Determinants of empiric combination antibiotic therapy for hospital associated bloodstream infections in the intensive care unit
Evaldas Kauzonas, Gustav Torisson, Juan Merlo, Raquel Perez, Alexis Tabah, Niccolò Buetti, Stéphane Ruckly, François Barbier, Jean-François Timsit, Fredrik Sjövall

TL;DR
This study explores factors influencing the use of combination antibiotic therapy for bloodstream infections in ICU patients across 52 countries.
Contribution
The study identifies patient, institutional, and national factors affecting empiric combination antibiotic therapy use in ICU settings.
Findings
ECAT was used in 52.5% of cases, most commonly with beta-lactams plus glycopeptides.
Immune deficiency, high SOFA scores, and ICU-level carbapenemase prevalence increased ECAT odds.
Institutional and national factors significantly influenced ECAT use, with 23.2% variation at the ICU level.
Abstract
Empiric combination antibiotic therapy (ECAT) is commonly used to treat healthcare-associated bloodstream infections (HA-BSIs) and sepsis. However, the level of supporting evidence is low and clinical practice varies significantly. We conducted a post hoc analysis using the EUROBACT-2 international cohort study database, which contained data on 2406 adult patients from 328 intensive care units (ICUs) across 52 countries, collected between June 2019 and January 2021. The main outcome was the proportion of patients receiving ECAT for HA-BSIs. Patient and institutional factors influencing the use of ECAT were examined using Markov-Chain Monte Carlo estimation. Three quarters of patients (75.2%; n = 1810) received empiric antibiotic therapy, with ECAT used in approximately half of cases (52.5%; n = 950). Most patients receiving ECAT (70.4%; n = 669) were treated with two antibiotics,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
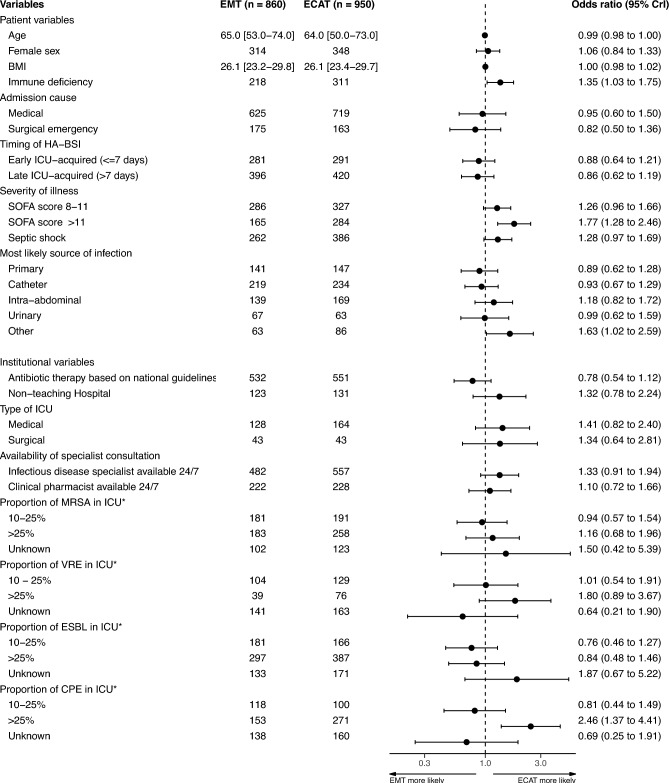 Figure 1
Figure 1- —Lund University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Use and Resistance · Nosocomial Infections in ICU · Bacterial Identification and Susceptibility Testing
Introduction
Hospital-associated infections, defined as infections presenting more than 48 h after hospitalisation, are highly prevalent in the intensive care unit (ICU)^1,2^. Hospital-associated bloodstream infections (HA-BSIs) constitute 12% of the 4.8 million annual hospital-associated infection episodes in Europe^3^.
HA-BSIs may be caused by a broad range of pathogens and present with greatly varying degrees of severity, ranging from asymptomatic bacteraemia to critical conditions such as sepsis, and are associated with high mortality rates^4,5^. Up to 30% of patients treated in ICUs present with sepsis, defined as life-threatening organ dysfunction caused by a dysregulated host response to infection^6,7^. An estimated 48.9 million cases of sepsis and 11 million sepsis-related deaths, constituting 19.7% of all global deaths annually, have been reported^8^.
The Surviving Sepsis Campaign (SSC) recommends initiating empiric antibiotic therapy within one hour in patients with a high likelihood of sepsis^9^. Indications for combining different groups of antibiotic agents can largely be classified into two groups: i) extending the spectrum of antimicrobial coverage to treat a broader range of possible causative bacteria by using broad-spectrum antibiotics with consideration for local bacterial antibiotic resistance patterns; ii) targeting suspected pathogens with different antibiotic mechanisms of action, thus increasing the total bactericidal effect.
Despite its potential benefits, ECAT has not received unequivocal support^10–13^. Excessively broad antibiotic therapy has also been associated with negative patient outcomes^14^. While potentially beneficial in cases of high-risk infections, ECAT may be associated with increased rates of adverse events and mortality when used to treat low-risk infections^10^. Antibiotic treatment practices can also be influenced by factors unrelated to individual patients, such as geographical region, traditions, local resistance patterns, and practice guidelines employed by institutions^15,16^.
The EUROBACT-2 international cohort study examined the epidemiology and outcomes of HA-BSIs in ICU patients^17^. A high-quality, international database of a broad ICU population was generated during the study process. The objective of the present study was to use the EUROBACT-2 database to examine the use of ECAT to treat HA-BSIs in the ICU and to explore patient-related and institutional factors influencing the use of ECAT.
Methods
Study design
We conducted a post hoc analysis using the EUROBACT-2 international cohort study database. The original database contained data on 2600 adult patients from 333 ICUs across 52 countries collected between June 2019 and January 2021^17^. For this study, we accessed data regarding patients who received antimicrobial therapy within the first 48 h from initial blood culturing, resulting in a dataset of 2406 adult patients from 328 ICUs across 52 countries. A list of participating countries is provided in Supplementary Table S1. All methods were performed in accordance with the relevant guidelines and regulations.
Ethics approval
The EUROBACT-2 study (ClinicalTrials.gov registration NCT03937245) was granted an initial ethical approval as a low-risk research project with waiver of individual informed consent by the Human Research Ethics Committee of the Royal Brisbane & Women’s Hospital, Queensland, Australia (LNR/2019/QRBW/48,376). Each study site then obtained ethical and governance approvals according to national and/or local regulations^17^.
Outcomes
The primary study outcomes were the proportions of patients receiving ECAT or empiric antibiotic monotherapy (EMT) for the treatment of HA-BSI. Odds ratios (ORs) with corresponding 95% credible intervals (95% CrIs) were estimated for variables that may have influenced the use of ECAT. The secondary outcomes were the number of antibiotic agents used in patients receiving ECAT and the frequencies of different antibiotic combinations used. No patient outcomes were analysed.
Definitions
The EUROBACT-2 study included adult (≥ 18 years old) patients with HA-BSI treated in the ICU^17^. HA-BSI was defined as a positive blood culture sample collected more than 48 h after hospital admission^17^. Sepsis-3 definitions for sepsis and septic shock were used^6,17^. A detailed explanation of definitions used in the study, including a flow-chart visualising the patient inclusion process (Supplementary Fig. S1), is available in ”Definitions”, Supplementary File 1.
Antibiotic therapy was classified as empiric when the following criteria were met: the primary indication was reported as empiric treatment for HA-BSI (i.e. not targeted therapy, de-escalation on the basis of antibiotic susceptibility testing, or treatment of other infections) by physicians participating in EUROBACT-2; treatment was initiated within 48 h after initial blood culture sampling. If empiric antibiotic therapy was started before initial blood culture sampling, it had to have continued during the first 48 h after blood culture sampling. Antifungal and antiviral agents were not included in the definition of empiric antibiotic therapy.
ECAT was defined as empiric therapy for HA-BSI using two or more antibiotic agents of different classes (e.g., beta-lactam plus aminoglycoside). EMT referred to the use of a single antibiotic agent. Patients receiving multiple antibiotic agents simultaneously, with only one agent used specifically for empiric treatment of HA-BSI, were classified in the EMT group. For example, a patient who received a broad-spectrum beta-lactam for empiric HA-BSI treatment while simultaneously receiving vancomycin as part of prior targeted therapy was included in the EMT group.
Immune deficiency was defined as the presence of any of the following: malignant tumours regardless of the presence of metastases, haematological malignancy, other solid tumours, previous organ transplantation, treatment with high-dose steroids, or other immunosuppression. The frequencies of the aforementioned diagnoses in the study population are presented in Supplementary Table S2.
Statistical analysis
A detailed description of the statistical methods used in the study is provided in ”Statistical Analysis”, Supplementary File 1. Patients were stratified into groups based on having received EMT or ECAT, and descriptive statistics tables were generated. Continuous variables were presented as medians with corresponding interquartile ranges. Categorical values were presented as counts and percentages.
A multilevel logistic regression model was used, with patients nested within ICUs, which were further nested within countries. Such clustering leads to statistical correlation and reduces the effective sample size^18^. Multilevel modelling accounts for this correlation, ensuring accurate estimation of uncertainty (e.g., 95% CrIs) around measures of association (e.g., ORs). From a clinical perspective, the existence of patient correlation within ICUs and countries is valuable and may reflect differences in therapeutic traditions^19^.
Markov-chain Monte Carlo (MCMC) estimation was used to assess the effects of patient and institutional factors on the odds of receiving ECAT. ORs with corresponding 95% CrIs were calculated by exponentiating the regression coefficients. The intra-class correlation coefficient (ICC), which measures the proportion of total variance attributable to higher-level clustering (e.g., ICUs or countries), was calculated^18^. Regression models containing no fixed effects, patient variables only, as well as patient and ICU variables, were compared by calculating the proportional change in variance (PCV). This approach helped distinguish whether variations in ECAT use were caused primarily by differences in patient cohorts or by contextual factors like therapeutic traditions^20^.
Variable selection
As the goal of regression modelling was exploratory in nature (as opposed to the construction of a prediction model), variables available in the EUROBACT-2 database were chosen based on their clinical relevance as determined by the study authors. Variables were excluded from the final regression analysis due to collinearity, e.g. vasopressor support was not included in the model as it is already included in the definition of septic shock.
Subgroup analyses
Subgroup regression analyses were performed based on the profile of empiric antibiotic coverage: gram-negative coverage; gram-positive coverage; anaerobe coverage; coverage for atypical pathogens.
Sensitivity analysis
A proportion of patients included in the EUROBACT-2 study received simultaneous treatment for infections other than HA-BSI. A sensitivity analysis including patients who received ECAT or EMT exclusively for the treatment of HA-BSI was performed. This was done due to the possibility that treatment of other infections, initiated prior to the onset of HA-BSI, may have affected the choice or reporting of ECAT and EMT. For example, for a patient with a new HA-BSI where ECAT with beta-lactams and aminoglycosides is indicated, and where treatment with a beta-lactam for another infection is already ongoing, the reporting physician may have reported only the initiation of EMT with an aminoglycoside (this being the only new treatment started), as opposed to registering ECAT with a beta-lactam and aminoglycoside combination (this being the actual agents exerting antimicrobial effects in vivo).
Missing data
A complete case analysis was performed due to a very low proportion of missing data.
Software
Statistical analysis was performed using the R statistical software environment (v4.4.2; R Foundation for Statistical Computing, Vienna, Austria) and MlwiN (v3.06; Centre for Multilevel Modelling, University of Bristol)^21–30^.
Results
The study database contained data on 2406 patients from 328 intensive care units across 52 countries. Patients (24.1%; n = 580) were excluded from the final analysis due to meeting at least one of the following conditions: non-empiric treatment indication, empiric antibiotic therapy administered later than 48 h after initial culture sampling, therapy with antiviral or antifungal agents only, or duplicate entries. Patients were also excluded if data were missing for any of the examined variables (0.7%; n = 16).
Three quarters of patients (75.2%; n = 1810) received empiric antibiotic therapy as per the study criteria (Table 1). ECAT was used slightly more often than EMT (52.5%; n = 950 vs. 47.5%; n = 860). Most patients (74.3%; n = 1344) were treated in the ICU due to medical causes, as compared to emergency surgery (18.7%; n = 338) or elective surgery (7.1%; n = 128). Respiratory infections were the most common primary source of HA-BSI (26.6%; n = 482). Nearly all patients included in the final analysis had sepsis (97.0%; n = 1756) and a third (35.8%; n = 648) had septic shock. The median SOFA score on day one of HA-BSI was 8 (IQR 6–11), with most patients presenting with an initial SOFA score < 8 (41.3%; n = 748), followed by those with SOFA scores of 8–11 (33.9%; n = 613), and SOFA scores > 11 (24.8%; n = 449). Immune deficiency was common in the study population (29.2%; n = 529), with active malignancy being the most common cause (Supplementary Table S2).Table 1. Characteristics of patients stratified based on treatment modality.EMTECATNumber of patients, n860950Age (median [IQR])65 [53–74]64 [50–73]Sex, n (%)Male546 (63.5)602 (63.4)Female314 (36.5)348 (36.6)BMI (median [IQR])26.1 [23.2–29.8]26.1 [23.1–29.7]Charlson comorbidity index, n (%)0264 (30.7)298 (31.4)1–2305 (35.5)324 (34.1) > 2291 (33.8)328 (34.5)Immune deficiency^†^, n (%)218 (25.3)311 (32.7)Cause of ICU-admission, n (%)Medical625 (72.7)719 (75.7)Surgical elective60 (7)68 (7.2)Surgical emergency175 (20.3)163 (17.2)Modified SAPS 2* (median [IQR])36 [26–48]36 [26.2–50]Timing of HA-BSI, n (%)Hospital-acquired183 (21.3)239 (25.2)Early ICU-acquired (**≤ **7 days)281 (32.7)291 (30.6)Late ICU-acquired (> 7 days)396 (46)420 (44.2)Likely primary source of infection, n (%)Primary141 (16.4)147 (15.5)Catheter219 (25.5)234 (24.6)Intra-abdominal139 (16.2)169 (17.8)Respiratory231 (26.9)251 (26.4)Urinary67 (7.8)63 (6.6)Other63 (7.3)86 (9.1)SOFA score^‡^, n (%) < 8409 (47.6)339 (35.7)8–11286 (33.3)327 (34.4) > 11165 (19.2)284 (29.9)Sepsis^‡^, n (%)837 (97.3)919 (96.7)Septic shock^‡^, n (%)Yes262 (30.5)386 (40.6)Source control, n (%)Not required432 (50.2)435 (45.8)Required, achieved354 (41.2)419 (44.1)Required, not achieved74 (8.6)96 (10.1)Vasopressor use^‡^, n (%)434 (50.5)606 (63.8)Respiratory support^‡^, n (%)No oxygen or low flow oxygen175 (20.3)164 (17.3)High flow oxygen nasal canula61 (7.1)56 (5.9)Non-invasive mechanical ventilation or CPAP56 (6.5)48 (5.1)Invasive mechanical ventilation568 (66)682 (71.8)Renal replacement therapy^‡^, n (%)166 (19.3)186 (19.6)ECMO^‡^, n (%)9 (1)20 (2.1)BMI body mass index, CPAP continuous positive airway pressure, ECAT empiric combination antibiotic therapy, ECMO extracorporeal membrane oxygenation, EMT empiric antibiotic monotherapy, HA-BSI hospital-associated bloodstream infection, ICU intensive care unit, SAPS 2 Simplified Acute Physiology Scale, SOFA Sequential Organ Failure Assessment, * simplified acute physiology scale II score upon admission, age variable subtracted; † prior to debut of HA-BSI; ‡ on the day of initial blood culture sampling.
The majority of patients in the ECAT group received treatment with two antibiotic agents (70.4%; n = 669) (Table 2). The most common antibiotic combination was a beta-lactam paired with a glycopeptide antibiotic (40.2%; n = 382), followed by a beta-lactam plus aminoglycoside combination (19.7%; n = 187). Among patients treated with EMT, the most common agents were piperacillin/tazobactam (29.7%; n = 255), meropenem (25.8%; n = 222), ceftriaxone (4.4%; n = 38), vancomycin (4.3%; n = 37), and imipenem/cilastatin (3.6%; n = 31).Table 2. Antibiotic combinations used for empiric combination antibiotic therapy.nProportion of ECAT (%)Proportion of total* (%)Number of antibiotic agents used266970.437321822.9124555.83 > 480.80.4Gram-negative coverageBeta-lactam + AminoglycosideTotal18719.710.3Carbapenem + Aminoglycoside626.53.4Piperacillin / Tazobactam + Aminoglycoside788.24.3Beta-lactam + QuinoloneTotal10010.55.5Carbapenem + Quinolone373.92Piperacillin / Tazobactam + Quinolone323.41.8Beta-lactam + ColistinTotal14715.58.1Carbapenem + Colistin11011.66.1Piperacillin / Tazobactam + Colistin1921Anaerobe coverageBeta-lactam + MetronidazoleTotal677.13.7Carbapenem + Metronidazole161.70.9Piperacillin / Tazobactam + Metronidazole101.10.6Lincosamide + Metronidazole30.30.2Gram positive double coverage and extended spectrumBeta-lactam + GlycopeptideTotal38240.221.1Carbapenem + Glycopeptide22223.412.3Piperacillin / Tazobactam + Glycopeptide10911.56Beta-lactam + LincosamideTotal232.41.3Carbapenem + Lincosamide101.10.6Piperacillin / Tazobactam + Lincosamide40.40.2Beta-lactam + OxazolidinoneTotal12312.96.8Carbapenem + Oxazolidinone697.33.8Piperacillin / Tazobactam + Oxazolidinone333.51.8Extended spectrum for atypical pathogensBeta-lactam + MacrolideTotal252.61.4Carbapenem + Oxazolidinone101.10.6Piperacillin / Tazobactam + Oxazolidinone70.70.4ECAT empiric combination antibiotic therapy; * proportion of total patient population included in the final analysis (n = 1810).
Most patients were treated in mixed medical-surgical ICUs (79.1%; n = 1432) in teaching hospitals (86.0%; n = 1556) (Table 3). Empiric antibiotic therapy was often informed by national/international guidelines (59.8%; n = 1083). Around-the-clock consultations by either infectious disease specialists (57.4%; n = 1039) or clinical pharmacists (24.9%; n = 450) were relatively commonly available. The reported rates of resistant bacteria (methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus spp., extended-spectrum ß-lactamase-producing Enterobacteriaceae, and carbapenemase-producing Enterobacteriaceae) varied between ICUs Table 3.Table 3. Characteristics of intensive care units participating in the EUROBACT-2 study.EMT, n (%)ECAT, n (%)Hospital academic statusNon-teaching123 (14.3)131 (13.8)Teaching737 (85.7)819 (86.2)Type of ICUMixed (medical-surgical)689 (80.1)743 (78.2)Medical128 (14.9)164 (17.3)Surgical43 (5)43 (4.5)24-h coverage by senior ICU specialist783 (91)878 (92.4)Empiric antibiotic treatment determined by national/international guidelinesYes532 (61.9)551 (58)Availability of consultations by infectious diseases specialists or clinical microbiologistNever or sporadically45 (5.2)48 (5.1)During business hours217 (25.2)216 (22.7)Scheduled multidisciplinary meetings208 (24.2)206 (21.7)Part of the permanent ICU staff137 (15.9)160 (16.8)24/7482 (56.1)557 (58.6)Availability of consultations by clinical pharmacistsNever or sporadically330 (38.4)445 (46.8)During business hours214 (24.9)206 (21.7)Scheduled multidisciplinary meetings75 (8.7)89 (9.4)Part of the permanent ICU staff154 (17.9)154 (16.2)Availability of molecular testsUsed for detection of MRSA284 (33)321 (33.8)Detection of MDR mechanism324 (37.7)388 (40.8)NA7 (0.8)3 (0.3)24/7222 (25.8)228 (24)MRSA in ICU* < 5%264 (30.7)231 (24.3)5–9.9%130 (15.1)147 (15.5)10–24.9%181 (21.1)191 (20.1)25–50%130 (15.1)178 (18.7) > 50%53 (6.2)80 (8.4)Unknown102 (11.9)123 (13)VRE in ICU* < 5%433 (50.4)431 (45.4)5–9.9%143 (16.6)151 (15.9)10–24.9%104 (12.1)129 (13.6)25–50%32 (3.7)59 (6.2) > 50%7 (0.8)17 (1.8)Unknown141 (16.4)163 (17.2)ESBL in ICU* < 5%96 (11.2)73 (7.7)5–9.9%153 (17.8)153 (16.1)10–24.9%181 (21.1)166 (17.5)25–50%210 (24.4)215 (22.6) > 50%87 (10.1)172 (18.1)Unknown133 (15.5)171 (18)CPE in ICU* < 5%367 (42.7)292 (30.7)5–9.9%84 (9.8)127 (13.4)10–24.9%118 (13.7)100 (10.5)25–50%84 (9.8)122 (12.8) > 50%69 (8)149 (15.7)Unknown138 (16.1)160 (16.8)ECAT empiric combination antibiotic therapy, EMT empiric antibiotic monotherapy, ICU intensive care unit, MRSA Staphylococcus aureus resistant to methicillin, MDR multidrug-resistance, VRE Enterococcus spp. resistant to vancomycin, ESBL Enterobacteriaceae producing extended-spectrum ß-lactamases, CPE carbapenemase producing *Enterobacteriaceae; * *percentage of bacterial species isolates within the reporting ICU resistant to the indicated antimicrobial. Patient counts are provided and stratified based on treatment with empiric combination antibiotic therapy or empiric antibiotic monotherapy.
In regression analys including all patients receiving empiric therapy, the odds of ECAT (Fig. 1) were increased by the presence of immune deficiency (OR 1.35 [95% CrI 1.03**–1.75]), SOFA scores > 11 (OR 1.77 [95% CrI 1.28–2.46]), and uncommon (reported as “other” in EUROBACT-2) primary sources of HA-BSI (OR 1.63 [95% CrI 1.02–2.59]). Admission to ICUs reporting high proportions (> 25%) of carbapenemase-producing Enterobacteriaceae (CPE) isolates doubled the odds of receiving ECAT (OR 2.46 [95% CrI 1.37–4.41]). The use of different antibiotic combinations in patients exposed to the aforementioned factors are presented in Supplementary Table S3. Other institutional factors, such as the use of national guidelines to inform antibiotic therapy, non-academic hospital status, type of ICU, or possibility of around-the-clock consultation by infectious disease specialists or clinical pharmacists, did not affect the odds of ECAT significantly.Fig. 1. Multilevel logistic regression estimations of variable effects on the odds of EMT and ECAT use. BMI body mass index,* CPE* carbapenemase producing Enterobacteriaceae,* ECAT* empiric combination antibiotic therapy,* EMT* empiric antibiotic monotherapy,* ESBL* Enterobacteriaceae producing extended-spectrum ß-lactamases,* HA-BSI* hospital-associated blood-stream infection,* ICU* intensive care unit, MRSA Staphylococcus aureus resistant to methicillin, SOFA sequential organ failure assessment ,* VRE* Enterococcus spp. resistant to vancomycin; 95% CrI 95% credible interval; * percentage of bacterial species isolates within the reporting ICU resistant to the indicated antimicrobial. Patient counts are shown for categorical variables. Median values with interquartile ranges are shown for continuous variables.
The ICC was estimated at 23.2% at the ICU-level and 4.4% at the country-level. Detailed results regarding variance components are presented in Table 4.Table 4. General contextual effects on the use of empiric combination antibiotic therapy.Model 0(variance partition component model)Model 1(patient variables)Model 2(patient + ICU variables)ECAT risk score quartile Lowest, OR (95% CrI).ReferenceReference Medium–low, OR (95% CrI).1.36 (1.01–1.84)1.33 (0.98–1.81) Medium–high, OR (95% CrI).1.94 (1.43–2.63)1.97 (1.44–2.70) High, OR (95% CrI).2.73 (2–3.72)3.87 (2.73–5.48) General Contextual Effects Country, σ² (SE)0.19 (0.21)0.27 (0.20)0.17 (0.20) ICU, σ² (SE)0.81 (0.25)0.71 (0.23)0.59 (0.22) Proportional change in variance PCV_country_, %.-3.172.56 PCV_ICU_, %.4.5827.27Intra-class correlation ICC_country_, %4.414.584.7 ICC_ICU_, %23.2422.6818.56 DIC2335.852298.542296.69 DIC change.37.311.85ECAT empiric combination antibiotic therapy, OR odds ratio; 95% CrI 95% credible interval, σ² variance, SE standard error, PCV proportional change of variance, ICC intra-class correlation coefficient, DIC deviance information criterion.
Results of regression analysis based on antibiotic coverage subgroups are presented in Table 5. In the gram-negative coverage group, immune deficiency, septic shock, and high (> 25%) prevalence of CPE and vancomycin-resistant Enterococcus (VRE) within the ICU were associated with increased odds of ECAT, whereas high (> 25%) prevalence of methicillin-resistant Staphylococcus aureus (MRSA) was associated with reduced odds.Table 5. Multilevel logistic regression estimations of variable effects on the odds of EMT and ECAT use based on antibiotic coverage subgroups.Gram-negative coverageGram-positive coverageAnaerobe coverageOR95% CrISigOR95% CrISigOR95% CrISigPatient variablesAge0.990.98 to 1.000.990.98 to 1.000.990.98 to 1.01Female sex1.020.79 to 1.310.880.68 to 1.131.520.90 to 2.57BMI10.98 to 1.0210.98 to 1.020.990.95 to 1.03Immune deficiency1.451.09 to 1.921.431.09 to 1.871.290.76 to 2.20Admission causeMedical1.530.90 to 2.611.220.74 to 2.000.640.30 to 1.38Surgical emergency1.060.59 to 1.881.120.66 to 1.900.810.36 to 1.84Timing of HA-BSIEarly ICU-acquired (≤ 7 days)0.960.68 to 1.360.850.62 to 1.181.030.57 to 1.88Late ICU-acquired (> 7 days)1.10.78 to 1.550.880.64 to 1.210.470.23 to 0.95Severity of illnessSOFA score 8–111.020.76 to 1.371.61.19 to 2.161.140.61 to 2.12SOFA score > 111.380.97 to 1.972.41.70 to 3.381.820.87 to 3.80Septic shock1.551.15 to 2.091.431.07 to 1.911.010.54 to 1.88Most likely source of infectionPrimary0.780.53 to 1.150.990.67 to 1.460.820.33 to 2.02Catheter0.830.59 to 1.161.330.95 to 1.850.410.15 to 1.15Intra-abdominal1.030.69 to 1.541.250.85 to 1.853.211.58 to 6.50Urinary1.180.73 to 1.920.890.52 to 1.510.410.10 to 1.71Other0.860.50 to 1.471.751.09 to 2.815.012.21 to 11.40Institutional variablesAntibiotic therapy based on national guidelines0.850.65 to 1.110.690.53 to 0.891.170.67 to 2.03Non-teaching hospital1.40.97 to 2.030.910.62 to 1.341.230.57 to 2.64Type of ICUMedical1.340.94 to 1.911.110.78 to 1.580.840.36 to 1.96Surgical1.030.56 to 1.901.090.60 to 1.971.480.54 to 4.08Availability of specialist consultationInfectious disease specialist available 24/70.910.70 to 1.191.421.10 to 1.850.940.54 to 1.65Clinical pharmacist available 24/70.960.70 to 1.301.040.78 to 1.390.980.53 to 1.82Proportion of MRSA in ICU^†^10–25%0.70.49 to 1.001.110.79 to 1.540.940.46 to 1.89 > 25%0.650.44 to 0.971.340.93 to 1.910.720.32 to 1.63Unknown3.031.21 to 7.640.630.28 to 1.390.230.06 to 0.96Proportion of VRE in ICU^†^10–25%1.250.83 to 1.880.960.64 to 1.440.320.09 to 1.10 > 25%2.341.36 to 4.031.791.07 to 2.992.450.98 to 6.12Unknown0.390.19 to 0.770.960.54 to 1.701.130.36 to 3.56Proportion of ESBL in ICU^†^10–25%0.80.55 to 1.1610.69 to 1.460.930.42 to 2.04 > 25%1.010.68 to 1.511.050.71 to 1.560.810.33 to 1.97Unknown1.410.63 to 3.132.21.07 to 4.522.960.96 to 9.12Proportion of CPE in ICU^†^10–25%1.10.72 to 1.690.760.49 to 1.160.90.32 to 2.50 > 25%3.212.16 to 4.762.221.52 to 3.253.091.30 to 7.32Unknown0.870.40 to 1.890.960.49 to 1.902.010.64 to 6.33BMI body mass index, CPE carbapenemase producing Enterobacteriaceae, ECAT empiric combination antibiotic therapy, EMT empiric antibiotic monotherapy, ESBL Enterobacteriaceae producing extended-spectrum ß-lactamases, HA-BSI hospital-associated blood-stream infection, ICU intensive care unit, MRSA Staphylococcus aureus resistant to methicillin, OR odds ratio, Sig statistical significance, SOFA Sequential Organ Failure Assessment, VRE Enterococcus spp. resistant to vancomycin; 95% CrI 95% credible interval; * the estimated 95% credible interval does not include 1; † percentage of bacterial species isolates within the reporting ICU resistant to the indicated antimicrobial. Patient counts are shown for categorical variables. Median values with interquartile ranges are shown for continuous variables.
In the gram-positive group, higher odds of ECAT were observed in patients with immune deficiency, high SOFA scores, septic shock, and uncommon (“other”) infection sources, as well as in ICUs with high (> 25%) rates of VRE and CPE and 24/7 infectious diseases specialist consultation availability. Use of national guidelines to guide antibiotic therapy reduced the odds within this group.
Among patients receiving anaerobe coverage, ECAT was associated with intra-abdominal or uncommon (“other”) infection sources and high (> 25%) CPE prevalence but was less likely when HA-BSI occurred more than 7 days after ICU admission.
Unknown rates of resistant organisms (Enterobacteriaceae producing extended-spectrum beta-lactamases (ESBL), MRSA, VRE) were also associated with altered odds of ECAT, with effects varying by antibiotic coverage group. Analysis including only patients receiving coverage for atypical pathogens could not be conducted due to model instability related to small sample size.
The results of sensitivity analyses including patients who received empiric antibiotic therapy exclusively for the treatment of HA-BSI are presented in Supplementary Table S4 and Supplementary Fig. S2. A total of 287 and 177 patients received ECAT and EMT respectively (15.9% and 9.8% of patients in the respective groups that were included in the final analysis). The odds for ECAT were increased by the presence of immune deficiency. The odds for ECAT were lower in patients receiving treatment for HA-BSI acquired soon after ICU admission (within 7 days).
Discussion
The proportions of patients treated with ECAT and EMT were relatively equal and consistent with previously published data^31^. The most common combination used for ECAT included beta-lactams and glycopeptide antibiotics, also confirming recent findings^13^. The finding indicates that ECAT is more commonly used to broaden the spectrum of coverage during the empiric phase of therapy. This is opposed to achieving greater treatment efficacy due to antibiotic synergism against specific pathogens, such as when beta-lactams and aminoglycoside antibiotics are combined to treat infections caused by gram-negative bacteria^32^.
Our findings revealed that immune deficiency, higher SOFA scores at presentation of HA-BSI, and uncommon primary sources of infection increased the odds of ECAT being used. While septic shock was more prevalent in the ECAT group (40.5% vs. 30.5%), it did not significantly increase the odds of ECAT. This may be explained by the broad definition of septic shock, which fails to differentiate between patients with low-dose vasopressor support, and those with severe shock requiring high-dose vasopressors. Infection sources classified as “other” referred to sources other than primary, respiratory, catheter, intra-abdominal, or urinary. This is a heterogenous group and represents infections with scarce possibilities of source control, such as bone and cardiac infections.
The general trend of using ECAT to treat patients at higher risk observed in our study aligns with previous results, demonstrating potential benefits in treating high-risk infections^10^. However, a more recent systematic review with meta-analysis did not reveal any benefit or harm when comparing ECAT to EMT in adult ICU patients with severe sepsis^12^. Recently published results cast further doubts on the benefits of ECAT in terms of patient outcomes^13,14,33^.
Considering the uncertain benefits of ECAT, its potential harms, such as nephrotoxicity, ototoxicity, superinfections, and deleterious effects on commensal microbiotas, should be considered^11,34^. As timely de-escalation of therapy based on antibiotic susceptibility testing results is a key component of antibiotic stewardship, exposure to broad-spectrum antibiotics should be limited to avoid potential development of antibiotic resistance^35^. However, the DIANA study and data from the European Centre for Disease Prevention and Control indicate that only 4–16% of empiric antimicrobial therapy regimens are de-escalated within the first three days, indicating that the practice has not been widely adopted in ICUs worldwide^3,31^. Delays in initiating adequate antibiotic therapy may lead to increased mortality rates, which likely contributes to reluctance to de-escalate antibiotic therapy^9,14^. The EUROBACT-2 study indicated that only 51.5% of patients received adequate therapy within 24h of blood culture sampling, and that time to adequate therapy increased with antibiotic resistance^17^. The increased odds of ECAT being used in ICUs where a high proportion of Enterobacteriaceae isolates produce carbapenemases likely reflect the difficulty of combating infections in regions with a high prevalence of resistant micro-organisms, where standalone therapy with common broad-spectrum agents, such as carbapenems, is rendered ineffective^36^.
The impact of institutional and regional factors, such as the availability of therapeutic drug monitoring, antimicrobial resistance surveillance, and intermediate care, on 28-day mortality rates among ICU patients was described in a recent study^37^. Our findings further highlight the interplay between patient-specific factors and external variables, such as antimicrobial resistance patterns, which must be accounted for when choosing antimicrobial therapy regimens. The calculated ICCs indicate that 23.2% and 4.4% of the variance in ECAT use was attributable to ICU-related and national variables, respectively. Values exceeding 10% indicate substantial clustering, highlighting the influence of institutional or national contexts on clinical practice^38^. Subgroup analyses based on empiric treatment coverage further illustrate the impact of both patient-related and institutional factors on treatment choice. The odds of ECAT use were significantly influenced by the rates of antibiotic-resistant bacterial isolates within ICUs in all subgroups. In addition, the use of national guidelines to inform antibiotic therapy decreased, while the 24/7 availability of infectious disease specialist consultations increased the odds of ECAT for patients receiving empiric therapy with gram-positive coverage.
However, the ICC does not provide information regarding which variables should be included in regression models to explain the observed variance. This implies that the collection of data regarding contextual factors should be an integral part of future study designs. Implementing such an approach would provide more accurate results regarding patient-level variables by accounting for clustering and allow for simultaneous evaluation of institutional and national factors that affect clinical practice. This would facilitate comparisons of differing practices in multi-centre studies and aid clinicians in developing best-practice recommendations, as well as policy makers in prioritising development of healthcare infrastructure.
The present study has several strengths. The database generated during the EUROBACT-2 study contains recent, high-quality data with minimal missing values for a broad, international population of ICU patients, and provides a global overview of intensive care practice. The analysis involved the use of variables and risk scores relevant to daily clinical practice. The multilevel approach to regression analysis accounted for the natural clustering of patients within hospitals and provides more accurate standard errors, thus lowering the risk of false positive results.
Thestudy has multiple limitations. The EUROBACT-2 study included only patients with positive blood cultures, potentially limiting the generalisability of our findings^17^. However, our study examined treatment initiated prior to the availability of results from the first positive blood culture, enabling the examination of factors associated with treatment decisions made during the empiric phase. An exploratory analysis of heterogeneous ICU patient data generated during a study not originally designed for the assessment of ECAT determinants introduces the risk for unmeasured confounders and further limits generalisability. Only variables included in the EUROBACT-2 database could be evaluated, thus excluding potential predictors of interest. The definition of empiric antibiotic therapy used in the study relied heavily on the indications and timing of initiation reported by participating physicians. Extrapolation towards a definition not established during the original study introduces the risk of inaccurately assigning patients to the ECAT and EMT groups. Regression variables were selected based on availability and clinical relevance as determined by the study authors, which may be considered subjective compared with other, data-driven approaches. The results of the regression analysis should be interpreted with caution, as model fit was not optimal (Supplementary Fig. S3 and Supplementary Fig. S4). In addition, as the frequencies of both ECAT and EMT were close to 50%, odds ratios may have been overestimated. Although the regression analysis accounted for the clustering of ICUs within countries, no national-level variables were included in the model, as no publicly available predictors relevant to our study were identified. Another significant limitation is the large proportion of patients who received antibiotic therapy for other infections alongside the HA-BSI treatment analysed in our study. We attempted to mitigate bias by performing sensitivity analyses including patients who received antibiotic treatment for HA-BSIs exclusively. Lastly, patients receiving treatment for infections such as endocarditis, where ECAT is part of routine therapy, were not excluded, which may have affected the regression analysis results.
In conclusion, factors at the individual, institutional, and national levels may affect the decision to use empiric combination antibiotic therapy to treat hospital-associated bloodstream infections. Given the impact of institutional and national variables on empiric combination antibiotic therapy use and the inconclusive evidence regarding its potential risks and benefits, it is of great importance that treatment is tailored to the specific needs of the individual patient.
Supplementary Information
Supplementary Information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1European Centre for Disease Prevention and Control. Point Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use in European Acute Care Hospitals, 2022–2023. https://data.europa.eu/doi/10.2900/88011 (2024).
- 2European Centre for Disease Prevention and Control. Healthcare-Associated Infections Acquired in Intensive Care Units - Annual Epidemiological Report for 2020. https://www.ecdc.europa.eu/en/publications-data/healthcare-associated-infections-acquired-intensive-care-units-annual (2024).
- 3R Core Team. R: A Language and Environment for Statistical Computing. https://www.R-project.org/ (2023).
- 4R Studio Team. R Studio: Integrated Development Environment for R. http://www.rstudio.com/ (2020).
- 5Yoshida, K. et al. tableone: Create ‘Table 1’ to Describe Baseline Characteristics with or without Propensity Score Weights. (2022).
- 6Wickham, H. et al. readxl: Read Excel Files. (2025).
- 7Bates, D. et al. lme 4: Linear Mixed-Effects Models using ‘Eigen’ and S 4. (2025).
- 8Paul, M., Lador, A., Grozinsky-Glasberg, S. & Leibovici, L. 2014 Beta lactam antibiotic monotherapy versus beta lactam-aminoglycoside antibiotic combination therapy for sepsis. Cochrane Database Syst. Rev.201810.1002/14651858.CD 003344.pub 3PMC 651712824395715 · doi ↗ · pubmed ↗