A Woman With Continuous, Involuntary, Unilateral Movement
Raymond Che, Suhani Patel, Michael Edwards, Michelle Wilson

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
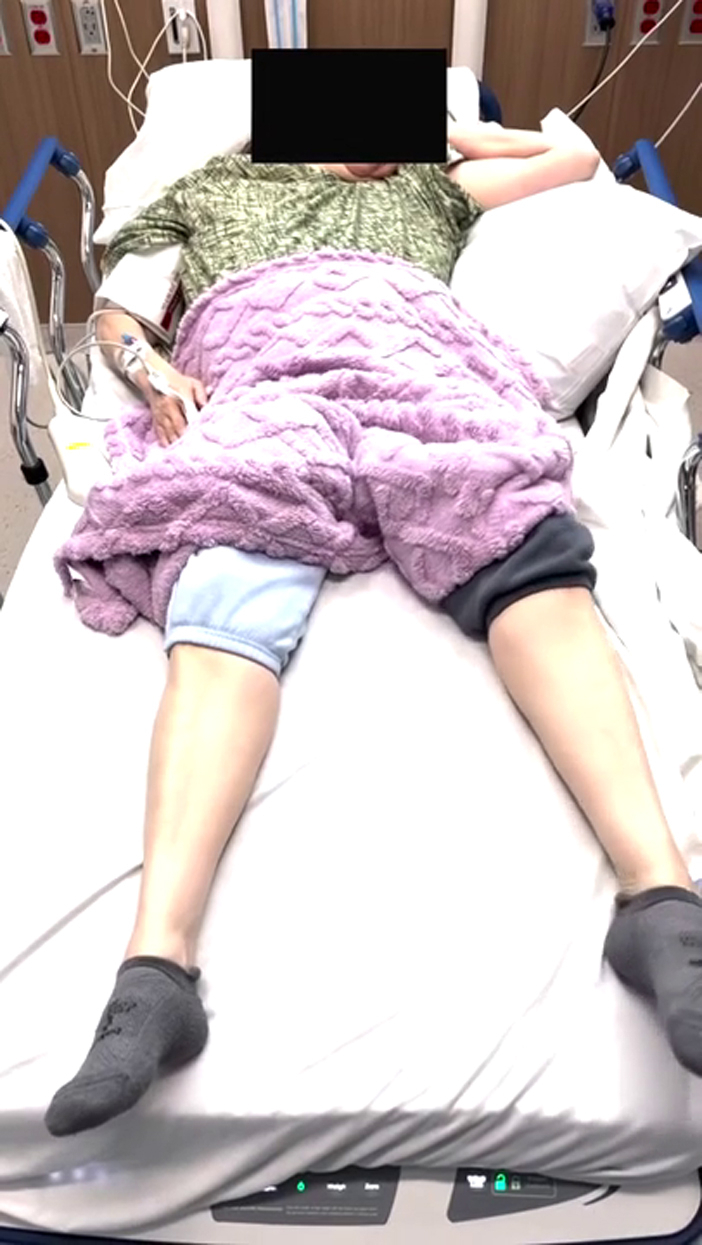 Figure 1
Figure 1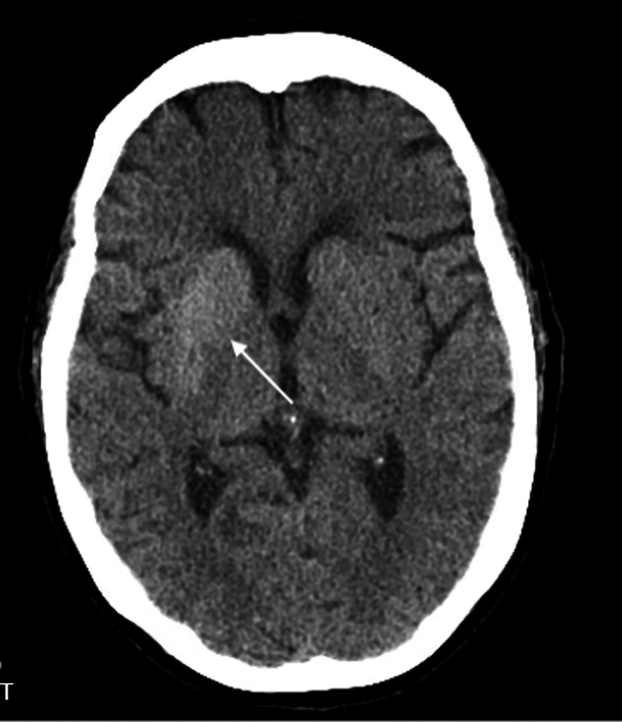 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological and metabolic disorders · Neurological disorders and treatments · Genetic Neurodegenerative Diseases
Case Presentation
1
A 59-year-old woman with type 2 diabetes mellitus presented to the emergency department with 4 days of continuous, involuntary movements of her left arm and leg. She reported poor adherence to her diabetes medications and significant psychosocial stress. Vital signs were stable. Examination revealed continuous, irregular, choreiform movements of the left upper and lower extremities (Video 1) without other deficits. A noncontrast computed tomography scan of the head was obtained (Fig). Laboratory results revealed a blood glucose level of 420 mg/dL, negative ketones, and normal osmolality.Video 1Continuous, involuntary, unilateral movement seen on examination.FigureDiffuse right basal ganglia hyper-attenuation.
Diagnosis: Nonketotic Hyperglycemic Hemichorea Hemiballismus
2
Nonketotic hyperglycemic hemichorea hemiballismus, also called diabetic striatopathy, is a rare neurological complication of uncontrolled diabetes with a prevalence of approximately 1 in 100,000.1 It is the second most frequent cause of chorea after basal ganglia stroke.2
Diagnosis is made based on the presence of unilateral choreiform or ballistic movements in the setting of uncontrolled, often nonketotic, hyperglycemia, accompanied by characteristic imaging findings.1^,^2 Computed tomography typically demonstrates hyperdensity, whereas magnetic resonance imaging demonstrates T1 hyperintensity in the contralateral basal ganglia.3 The mechanism remains unclear.1
Treatment focuses on glycemic control. Around 25% of the patients improve with glucose correction alone, whereas others require medications such as haloperidol, tetrabenazine, or benzodiazepines to manage involuntary movements.1^,^2 Recovery varies from days to months, averaging 6 months.1 Some may experience only partial improvement, even after years, requiring long-term management. Our patient was started on fluids and an insulin drip, then admitted. She was discharged with improved glycemic control on Risperdal and as needed clonazepam for ongoing involuntary movements.
Funding and Support
By JACEP Open policy, all authors are required to disclose any and all commercial, financial, and other relationships in any way related to the subject of this article as per ICMJE conflict of interest guidelines (see www.icmje.org). The authors have stated that no such relationships exist.
Conflict of Interest
All authors have affirmed they have no conflicts of interest to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Arecco A.Ottaviani S.Boschetti M.Renzetti P.Marinelli L.Diabetic striatopathy: an updated overview of current knowledge and future perspectives J Endocrinol Invest 471202411510.1007/s 40618-023-02166-5PMC 1077672337578646 · doi ↗ · pubmed ↗
- 2Chua C.-B.Sun C.-K.Hsu C.-W.Tai Y.-C.Liang C.-Y.Tsai I.-T.“Diabetic Striatopathy”: clinical presentations, controversy, pathogenesis, treatments, and outcomes Sci Rep 1012020159410.1038/s 41598-020-58555-w 32005905 PMC 6994507 · doi ↗ · pubmed ↗
- 3Xu Y.Shi Q.Yue Y.Yan C.Clinical and imaging features of diabetic striatopathy: report of 6 cases and literature review Neurol Sci 431020226067607710.1007/s 10072-022-06342-y 35965280 PMC 9376124 · doi ↗ · pubmed ↗