2287.5PreMixedMedical error6Carmassi et al. [51]ItalyEUCA202213956.823.0IES-R22NSPeri/postGeneralCOVID–194Chang et al. [22]USANAMR2022131NS35.0PCL–52050.0Peri/postTraumaCOVID–194230NS6.7COVID–194Che et al. [52]ChinaEAPAC20236,33159.921.8IES-R220.72Peri/postAnesthesiologyCOVID–196Ciuluvica Neagu et al. [53]ItalyEUCA202142555.927.0COVID–19-PTSD19NSPeri/postDermaMixed5Collins et al. [24]USANAMR202462950.75.8PC-PTSD511.4Peri/postSurgeryWork-related stress6Dehon et al. [54]USANAMR202125937.07.5PCL–52050.0Peri/postTraumaCOVID–196DeLucia et al. [55]USANAMR201952643.915.8PCL-C17NSPreTraumaNS7Drudi et al. [56]USA/CanadaNAMR20236531.019.0IES-R2232.0Peri/postSurgeryWork-related stress6Emre et al. [57]TurkeyEUCA202122554.217.8PCL–52051.3Peri/postMixedCOVID–196Ffrench-O’Carroll et al. [58]IrelandEUCA20192847.018.0IES-R22100PreMixedMixed4Firth-Cozens et al. [59]IrelandEUCA19994124.419.5PSS1735.7PreTraumaTerror/conflict/war4Gainer et al. [60]USANAMR20211,72456.127.5APCL588.0Peri/postMixedCOVID–197Gilson et al. [61]FranceEUCA202511776.96.8PCL–52026.8Peri/postGeneralMixed3González-Mesa et al. [62]SpainEUCA202122068.112.4ITQ2227.5Peri/postOB-GYNCOVID–196Gregory et al. [63]FranceEUCA201968072.512.4IES-R2228.2PreMixedTerror/conflict/war6Guldner et al. [64]USANAMR202255NS3.6IES-R2217PreMixedTerror/conflict/war5Guo et al. [65]ChinaEAPAC202279563.420.8PC-PTSD5NSPeri/postAnesthesiologyCOVID–195Hasanovic and Herenda [66]Bosn. and Herz.EUCA20087884.610.3HTQ1682.2PreFamilyTerror/conflict/war4Hébert et al. [67]CanadaNAMR20236053.014.0IES-R2270.6Peri/postMixedCOVID–196Hodgetts et al. [68]Bosn. and Herz.EUCA200313382.018.0PCL-C1790.5PreFamilyTerror/conflict/war5Holzer et al. [69]USNAMR202122250.09.0IES-R2216.2PreNSWork-related stress4Jackson et al. [25]USANAMR20191,927NS18.4PC-PTSD517.0PreSurgeryMixed8James et al. [70]USANAMR202239339.416.3PCL–6617.8Peri/postTrauma surgeryCOVID–195Johns et al. [71]UKEUCA202234675.011.8PCL–520NSPeri/postMixedCOVID–196Joseph et al. [17]USANAMR201445323.815.0PCL-C1741.0PreTrauma surgeryWork-related stress7Kalyanaraman et al. [72]USANAMR202229454.08.0PCL–52016.0Peri/postPediatricCOVID–197Kannan et al. [73]USANAMR2019194NS5.2PCL–52069.0PreInternalMixed4Kaplan et al. [74]USNAMR202156050.217PCL–52056.6PreMixedWork-related stress5Kisten et al. [75]South AfricaSSA202316440.217.9IES-R22NSPeri/postAnesthesiologyCOVID–194Lafta et al. [76]IraqMENAFR202522367.711.2PCL-C1794.0Peri/postNSWork-related stress6Lange et al. [77]FranceEUCA202233243.510.6IES-R2229.2Peri/postGeneralCOVID–196Lasalvia et al. [78]ItalyEUCA202221550.535.9IES-R2238.3Peri/postGeneralCOVID–196Leaune et al. [79]FranceEUCA202176444.213.7IES-R22NSPrePsychiatryWork-related stress6León Rojas et al. [80]Mexico202230310019.4PCL–520NSPeri/postNSCOVID–195Linane et al. [81]IrelandEUCA2019110NS11.8PCL-C1734.9PreNSWork-related stress3Lo et al. [82]USANAMR201938NS13.0PCL–52088.4PreMixedMixed4Lombard et al. [83]South AfricaSSA202239148.617.6PCL–52023.8Peri/postAnesthesiologistCOVID–196Lum et al. [84]SingaporeEAPAC202125743.68.9IES-R22NSPeri/postGeneralCOVID–196Lundin et al. [85]Denmark/Afghan.EUCA20124734.00PCL-C2065.0PreMedical officersTerror/conflict/war6Malinauskiene and Einarsen [86]LithuaniaEUCA2014323NS15.8IES-R2289.2PreFamilyAggression/violence6Marco et al. [23]USANAMR20201,30040.022.3PCL–5203.4Peri/postTraumaMixed7McFarland und Roth [87]USANAMR20175652.017.0IES-R2258.0PreOncologyWork-related stress4Mukherjee et al. [88]USANAMR20221,01749.69.0PCL–5202.8Peri/postMixedCOVID–197Naghavi et al. [7]UKEUCA2013147NS12.0IES–66NSPreNSWork-related stress3Ntalouka et al. [89]GreeceEUCA202410072.018.0PCL–52085.0Peri/postAnesthesiologyWork-related stress4O’Meara et al. [90]IrelandEUCA202216NS6.3PC-PTSD5NSPreSurgeryNS3Ouazzani Housni Touhami et al. [91]MoroccoMENAFR20221,26759.321.7PCL–52063.3Peri/postNSCOVID–198Pajonk et al. [92]GermanyEUCA201248724.216.8PTSS–101042.7PreTraumaNS7Pascoe et al. [93]AustraliaEAPAC20221,96663.63.3IES–66NSPeri/postNSMixed7Pasin et al. [94]ItalyEUCA202050356.855.8IES-R2238.8Peri/postNSCOVID–195Roberts et al. [95]UK and IrelandEUCA202113,89651.012.6IES-R2271.7Peri/postMixedCOVID–19823,07951.010.182.7COVID–198Rollin et al. [96]FranceEUCA202431860.018.0PCLS1713.6Peri/postMixedWork-related stress5Ruitenburg et al. [97]The NetherlandsEUCA201243253.015.0IES-R2251.0PreMixedNS7Saeki et al. [98]JapanEAPAC201175817.58.2IES-R2266.0PreMixedAggression/violence6Sar-El et al. [99]IsraelMENAFR202214551.79.6IES–6677.0Peri/postNSCOVID–195Sansone et al. [100]USANAMR20076127.91.6PC-PTSD554.0PreMixedMixed5Scheepstra et al. [101]The NetherlandsEUCA2020137455.11.5TSQ1027.7PreMixedNS6Seifeldin Abdeen et al. [102]EgyptMENAFR202312464.537.9PCL-C17NSPeri/postNSCOVID–195Slade et al. [103]UKEUCA20201,09571.118.0IES-R2217.4PrePediatricWork-related stress7Somville et al. [6]BelgiumEUCA201615237.714.5IES-R2243.9PreTraumaWork-related stress5Stanislawski et al. [104]AustraliaEAPAC2023111045.739.0PCL–52074.8Peri/postMedical studentsCOVID–195287NS29.362.6Work-related stress5Stukalin et al. [105]CanadaNAMR20195135.331.4IES-R2234.0PreMixedNS4Thirayan et al. [106]South AfricaSSA20241931.610.5TSQ1032.0PreTrauma surgeryWork-related stress4Thompson et al. [5]UKEUCA201716739.016.0IES-R2286.0PreMixedMixed6Tuncer et al. [107]TurkeyEUCA202222274.355.0IES-R2295.7Peri/postPediatricCOVID–198Valenzuela et al. [26]USANAMR202333435.917.0PCL–6617.8Peri/postTrauma surgeryCOVID–197van der Ploeg et al. [108]The NetherlandsEUCA20036432.114.0IES-R22NSPreForensicNS6van Niekerk et al. [109]South AfricaSSA202037557.628.8IES-R2224.4PreAnesthesiologyWork-related stress7van Steijn et al. [110]The NetherlandsEUCA201941067.36.3TSQ1018.9PrePediatricMixed7Vance et al. [111]USANAMR20211,13458.610.8PC-PTSD526.0PreMixedWork-related stress7Warren et al. [112]USANAMR201313316.521STSS17NSPreTrauma surgeryTrauma patients4Weiniger et al. [34]IsraelMENAFR2006212NS15.6PSS-SR1775.4PreMixedTerror/conflict/war5Wilberforce et al. [113]CanadaNAMR201015954.04.4PCL–52048PreMixedWork-related stress7Wilgenbusch et al. [114]CanadaNAMR202356555.821.2PCL-C1718.6PreMixedNS5Zafar et al. [115]PakistanSAS201617958.715.4PCL-C1792.2PreMixedAggression/violence5Abbreviations: *Time = time point of data collection. Bosn. and Herz. = Bosnia and Herzegovina; WB = World Bank; NAMR = North America, EUCA = Europe and Central Asia; EAPAC = East Asia and Pacific; MENAFR = Middle East and North Africa; SAS = South Asia; SSA = Sub-Saharan Africa; LACA = Latin America and Caribbean; NS = not specified; PCL-5 = PTSD Checklist for DSM-5; TSQ = Trauma Screening Questionnaire; PC-PTSD = Primary Care PTSD Screen for DSM-5; IES-R = Impact of Event Scale–revised; COVID-19-PTSD = Posttraumatic Stress Disorder Related to COVID-19 Questionnaire; PCL-C = PTCS Checklist Civilians; PSS = PTSD Symptom Scale; APCL = Abbreviated PTSD Checklist; HTQ = Harvard Trauma Questionnaire; PCL-6 = Impact of Event Scale 6; PTSS-10 = Posttraumatic Stress Scale 10; PCLS = PTSD Checklist Scale; STTSS = Secondary Traumatic Stress Scale; PSS–SR = PTSD Symptom Scale–Self Report; RR = response rate.
Risk of bias was assessed [45]. A summary of the quality ratings for each included study is presented in the last row of Table 1. Quality scores ranged from 3 to 8, with a mean score of 5.58 (SD =1.28). Overall, 58 (72.50%) studies were rated as moderate quality, 4 (5.0%) studies as high quality, and 18 (22.50%) studies as low quality. Figure 2 provides an overview of the proportion of studies meeting each quality criterion. The most common sources of potential bias were insufficient coverage of the sample, low response rates, and inappropriate sampling frames or sampling methods. Cohen’s Kappa for interrater reliability was .71, indicating a moderate level of agreement [116].Figure 2.Risk of bias rating in %.
Interrater reliability for the screening procedure was .95 for the abstract screening and .88 for the full-text screening, indicating an almost perfect agreement for abstract and a strong agreement for full-text screening [116].
PTS symptoms among physicians
The primary outcome was the prevalence of PTSD symptoms among physicians, as assessed by all 81 studies included in our meta-analysis (see Table 1).
The mean effect size was 0.149, with a 95% confidence interval ranging from 0.132 to 0.168, resulting in a pooled prevalence rate of 14.9% (N = 6816). The Q value was 1902.23 with 80 degrees of freedom, and p < 0.001, therefore, heterogeneity was confirmed. The I ^2^ statistic was 95.79%, indicating that some 95.79% of the variance in observed effects reflects variance in true effects rather than sampling error [46]. The prediction interval ranged from 0.050 to 0.371. The prevalence of PTSD symptoms ranged from 0 to 55.8%.
Subgroup analysis
Overall, only income level and the length of the screening questionnaire moderated the occurrence of PTSD symptoms.
Studies with short screens (≤10 items) estimated the occurrence of PTSD significantly lower (event rate = 10.2, 95% CI [0.076–0.136]) compared to those using longer screens (event rate = 16.4, 95% CI [0.143–0.187]) (p < 0.027). Regarding income level, there was no significant difference (p = 0.483) between lower middle-income countries (event rate = 23.8, 95% CI [0.168–0.32.5]) and upper middle-income countries (event rate = 20.6, 95% CI [0.166–0.253]). Consequently, these groups were merged and compared to high-income countries. Studies in high-income countries estimated the occurrence of PTSD significantly lower (event rate = 13.6, 95% CI [0.118–0.156]) than studies in middle-income countries (event rate = 21.2, 95% CI [0.163–0.268]) (p < 0.036).
There were no significant differences in other subgroups (see Table 2; all ps > 0.05). Additionally, meta-regression analyses showed that neither year of data collection nor gender could explain the heterogeneity (all ps > 0.05).Table 2.Subgroup analysisSubgroupsCategories N studies N total (participants)Prevalence % (N)95% CIHeterogeneityBetween Group comparison I ^2^Qdf (Q)pCorr.COVID–19Pre3914,51913.8 (N = 2,048)0.115–0.16590.67407.17410.235>.999Peri/post4226,53216.0 (N = 4,768)0.136–0.18797.071400.3138EmergencyOther6936,62014.6 (N = 5,990)0.128–0.16796.301835.70680.148>.999Emergency12443116.6 (N = 825)0.121–0.22583.3666.1011SurgeryOther7237,08215.0 (N = 6,193)0.131–0.17096.131833.06710.912>.999Surgery9396914.4 (N = 623)0.097–0.20985.8256.408Trauma categoryWar/terror7124612.2 (N = 159)0.075–0.19354.5713.2160.051.459Pandemic3423,31517.6 (N = 4,315)0.147–0.20997.361250.8733Work-related4016,49013.2 (N = 2,342)0.110–0.15792.51520.8339IncomeHigh6529,82913.6 (N = 4,342)0.118–0.15695.921569.55640.004.036Middle1611,22221.1 (N = 2,473)0.163–0.26891.81183.1215Instrument categoryIES3017,39116.6 (N = 3,276)0.136–0.20197.431126.17290.805>.999PCL34728515.2 (N = 1,169)0.125–0.18391.90407.5233PC-PTSD6427715.6 (N = 748)0.095–0.24693.5177.075Instrument lengthShort screen1712,24410.2 (N = 1,583)0.076–0.13697.40614.70160.003.027*Long screen6428,80716.4 (N = 5,233)0.143–0.18794.921240.2663WB regionEAPAC610,20613.0 (N = 1,730)0.078–0.20798.57348.9250.732>.999EUCA3414,22414.5 (N = 2,103)0.116–0.17896.761016.8433MENAFR6236418.6 (N = 486)0.115–0.28889.7048.555NAMR2912,82714.2 (N = 2,202)0.112–0.17893.56434.2028QualityHigh5722722.0 (N = 1,204)0.139–0.32898.54273.9440.216>.999Low18168414.2 (N = 237)0.106–0.18867.7552.7117Moderate5832,14114.5 (N = 5,375)0.125–0.16896.331554.3457 Notes. *p < 0.05.Abbreviations: WB = World Bank; EAPAC = East Asia and Pacific; EUCA = Europe and Central Asia; MENAFR = Middle East and North Africa; NAMR = North America.
Discussion
Due to high psychological challenges, physicians face a higher lifetime risk of developing posttraumatic stress disorder (PTSD) compared to the general population. This meta-analysis aimed to assess the current prevalence of PTSD among physicians and the factors that mediate the occurrence of symptoms. Our meta-analysis found a pooled prevalence of 14.9% for PTSD among physicians, which is consistent with the findings of the previous meta-analysis conducted among physicians [13]. Compared to the global prevalence in the general population of 3.9% [14] physicians are therefore three to four times more likely to suffer from PTSD than the general adult population.
Subgroup analysis results provide evidence that posttraumatic stress symptoms are lower among physicians in high-income countries compared to those in middle-income countries. These findings might be influenced by qualitative differences in the healthcare systems across countries with varying income levels [18]. Structural stress factors, such as long and irregular working hours or sleep deprivation, which might be more pronounced in lower and middle-income countries, could also play a role in affecting physicians’ mental health [30].
There was no significant difference in outcome when comparing PCL, PC-PTSD, and IES-based screening tools. This aligns with research suggesting similar accuracy between different instruments [36]. When comparing short and long screening instruments, we found a significantly lower prevalence rate in short screening tools. These results stand in contrast to our hypothesis and are also not in line with Mouthaan et al. [36] who found no differences in accuracy between shorter and longer instruments. One possible explanation could be attributed to the structure of the questionnaires. For instance, the Primary Care PTSD Screen (PC-PTSD) [117] employs a cut-off of three of five items (with the revised version of PC-PTSD-5 comprising four items) with each item corresponding to one of the core diagnostic criteria for PTSD. This structure might increase the sensitivity for detecting individuals who meet the diagnostic criteria for PTSD, while potentially underestimating those who exhibit subthreshold posttraumatic stress symptoms.
To our knowledge, this is the first meta-analysis, which directly compares the prevalence of PTSD symptoms among physicians before and after the onset of the COVID-19 pandemic. Some studies have reported an increase in PTSD symptoms during the pandemic [53, 60, 102]. In several longitudinal studies, which stated high levels of PTSD at the pandemic’s onset, a subsequent decrease in symptoms was observed over time [21, 22]. In our analysis, we found a descriptive difference in PTSD prevalence before the pandemic, pre (13.8%), and during/after the pandemic (16.0%), COVID-19 pandemic, though this difference was not statistically significant. This finding might be attributable to an adaption process, where PTSD symptoms could have initially increased due to the acute stress of the pandemic, followed by a reduction over time as individuals adjusted. However, further research is needed to confirm this potential pattern. Additionally, this finding suggests that physicians were already exposed to significant stress before the COVID-19 pandemic, whether from traumatic experiences at work [97], medical errors [9], or physical assaults [8, 98], with the pandemic serving as an additional stressor.
No other moderators were identified in our analysis, possibly due to methodological limitations such as small subgroup sizes. Thus, contrary to expectations, neither the surgery nor the emergency subgroups, nor trauma type, had a significant impact on PTSD prevalence. In contrast to findings from other studies, PTSD prevalence in studies conducted in conflict areas was not elevated. Instead, an opposite trend emerged: although not statistically significant, studies related to COVID-19 showed descriptively higher PTSD prevalence than those examining work-related trauma or exposure to war and terrorism.
Limitations
Our meta-analysis included studies with varying outcomes and potential moderators, reflecting the inherent heterogeneity in this field. While this diversity allows for a broader understanding of PTSD prevalence among physicians, future research might benefit from focusing on more homogenous populations in terms of country, specialty, and type of trauma exposure. This would enable greater comparability and potentially yield more precise estimates of PTSD prevalence within specific subgroups of physicians.
There was considerable variability in subgroup size, ranging from one study to 72 studies within certain subgroups. This limits the robustness of the statistical analyses and the interpretation of some results. Furthermore, this variability resulted in excluding South and East Asian countries from the subgroup analysis due to inadequate sample sizes. Despite this, there exists a substantial body of research from South Asian regions that includes healthcare workers in general [38, 37, 39], which was not considered in our analysis. Future research should focus on comparative studies across different healthcare professions in the various areas of the world.
One of the most significant limitations is the lack of representativeness in a majority of studies. Based on the risk of bias assessment, only half of the studies used sample frames appropriate for answering our research question, regardless of whether they matched the specific research questions of the studies. This raises concerns about whether the reported prevalence of PTSD in these studies can be generalized to physicians as a whole. Future research should place greater emphasis on ensuring representativeness in study design.
Conclusion and implications
The medical profession is associated with a heightened risk of experiencing trauma and developing posttraumatic stress disorder (PTSD) symptoms. The mental health of medical professionals is crucial for maintaining the overall quality of the healthcare system, as stress and mental illness can significantly impair medical performance and patient care [118]. Improving physicians’ well-being, especially in lower income countries, not only supports individual practitioners but also holds the potential to enhance the overall quality of healthcare delivery.
In this context, the treatment of physicians is of central importance. In addition to conventional psychotherapeutic treatment, Internet-based therapy can contribute to improving access to care, offering an anonymous, low-threshold, and highly flexible treatment option (for more details, see [119]). Society needs to prioritize the monitoring and support of physicians’ mental health, recognizing their essential role in sustaining the quality of healthcare services. By implementing early preventive measures and interventions, the overall health of medical professionals can be positively influenced, protecting and ensuring their well-being, and in turn, the well-being of the patients they serve.
Supporting information
10.1192/j.eurpsy.2025.10084.sm001Reinhardt et al. supplementary material 1Reinhardt et al. supplementary material
10.1192/j.eurpsy.2025.10084.sm002Reinhardt et al. supplementary material 2Reinhardt et al. supplementary material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Joules N, Williams DM, Thompson AW. Depression in resident physicians: a systematic review. Open J Depress. 2014;3:89–100.
- 2Low ZX, Yeo KA, Sharma VK, Leung GK, Mc Intyre RS, Guerrero A, et al. Prevalence of burnout in medical and surgical residents: a meta-analysis. Int J Environ Res Public Health. 2019;16(9):1479.31027333 10.3390/ijerph 16091479 PMC 6539366 · doi ↗ · pubmed ↗
- 3Kuhn CM, Flanagan EM. Self-care as a professional imperative: physician burnout, depression, and suicide. Can J Anaesth. 2017; 64(2):158–68.27910035 10.1007/s 12630-016-0781-0 · doi ↗ · pubmed ↗
- 4Brooks SK, Gerada C, Chalder T. Review of literature on the mental health of doctors: are specialist services needed? J Ment Health. 2011;20(2):146–56.21275504 10.3109/09638237.2010.541300 · doi ↗ · pubmed ↗
- 5Thompson CV, Naumann DN, Fellows JL, Bowley DM, Suggett N. Post-traumatic stress disorder amongst surgical trainees: an unrecognised risk? Surgeon. 2017; 15(3):123–30.26482084 10.1016/j.surge.2015.09.002 · doi ↗ · pubmed ↗
- 6Somville FJ, de Gucht V, Maes S. The impact of occupational hazards and traumatic events among Belgian emergency physicians. Scand J Trauma Resusc Emerg Med. 2016;24:1–10.27121279 10.1186/s 13049-016-0249-9PMC 4848801 · doi ↗ · pubmed ↗
- 7Naghavi SH, Shabestari O, Alcolado J. Post-traumatic stress disorder in trainee doctors with previous needlestick injuries. Occup Med. 2013; 63(4):260–5.10.1093/occmed/kqt 02723580567 · doi ↗ · pubmed ↗
- 8Phillips JP. Workplace violence against health care workers in the United States. N Engl J Med. 2016; 374(17):1661–9.27119238 10.1056/NEJ Mra 1501998 · doi ↗ · pubmed ↗