White matter tracts associated with iTBS-induced heart rate deceleration and treatment response in major depressive disorder
Jonas Wilkening, Roberto Goya-Maldonado

TL;DR
This study explores how white matter tracts in the brain relate to heart rate changes and treatment response in depression patients undergoing iTBS.
Contribution
The study identifies specific white matter tracts that predict heart rate modulation and treatment outcomes in iTBS for depression.
Findings
Fractional anisotropy in the fornix and cingulum correlates with heart rate deceleration and symptom improvement.
Longitudinal increases in cingulum FA are linked to greater symptom alleviation after iTBS.
White matter changes in the cingulum appear as early as four weeks into treatment.
Abstract
Intermittent theta burst stimulation (iTBS) is a well-established treatment for major depressive disorder (MDD), but predicting clinical outcomes remains challenging. Heart rate deceleration induced by iTBS has emerged as a potential biomarker for treatment response, yet the role of white matter (WM) properties in mediating these effects is largely unexplored. In this quadruple-blind, crossover study, we investigated the relationship between WM microstructure, iTBS-driven heart rate modulation, and antidepressant effects. Using correlational tractography, we focused on four major WM tracts—the cingulum, fornix, superior longitudinal fasciculus, and uncinate fasciculus—to examine short-term microstructural changes in relation to therapeutic outcomes. At baseline, findings revealed that fractional anisotropy (FA) in the fornix and right dorsal cingulum was negatively correlated with heart…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
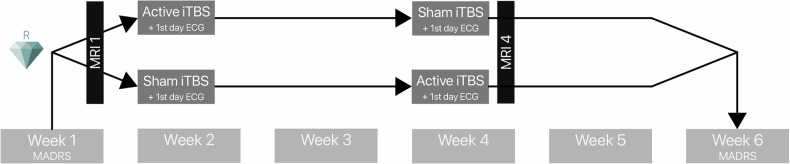 Figure 1
Figure 1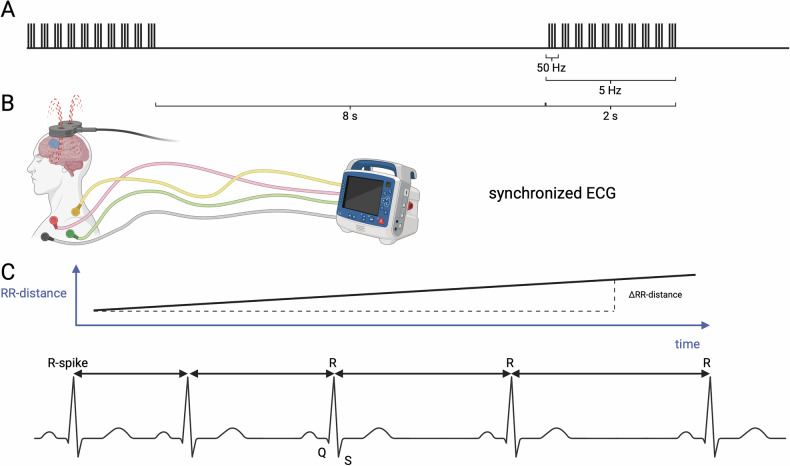 Figure 2
Figure 2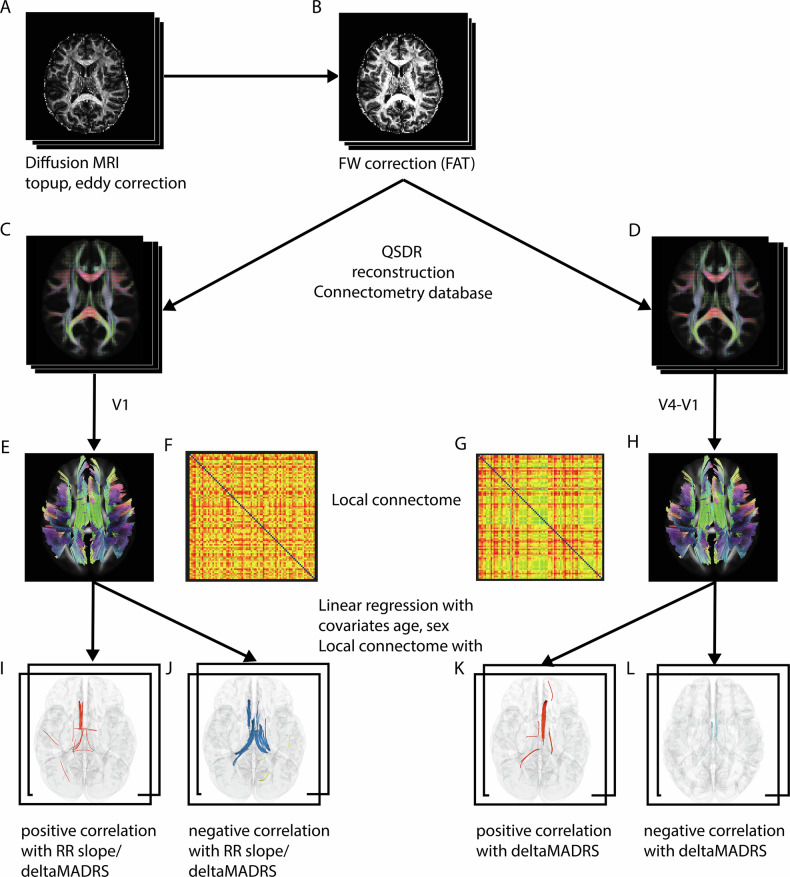 Figure 3
Figure 3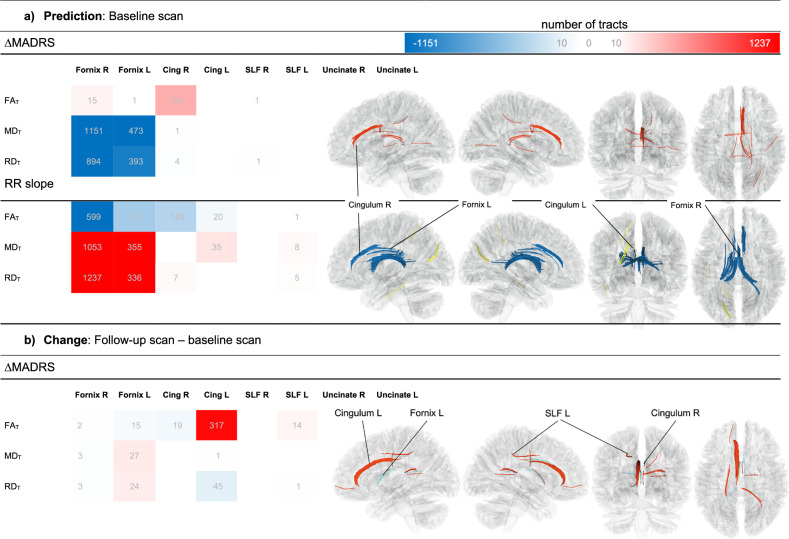 Figure 4
Figure 4- —https://doi.org/10.13039/501100002347Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Neuroimaging Techniques and Applications · Functional Brain Connectivity Studies · Advanced MRI Techniques and Applications
Introduction
Major depressive disorder (MDD) is a pervasive mental health condition with significant societal and individual impacts, marked by rising prevalence globally [1]. While pharmacological and psychological interventions remain central to treatment, novel neuromodulatory approaches, such as intermittent theta burst stimulation (iTBS), have garnered attention for their potential efficacy in alleviating depressive symptoms. iTBS, a patterned form of repetitive transcranial magnetic stimulation (rTMS), applies rapid bursts of stimulation to the left dorsolateral prefrontal cortex (DLPFC). This technique has been shown to reduce depressive symptoms, offering promise as an alternative or adjunctive therapy for patients who fail to respond to conventional treatments [2, 3]. However, predicting which individuals will benefit from iTBS remains a significant challenge, and identifying reliable biomarkers of treatment response is an ongoing area of research.
Among these potential biomarkers, heart rate (HR) modulation during iTBS has emerged as a promising indicator of therapeutic outcomes. Individuals with MDD frequently exhibit autonomic nervous system dysregulation, evidenced by increased resting HR and reduced heart rate variability (HRV) compared to healthy individuals [4–6]. This autonomic imbalance reflects altered interactions between the brain and peripheral systems, particularly within the central autonomic network (CAN). Notably, high-frequency rTMS targeting the DLPFC has been shown to acutely reduce HR, a change not observed with sham stimulation [7–9]. Furthermore, changes in HR and HRV parameters during stimulation have been correlated with reductions in symptom severity [10, 11]. These findings suggest that HR modulation may serve as a functional biomarker of iTBS efficacy, reflecting changes in the frontal-vagal network that integrates autonomic and cognitive processes [11, 12]. While this supports a role for functional mechanisms, the structural pathways underpinning these effects remain poorly understood.
White matter (WM) microstructure may play a pivotal role in mediating the effects of iTBS on both HR modulation and depressive symptoms. Altered WM integrity is a well-documented feature of MDD, with diffusion tensor imaging (DTI) studies revealing widespread microstructural abnormalities in individuals with the disorder compared to healthy controls [13–15]. Fractional anisotropy (FA), a DTI-derived metric of WM integrity, has been implicated as a potential predictor of treatment response. For example, prior research has shown that higher FA values in specific WM tracts are associated with clinical improvement following antidepressant therapies, including pharmacological and neuromodulatory interventions [16–19]. Importantly, these findings suggest that WM pathways may provide insight into the brain’s capacity for neuroplasticity, which could be essential for understanding iTBS efficacy. However, the specific WM tracts associated with iTBS-induced changes in HR and symptom alleviation have yet to be systematically investigated.
Beyond baseline WM properties, longitudinal changes in WM microstructure may also hold predictive value for treatment outcomes. Neuromodulatory interventions, including rTMS, have been shown to induce rapid changes in WM integrity. For instance, increases in FA and reductions in mean diffusivity (MD) and radial diffusivity (RD) have been observed as early as one week after treatment, correlating with clinical improvement in mood disorders [19–21]. These findings suggest that WM reorganization may reflect dynamic neuroplastic processes triggered by iTBS. Crucially, such changes are not limited to the stimulation site but extend to broader regions, highlighting the widespread impact of neuromodulation on brain connectivity. By combining baseline and longitudinal analyses, it may be possible to capture both stable WM characteristics that predispose individuals to treatment response and dynamic changes that signal neuroplasticity during therapy.
To investigate these mechanisms, advanced imaging techniques can provide greater precision in assessing WM microstructure. For example, free-water correction enhances the specificity of diffusion metrics by separating extracellular diffusion components, such as edema, from anisotropic diffusion within axons [22]. Correlational tractography, a complementary method, maps structural connectivity patterns of the local connectomes linked to study variables and employs differential tractography with higher sensitivity than traditional tractography [23]. These methods address limitations associated with traditional DTI, such as partial volume effects, enabling the analysis of white matter tract subcomponents and thereby allowing for more accurate identification of WM pathways associated with treatment outcomes.
Several WM tracts stand out as candidates for mediating the effects of iTBS in MDD. The cingulum, which interconnects regions of the default mode network (DMN) and the limbic system, plays a critical role in emotional regulation and reward processing [24]. Greater WM integrity in the cingulum has been linked to antidepressant response, possibly due to its role in modulating activity in the subgenual anterior cingulate cortex (sgACC), a key region implicated in MDD pathology and HR control [7, 25, 26]. Similarly, the fornix, a major output tract of the hippocampus that connects to the hypothalamus and amygdala, is integral to memory and autonomic regulation. FA values in the fornix have been associated with emotional regulation and autonomic function, suggesting its relevance to iTBS-driven HR modulation and clinical outcomes [27, 28].
In addition, the superior longitudinal fasciculus (SLF) and uncinate fasciculus have been implicated in MDD and its treatment. The SLF, which connects the DLPFC to parietal regions involved in attention and executive function, has been associated with treatment resistance, with lower FA values linked to reduced responsiveness to antidepressant therapies [29]. Meanwhile, the uncinate fasciculus, a tract connecting the sgACC to the amygdala, plays a key role in emotion regulation. This tract has been associated with clinical improvement following deep brain stimulation, highlighting its potential role in mediating therapeutic effects in MDD [30, 31]. Together, these four tracts form an interconnected network that integrates cognitive, emotional, and autonomic functions, making them prime candidates for understanding the mechanisms underlying iTBS efficacy.
In the present study, we examined the relationship between WM microstructure, HR modulation, and clinical improvement in MDD, focusing on four major tracts anatomically relevant to the iTBS stimulation site: the cingulum, fornix, SLF, and uncinate fasciculus. Our dual approach combined baseline and longitudinal analyses to provide a comprehensive understanding of how WM properties relate to iTBS efficacy. We hypothesized that tracts with higher baseline microstructural integrity, as reflected by higher FA as well as lower MD and RD, would predict greater HR deceleration and stronger symptom alleviation. Additionally, we expected to observe longitudinal increases in FA alongside decreases in MD and RD in these tracts, with these changes correlating positively with clinical improvement. By integrating functional biomarkers like HR modulation with WM structural metrics, this study aims to advance our understanding of the mechanisms underlying iTBS efficacy and pave the way for more personalized therapeutic strategies.
Materials and methods
Participants
The study protocol (clinicaltrials.gov/show/NCT05260086) complies with the latest version of the Declaration of Helsinki and was approved by the Ethics Committee of the University Medical Center Göttingen (UMG). Prior to enrollment, all participants provided verbal and written informed consent after the study protocol was fully explained. Individuals aged 18 to 60 years, diagnosed with MDD and currently experiencing a moderate or severe depressive episode, were recruited. Trained psychiatrists confirmed the inclusion criteria using the Structured Clinical Interview for DSM-5 Disorders – Clinical Version (SCID-5-CV) and the the Montgomery-Åsberg Depression Rating Scale (MADRS) [32, 33].
Patients with contraindications to MRI or rTMS (e.g., epilepsy, neurological diseases, pregnancy, metallic implants) were excluded from the study. Participants were required to maintain stable medication regimens for a minimum of two weeks prior to and throughout the duration of the study, with adherence monitored through serum level assessments. These values were also incorporated into the statistical model to account for their potential effects on clinical improvement. The sample included both clinic inpatients and outpatients; however, the study intervention was administered exclusively in an outpatient setting. Detailed study information can be found elsewhere [12, 34].
Study design
The study protocol spanned six weeks and employed a quadruple-blinded (participant, care provider, investigator, and rater) randomized sham-controlled crossover design (Fig. 1). Each participant received one week of active stimulation and one week of sham stimulation, with the order of conditions randomly assigned (active-sham, sham-active). Randomization followed pre-coded sequences generated using a true random function in MATLAB (The MathWorks, Inc., Natick, MA, USA) and was managed by the study principal investigator, who had no direct contact with participants.Fig. 1. Study design.The accelerated iTBS stimulation protocol was administered in a week over five consecutive days, before or after an identical sham protocol, in a crossover design. The MADRS score was evaluated at baseline and at a six-week follow-up, yielding a delta MADRS score. MRI scans were acquired before and after iTBS intervention. ECG recordings were obtained on the first day of each intervention week. iTBS Intermittent theta burst stimulation, MADRS Montgomery-Åsberg Depression Rating Scale, ECG Electrocardiogram.
As part of a broader investigation into the clinical benefit of personalized stimulation sites, an additional pseudorandomization was performed to compare two stimulation approaches: fixed stimulation at the EEG 10-20 cap F3 position or a personalized approach. The personalized approach involved selecting a point within the left DLPFC in which the individual exhibited the strongest anticorrelation with the DMN as measured by resting-state functional MRI [12]. In the current study, we did not consider this separation, opting for a unified stimulation approach due to the similarity of the stimulation methods. Moreover, prior research using the current sample revealed no significant influence of the stimulation target groups on RR slope or treatment outcome [12]; therefore, we analyzed the sample here as a whole.
A nine-day gap separated the two stimulation weeks. Trained clinical interviewers collected the MADRS scores at the end of each week, starting from baseline, to assess the clinical outcome over the six-week period (Fig. 1).
iTBS treatment
The MagVenture X100 system with Mag-option and a figure-of-eight MCF-B65 A/P cooled coil was used for stimulation by trained and experienced personnel. Each daily visit included four sessions of approximately 10 min each, followed by at least 20-minu pauses, based on the necessary inter-session time described in previous literature [35]. The iTBS protocol consisted of bursts at 5 Hz, each comprising 3 pulses delivered at 50 Hz, resulting in a volley with 2 s on and 8 s off (Fig. 2A). One session consisted of 60 volleys, resulting in a total of 1800 pulses per session, 7200 per day, and 36000 pulses in total. The resting motor threshold (RMT) was reevaluated daily via electromyography in the right first dorsal interosseous muscle with the lowest intensity eliciting 50 mV motor reaction in 5 of 10 attempts. Treatment stimulation was performed at 110% of the RMT. In the sham condition, the same figure-eight-shaped MCF-B65 A/P coil was blindly flipped 180 degrees. Additionally, tENS electrodes mimicked scalp sensation simultaneously to the sound of magnetic pulses, regardless of the stimulation condition. The blinding procedure was assessed using a visual analogue scale (VAS).Fig. 2. Visualization of RR slope.iTBS pulses (A) and ECG recordings (B) are time-tracked (created in BioRender). The RR slope (C) is calculated by determining the linear gradient of RR intervals in the ECG. The greater the RR distance, the greater the heart rate deceleration. RR Time between two successive ventricular depolarizations, iTBS Intermittent theta burst stimulation, ECG Electrocardiogram, RR Time between two successive ventricular depolarizations.
Cardiac data acquisition and analysis
During iTBS treatment, subjects had an ECG recorded using three chest electrodes from the NCG-rTMS device (neuroConn NCG-rTMS device, neuroCare, Munich, Germany), allowing synchronization with the triggers of the TMS coil (Fig. 2B). The ECG signal underwent powerline noise reduction using the SciPy module in Python 3.6 and BioSignal Processing (BioSPPy) to remove baseline wander noise [36]. The automatically detected R-peaks were then corrected to match with the maxima of the curve within a tolerance of 50 milliseconds. Subsequently, the intervals between two QRS-spikes in the ECG (RR intervals) were calculated using a Python implementation of the algorithm developed by Lipponen & Tarvainen, 2019 [37], allowing correction for ectopic beats. The slopes of RR intervals (Fig. 2C) were calculated for 45 s after iTBS session initiation, which is the timeframe with the strongest difference between active and sham stimulation in [11]. A positive slope indicates an increase in RR intervals, i.e. a decrease in HR. Outliers greater than ±2.5 in z-standardized values were removed on a session-wise basis. The median RR slope of all four sessions of the first day of stimulation was used as a predictive parameter [38]. It was previously demonstrated that the change in the slope of RR intervals in the first 45 s of stimulation was significantly associated with the six-week treatment outcome (Supplementary Fig. 1A).
Image acquisition
We analyzed MRI data from participants before the stimulation and after the second week of stimulation, resulting in an interval of 4 weeks (Fig. 1). All scans were acquired on a 3 T Siemens scanner (Magnetom Prisma Fit, Siemens Healthcare, Erlangen, Germany) using a 32-channel head coil. The diffusion MRI was acquired at b = 1000 s/mm^2^ with 64 directions including the b0 image, TR = 4200 ms, TE = 93 ms, 90 slices, Flip angle = 90°, FOV = 218 mm, multiband factor = 3, fat saturation enabled. The voxel size was 1.7 mm isotropic.
Image processing
In a total of 34 DTI scans, one slice of one of the 64 volumes with diffusion weighting had to be removed because of artifacts using an in-house-written MATLAB script. After correction of diffusion data for eddy current and motion artifacts using FSL [39] the rotated bvecs were used for subsequent analysis [40, 41] (Fig. 3A).Fig. 3. Diffusion imaging analysis pipeline.The diffusion analysis following the standard FSL processing pipeline (A), incorporating a FW-corrected protocol for DTI data (B). Further processing was conducted using DSI Studio’s QSDR reconstruction to generate a connectometry database for baseline data (C, E, F) and a subtraction database (D, G, H) for longitudinal correlational tractography. Key study variables included delta MADRS scores and HR modulations, represented by the RR- slope (I–L). FW Free-water, QSDR Q-space Diffeomorphic Reconstruction, MADRS Montgomery-Åsberg Depression Rating Scale, HR heart rate, RR Time between two successive ventricular depolarizations.
The data were input into a custom modified Python code (https://github.com/sameerd/DiffusionTensorImaging) referring to Pasternak et al. 2009 [22]. It describes a voxel-wise bi-tensor model which reflects the partial volume artifacts by free water DTI (FW-DTI) and the tissue compartment [22, 42]. The corrected images were fit with FW-corrected FA (FA_T_), MD_T_ and RD_T_ using the dipy.reconstruct.dti function in Python 3.6 (Fig. 3B).
All subsequent analyses were conducted using DSI Studio (version 2022.09.27), following standard analysis protocols. The corrected images were reformatted into a DSI Studio-compatible format and resampled to an isotropic resolution of 2 mm, due to the atlas platform exhibiting better compatibility with 2 than 1.7 mm resolution. Integrity and quality checks were performed automatically [43] and visually inspected.
The diffusion data were reconstructed in the MNI space using q-space diffeomorphic reconstruction (QSDR) [44] (Fig. 3C, D) to obtain the orientation spin distribution function (ODF) [45]. The diffusion sampling length ratio was set to the default value of 1.25. A subject-specific brain mask from FSL tool bet was applied [46], and Gaussian filtering [47] was performed on the DWI signals using DSI Studio to achieve the necessary signal-to-noise ratio for correlational tractography, based on consultation and data inspection provided by the DSI Studio developer. FA_T_, MD_T_, and RD_T_ maps were registered to the MNI space using QSDR.
Correlational tractography and connectometry
From the preprocessed data, we created connectometry database files for both baseline (Fig. 3C) and longitudinal analyses. In the latter case, the algorithm created a subtraction image (V4-V1, Fig. 3D).
Diffusion MRI correlational tractography was performed, followed by connectometry for testing the statistical inference (Fig. 3E-H) [23]. The change in MADRS score and the RR slope were included as explanatory variables. A multiple regression model accounted for the effects of age and sex on WM. This technique, implemented in DSI Studio, computes voxel-wise Spearman rank correlations between diffusion metrics and the explanatory variables (Fig. 3I–L), disregarding the effects of age and sex on WM using a multiple regression model.
The algorithm estimated local connectomes for individual subjects and stretched them into row vectors. The vectors of a group of subjects were compiled into a single local connectome matrix Y (Fig. 3F, G), where each row represents one subject (n) and each column corresponds to local fiber orientations derived from the HCP-1065 atlas [23] (Fig. 3E, H).
Associations between local connectomes and study variables tend to continue a known fiber pathway:
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$Y\,({local\; connectome\; matrix})=X\,({matrix\; with\; study\; variables})* B\,({coefficient\; matrix})$$\end{document}
To estimate the empirical distribution of B, 5000 bootstrap resampling iterations (default setting) were applied to the row vectors of matrix X. The connectometry algorithm assesses local connectomes across varying T-score thresholds (1, 2, 3) and adjusts corresponding p-value thresholds for false discovery rate (FDR) control at 0.05, 0.075, and 0.1 as recommended in the documentation (https://dsi-studio.labsolver.org/doc/gui_cx.html). The most conservative parameter settings were selected for interpretation following visual inspection (Supplementary Fig. 2). The deterministic multi-fiber tracking algorithm implemented in DSI Studio [48] was utilized, with a manually delineated cerebellum mask designated as the termination region.
After applying 8000 random permutations to estimate the FDR correction, topology-informed pruning was iterated four times to remove potentially false-positive findings [49]. Results were located from the HCP-1065-atlas and interpreted according to the hypotheses.
Statistical analysis
The remaining statistical analyses were conducted using RStudio (2021.09.0) at significance level of α = 0.05. The change in MADRS score within 6 weeks (delta MADRS score) was calculated as 1 – post-stimulation score / pre-stimulation score. Z-standardized values > ± 2.5 were used for outlier detection of clinical changes. Median values of RR slopes were chosen for analysis to reduce within-subject variability and were used for connectometry analysis. They were tested for normal distribution using the quantile-quantile plots. Since significant differences between active and sham stimulation have been confirmed, a Pearson correlation between slopes and clinical outcome was performed (Supplementary Fig. 1B).
Results
A total of 125 patients were initially screened for participation in the study, out of which 92 met the inclusion and exclusion criteria of the trial. Of the 92 included patients, 81 successfully completed the study protocol (11.96% drop-out rate). The reasons for this were varied with medication changes, health problems independent of iTBS and symptom worsening. Of these, one subject only missed the final clinical assessment, so the neighboring MADRS value (V5) was imputed here to complete the data.
Two outliers in MADRS with (z = 4.02, z = 2.79) were removed, so that a total of 80 subjects were included in the analysis. No serious adverse events were reported during the observation period. The two treatment arms of the crossover study were comparable (active-sham n = 41, sham-active n = 39). In the stimulation effect expectation VAS, used for blinding verification, there was no significant difference between active and sham conditions (t(77) = 1.69, p = 0.09), confirming effective blinding. Additionally, no significant correlations were found between sensory discomfort or pain VAS intensity ratings and either the ΔMADRS (r = −0.07, p = 0.54) or the RR slope (r = 0.03, p = 0.79).
The relative changes in MADRS were almost identical across both arms (M ± SD_active–sham_ = 0.25 ± 0.39, M ± SD_sham–active_ = 0.34 ± 0.36). There was no significant difference in age (t(78) = 0.72 p = 0.48) and the mean age of the entire sample was 35.89 years. 33 (41.25%) of the subjects were females. The concomitant use of medications was assumed to be negligible across crossover groups (χ2(1) = 0.15, p = 0.70). The severity of symptoms in both groups significantly decreased over the entire observation period (t(78) = 7.03, p < 0.001).
The FW-DTI data achieved high data quality (Mean ± SD R^2^V1 = 0.65 ± 0.05, Mean R^2^V4 = 0.65 ± 0.05). There was extensive overlap in the previously identified relevant tracts in the baseline analysis. Also, significant longitudinal differences emerged in this exploratory analysis. Other tract results apart from the preselected ones are presented in the Supplementary Tables 1 and 2.
The primary finding was a positive correlation between changes in FA_T_ within tracts of the right cingulum and ΔMADRS. Significant negative correlations were observed in the bilateral fornices for MD_T_ and RD_T_ measurements (Fig. 4, Supplementary Table 1). Additionally, the bilateral fornices showed correlations with RR slope, while the right cingulum exhibited a greater number (104) of significant tracts.Fig. 4DTI tracts with significant correlation of FW-corrected fractional anisotropy (FA_T_), mean diffusivity (MD_T_) and radial diffusivity (RD_T_) with RR slope and delta MADRS.a correlation of baseline DTI parameters and b correlation of change of DTI parameters. Positive correlations (red) and negative correlations (blue) are shown by number of tracts (grey numbers) in the color scale. For visualization, only tract numbers >10 are labeled. All displayed tracts have p FDR < 0.05. DTI diffusion tensor imaging, FW Free-water, MADRS Montgomery-Åsberg Depression Rating Scale, HR heart rate, RR Time between two successive ventricular depolarizations, FA_T_ Free-water-corrected fractional anisotropy, MD_T_ Free-water-corrected mean diffusivity, RD_T_ Free-water-corrected radial diffusivity, Cing Cingulum, SLF Superior Longitudinal fasciculus, Uncinate Uncinate fasciculus.
In FA_T_, a substantial number of tracts (128) within the right and left cingulum were negatively correlated with RR slope. In contrast, MD_T_ and RD_T_ predominantly showed positive correlations with slope in fibers of the left cingulum (Fig. 4, Supplementary Table 1).
An increase in FA_T_ within the left cingulum significantly correlated with positive clinical outcomes. Similarly, a positive association was identified in a subset of fibers within the SLF. Conversely, a reduction in FA_T_ in a small number of fibers within the right cingulum and left fornix was associated with reductions in MADRS. Additionally, a decrease in RD_T_ in the left cingulum, as well as increases in MD_T_ and RD_T_ in the left fornix, were observed (Fig. 4, Supplementary Table 2).
An overlap was observed in a small number of fibers that were positively correlated with ΔMADRS and numerous fibers negatively correlated with RR slope and FA_T_ within the right fornix at baseline. Fibers exhibiting negative correlations of FA_T_ with RR slope at baseline coincided spatially with regions in the left fornix showing MADRS-associated FA_T_ decreases and MD_T_ increases. In both fornices, these results overlapped with tracts negatively correlated with baseline MADRS and MD_T_.
In the right cingulum, baseline analysis revealed positive associations between FA_T_ and MADRS, as well as tracts with negative correlations between RR slope and FA_T_, adjacent to regions where FA_T_ showed MADRS-related decreases. Notably, FA_T_-RR slope tracts in the right cingulum followed a more dorsal trajectory, distinct from the positive FA_T_-MADRS fibers observed in the right fornix. In contrast, findings in the left cingulum showed partial overlap between tracts exhibiting baseline FA_T_-slope correlations and those with FA_T_ increases (Table 1).Table 1. Demographic information and clinically relevant data of the study sample.All partcipants (n = 80)Active-Sham group (n = 41 (51.25%)Sham-Active group (n = 39 (48.75%)Statistical testGenderMale, Female47 (58.75%), 33 (41.25%)21 (51.22%), 20 (48.78%)26 (66.67%), 13 (33.33%)χ2(1) = 1.38, p = 0.24Age35.89 ± 13.0036.90 ± 13.6734.82 ± 12.35t(78) = 0.72, p = 0.48Age of onset23.06 ± 12.0523.55 ± 12.422.55 ± 11.82Treatment resistance31 (38.75%)15 (36.59%)16 (41.03%)Target selectionF3, Personalized40 (50%), 40 (50%),20 (48.78%), 21 (51.22%)20 (51.28%), 19 (48.72%)Baseline MADRS (V1)23.69 ± 7.4623.46 ± 7.0623.51 ± 7.95t(78) = 7.03, p < 0.001***Post-iTBS-MADRS (V6)16.04 ± 9.8116.82 ± 9.7115.23 ± 9.97Δ MADRS0.29 ± 0.380.25 ± 0.390.34 ± 0.36MedicatonMedication use58 (72.5%)31 (75.61%)27 (69.23%)χ2(1) = 0.15, p = 0.70No Medication22 (27.5%)10 (24.39%)12 (30.77%)No antidepressant3 (3.75%)0 (0%)3 (7.69%)Other antidepressant than SSRI29 (36.25%)15 (36.59%)14 (35.9%)SSRI26 (32.5%)16 (39.02%)10 (25.64%)Delta MADRS is displayed as relative change (1 – post-stimulation score / pre-stimulation score) and significant test difference is displayed as ***p < 0.001.MADRS Montgomery-Åsberg Depression Rating Scale.
Discussion
In this study, we investigated therapeutic outcomes of iTBS treatment in MDD, focusing on HR deceleration and WM free-water-corrected metrics. We found that iTBS-induced HR deceleration negatively correlated with baseline FA_T_ in the right dorsal cingulum and fornix. This finding may suggest that individuals with relatively lower WM integrity in these regions exhibit greater autonomic responsiveness to stimulation, possibly reflecting compensatory or heightened physiological adaptations in less intact pathways. In contrast, symptom alleviation measured by changes in MADRS scores positively correlated with FA_T_ in the right ventral cingulum, consistent with preserved or enhanced WM microstructure supporting clinical improvement. Inverted correlations for MD_T_ and RD_T_ were observed predominantly in the fornices, likely reflecting neurobiological processes such as increased myelination and/or reduced extracellular water content associated with improved WM integrity and neuroplasticity. Over time, increases in FA_T_ and decreases in RD_T_ in the left cingulum were significantly linked to symptom alleviation, highlighting ongoing neuroplastic remodeling as early as four weeks post-treatment. Collectively, these findings suggest that distinct microstructural features may underlie the differential modulation of autonomic function and depressive symptoms during iTBS treatment.
Role of the cingulum and fornix in therapeutic outcomes
The cingulum and fornix emerged as pivotal structures mediating the relationship between HR deceleration and therapeutic outcomes, aligning with their integral roles in the CAN and the pathophysiology of MDD [26, 50]. The fornix, known for its well-organized white matter tracts, displayed a strong association with positive treatment responses. Specifically, bilateral fornices showed higher FA_T_ alongside lower MD_T_ and RD_T_ values, which correlated with improved MADRS scores. These findings corroborate earlier studies emphasizing the role of intact myelination and white matter integrity in predicting favorable responses to MDD treatments [19, 51, 52].
Even so, a more nuanced interpretation is required given the variability in findings. For instance, [18] identified lower FA in the fornix as predictive of remission following pharmacotherapy, possibly reflecting distinct mechanisms of neural plasticity across treatment modalities. Nevertheless, the fornix’s involvement in HR modulation is consistent with its integration within the CAN, a network essential for regulating autonomic function and emotional processing [53–56].
Differential role of the cingulum in treatment response
The cingulum emerged as a critical predictor of therapeutic outcomes, with the right ventral segment showing the strongest association between higher FA_T_ and symptom alleviation. These findings align with prior work identifying elevated FA in the cingulum of treatment responders [18].
Interestingly, within the right cingulum, we observed a decrease in FA_T_ over the observation period in fiber regions that spatially overlapped with tracts where high baseline FA_T_ predicted changes in MADRS. Notably, in the same subregion of the right cingulum, though without spatial overlap, white matter properties demonstrated a negative correlation with HR deceleration during iTBS.
This heterogeneity may reflect dynamic neuroplastic processes, including alterations in axonal diameter, shifts in intra- and extra-axonal water content, or regional remodeling driven by iTBS-induced neural activity [57]. Such short-term changes in microstructural properties underscore the need for advanced imaging techniques like FW-DTI to capture subtle, region-specific alterations that are often missed by conventional DTI metrics [19, 58–60].
Mechanistic insights into observed white matter changes
The observed FA_T_ increases in the left cingulum underscore its neuroplastic potential, with changes indicative of myelination and protective remodeling occurring within just four weeks of treatment. These findings align with studies linking FA increases to learning- and stimulation-induced neuroplasticity, where myelination and oligodendrocyte activity were key contributors [61–63]. The capacity of iTBS to promote long-term potentiation (LTP)-like effects further supports this interpretation [64].
The FA_T_ increases in the left cingulum, coupled with MD_T_ and RD_T_ reductions, point to myeloproliferative processes affecting the axon diameter, consistent with enhanced myelin production and oligodendrocyte differentiation [57, 61, 65]. Conversely, decreases in FA_T_ and increases in MD_T_ and RD_T_ observed in the left fornix and right cingulum may reflect alternative neuroplastic processes, such as axonal branching, neurofilament stain or increased cellular volume, which are often associated with experience-dependent learning [20, 66].
The rapid microstructural changes induced by iTBS are unlikely to represent uniform myelination alone and may reflect transient shifts in axonal water content or extracellular matrix remodeling. The bi-tensor model used in this study provides a more granular understanding of these dynamic changes. However, multi-shell imaging or model-free reconstruction approaches could further enhance the interpretability of complex structural alterations [67, 68].
Limited predictive value of the uncinate fasciculus and superior longitudinal fasciculus
The uncinate fasciculus and SLF demonstrated limited predictive value for treatment outcomes, consistent with previous findings [16]. While a few SLF fibers showed correlations with MADRS reductions or HR deceleration, their overall contribution appeared marginal. This does not suggest irrelevance but rather highlights that their roles in depression and autonomic regulation may involve indirect or compensatory mechanisms that were not detectable in this study.
Limitations and future directions
The study’s reliance on single-shell DTI sequences limits its ability to differentiate between restricted and non-restricted diffusion, reducing the biological specificity of observed changes. Multi-shell imaging or advanced methodologies leveraging the full capabilities of generalized q-sampling imaging would provide greater insight into the underlying neurobiological mechanisms [44, 45]. Although ODFs derived from single-shell QSDR are suitable for multi-fiber tracking, their reliability in resolving complex fiber configurations—particularly in regions with low-angle kissing or crossing fibers—remains limited and requires cautious interpretation of results [69, 70]. Additionally, the absence of a sham stimulation group and the potential confounding influence of concurrent antidepressant use constrain the causal inferences that can be drawn.
Although the anterior limb of the internal capsule (ALIC) and anterior thalamic radiation (ATR) have been implicated in depression and autonomic regulation [16, 28, 71] we did not prioritize these tracts due to their subcortical depth and complex fiber architecture, which limit both rTMS reach and tractography reliability [72]. Furthermore, our whole-brain connectometry analysis showed only marginal involvement of the ALIC (Supplementary Tables 1 and 2). Future studies using higher-resolution imaging and deeper stimulation protocols may better elucidate their role.
In the current sample, heart rate deceleration demonstrated preliminary potential as a robust physiological marker of treatment efficacy (Supplementary Fig. 1B, C) [12], consistent with its role in autonomic regulation and its anticorrelation with sgACC activity [7, 24, 25]. However, emerging evidence highlights the importance of future studies controlling for confounding factors, such as respiratory sinus arrhythmia [73]. Consequently, the interplay between HR modulation, the frontal-vagal network, and subcortical structures warrants further investigation to refine its utility as a biomarker for personalized iTBS protocols.
Future studies should include longer follow-up periods to better capture sustained neuroplastic changes and assess the durability of iTBS-induced effects. In this context, the role of neuroinflammatory processes in MDD may be particularly relevant, as inflammation could influence both structural and functional brain plasticity. Finally, combining diffusion-based connectometry with functional seed-based approaches may help clarify how structural remodeling relates to changes in functional connectivity following iTBS.
Conclusion
This study highlights the intricate interplay between white matter architecture, HR modulation, and clinical outcomes in iTBS treatment for MDD. The cingulum and fornix emerged as critical predictors of therapeutic response, with observed white matter changes reflecting diverse neuroplastic processes, including myelination, axonal remodeling, and dynamic extracellular matrix shifts. While these findings enhance our understanding of iTBS’s structural correlates, further research is needed to refine mechanistic insights and improve the precision of neuroanatomical predictors.
As neuromodulatory treatments continue to evolve, the integration of advanced imaging techniques with autonomic biomarkers holds promise for tailoring interventions to individual neurobiological profiles. Such personalized approaches may improve treatment outcomes for MDD and set a precedent for precision psychiatry in other neuropsychiatric disorders. Our results underscore the relevance of specific frontolimbic tracts in mediating autonomic and antidepressant responses to iTBS and support the integration of diffusion imaging metrics into biomarker frameworks for treatment stratification.
Supplementary information
Supplementary Legends Supplementary Figure 1 Supplementary Figure 2 Supplementary Table 1: Supplementary Table 2:
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Depression and other common mental disorders: global health estimates. World Health Organization. 2017. https://iris.who.int/handle/10665/254610. Accessed 24 Jun 2024.
- 2Lipponen JA, Tarvainen MP. A robust algorithm for heart rate variability time series artefact correction using novel beat classification. J Med Eng Technol. 2019;43:173–81.10.1080/03091902.2019.164030631314618 · doi ↗ · pubmed ↗
- 3Fadnavis S, Batson J, Garyfallidis E. Patch 2Self: Denoising Diffusion MRI with Self-Supervised Learning. ar Xiv:201101355 [cs, q-bio] [preprint]. 2020. Available from: http://arxiv.org/abs/2011.01355.