Radiofrequency catheter ablation-associated silent iatrogenic right ventricular pseudoaneurysm: a case report and literature review
Shogo Haruki, Hiroyuki Yamamoto

TL;DR
This case report describes a rare complication of radiofrequency catheter ablation causing a right ventricular pseudoaneurysm, successfully diagnosed and treated with imaging and surgery.
Contribution
Highlights a rare iatrogenic cause of right ventricular pseudoaneurysm and emphasizes the role of cardiac computed tomography angiography in diagnosis.
Findings
RFCA can lead to iatrogenic right ventricular pseudoaneurysm.
Cardiac computed tomography angiography is effective in diagnosing RVP.
Surgical repair successfully treated the pseudoaneurysm in this case.
Abstract
Right ventricular pseudoaneurysm (RVP) encased by adjacent pericardial or scar tissue is rare but can be a fatal sequela of cardiac rupture. Differentiating between pseudoaneurysms and true aneurysms is important because they have different natural histories and require distinct treatments. Radiofrequency catheter ablation (RFCA) is a potential cause of RVP; however, RFCA-associated RVP incidence and management remain unclear. An 88-year-old woman with refractory paroxysmal supraventricular tachycardia was admitted to our hospital. We performed an electrophysiological study, which led to a final diagnosis of atrioventricular nodal reentrant tachycardia, for which successful RFCA was performed. On post-procedural day 2, echocardiography revealed a small right ventricular apical outpouching. Cardiac computed tomography angiography led to the correct diagnosis of RVP, which was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
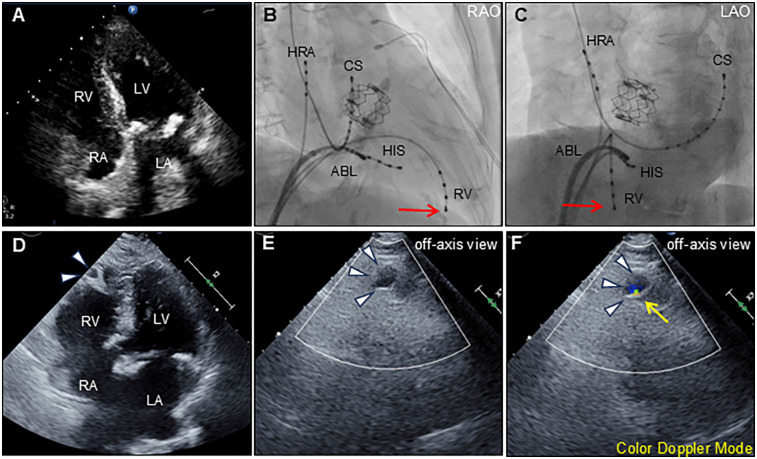 Figure 1
Figure 1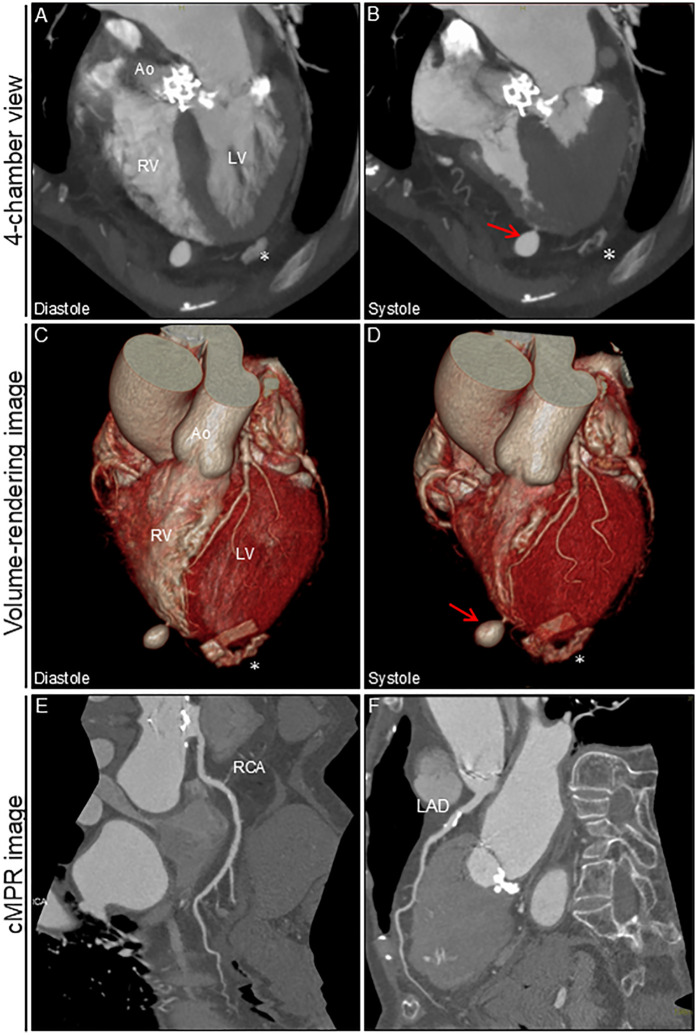 Figure 2
Figure 2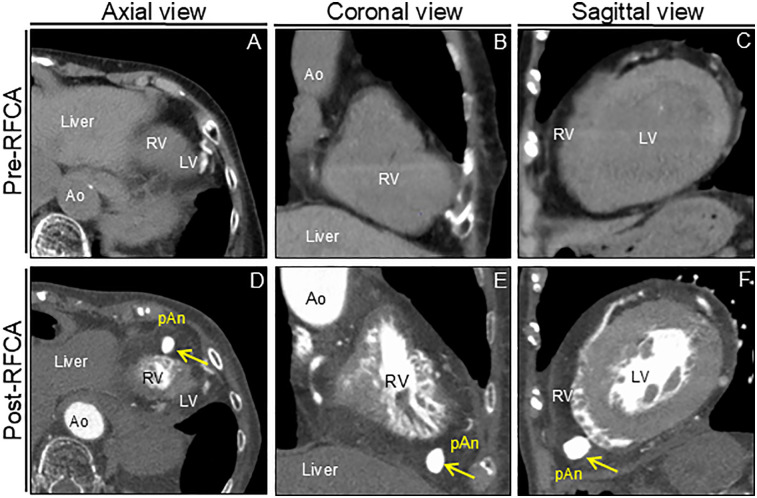 Figure 3
Figure 3| Case | Author | Age/Sex | Underlying disease | Trigger factor | Cardiac aneurysm | Management | Outcome | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (y) | Type | Anatomy | Location | Size (mm) | PE | Clinical manifestation | Time-to-onset | ||||||
| 1 | Salazer et al. ( | 31/M | WPW | Lateral free wall accessory pathway | P | LV | Left lateral atrioventricular groove near the coronary sinus | 20 | Absence | Cardiac murmur | PPD 3 months | SR | Survival |
| 2 | Mabo et al. ( | 49/M | WPW | Posterior accessory pathway | P | LV | Posterior mitral annuls | NA | Absence | None | PPD 2 months | SR | Survival |
| 3 | Gill et al. ( | 69/F | WPW | Concealed Kent posterior submitral | P | LV | Submitral in the posterolateral region of LV | NA | Absence | None | PPD 2–3 days | Con | Complete resolution at 1-month follow-up |
| 4 | Wolf et al. ( | 49/F | WPW/VT | RFCA for VT | P | RV | RV outflow tract | 10 × 10 × 10 | Presence | Sudden cardiac death | PPD 9 months | CPR | Died |
| 5 | Benezet-Mazuecos et al. ( | NA | OMI | RFCA for OMI-related VT | T | LV | Apex | NA | Absence | NA | PPD 2 days | Med | Survival |
| 6 | Mansour et al. ( | 50/M | WPW | Left lateral bidirectional accessory pathway | P | LV | Basal lateral wall under the mitral annulus | 30 × 40 | Absence | Syncope | PPD 15 years | SR | Survival |
| 7 | Miura et al. ( | 57/M | WPW | RFCA for WPW | P | LV | Posterolateral mitral annuls | 15 × 15 | Presence | Cardiogenic shock | During RFCA | SR | Survival |
| 8 | Han et al. ( | 27/M | AF | RFCA for AF | P | MAIVF | MAIVF | NA | Absence | None | PPD 1 month | Con | No change at 4-year follow-up |
| 9 | Koruth et al. ( | 63/M | VT | Epicardiac puncture | P | RV | Mid-RV free wall | 13 × 10 × 9 | Absence | CP | After procedure | Con | Complete resolution after few weeks |
| 10 | Koch et al. ( | 60s/F | VT | RFCA for VT | P | LV | Inferior wall extending into posterolateral wall | 90 | Presence | ICD inappropriate shock | PPD 8 months | SR | Survival |
| 11 | Han et al. ( | NA | AF | RFCA for AF | P | NA | NA | NA | Absence | None | PPD 1 month | NA | Partial resolution |
| 12 | Auriau et al. ( | Young/F | WPW | Left posterolateral accessory atrioventricular pathway | P | LV | Lateral wall near the circumflex artery and the mitral annulus | 37 × 44 | Absence | Palpitation, faintness and dyspnea | PPD 12 years | SR | Survival |
| 13 | Dandamudi et al. ( | 52/F | PVC | RFCA for LV summit PVC | P | LV | Basal anterior wall | 24 × 24 | Presence | Cardiogenic shock | PPD 5 weeks | SR | Survival at 5-month follow-up |
| 14 | Kim and Lee ( | 39/M | WPW | RFCA for WPW | P | LV | Posterior mitral annuls | 27 × 17 | Presence | Syncope and CP | PPD 12 days | Con | No change at 1-year follow-up |
| 15 | Wang et al. ( | 69/M | PVC | RFCA for PVC | P | LV | Inferior wall near the mitral annulus along the left atrium | 90 × 40 | Presence | Dizziness and CP | PPD 2 days | SR | Survival |
| 16 | Watanabe et al. ( | 60/M | VT | RFCA for VT | P | LV | Left ventricular outflow tract | NA | Absence | CP | During RFCA | Med | Improved |
| 17 | Fritz et al. ( | 59/M | PVC | RFCA for PVC | P | LV | Basal inferior wall | NA | Presence | Syncope and dyspnea | During RFCA | SR | Survival |
| 18 | Nicolazzi et al. ( | 38/F | VT | Fascicular VT target to posterior lateral papillary muscle | P | LV | Mid inferior wall | 20 × 14 | Absence | Fatigue, palpitations, GI symptoms | PPD 1 month | SR | Survival |
| 19 | Kim et al. ( | 74/F | VT | RFCA for VT from posteromedial papillary muscle | P | LV | Posteromedial papillary muscle | 26 × 9 | Absence | None | PPD 2 months | Con | No change at 1-year follow-up |
| 20 | Kasai et al. ( | 82/M | PVC | RFCA for PVC | P | LV | Posterior papillary muscle | 12 × 11 | Absence | None | PPD 1 month | Con | No change at 3-month follow-up |
| 21 | Korkmaz et al. ( | 69/M | PVC | RFCA for PVC | T | LV | Basal middle septum | NA | Absence | VT | PPD 1 year | Con | Survival |
| 22 | Izekor et al. ( | 72/M | PVC | RFCA for PVC | P | LV | Anterolateral wall | 19.5 | Absence | Palpitation | PPD 34 days | SR | Survival |
| 23 | Manongi et al. ( | 80s/F | PAF | Coronary sinus catheter | P | RA | RA appendage | NA | Presence | None | PPD 2 days | Con | Symptom resolution at 3-month follow-up |
| 24 | Present case | 88/F | SVT | RV catheter | P | RV | Apex | 9.6 × 12.1 | Absence | None | PPD 3 days | SR | Survival |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Structural Anomalies and Repair · Infective Endocarditis Diagnosis and Management · Mechanical Circulatory Support Devices
Highlights
•Right ventricular pseudoaneurysm (RVP) is potentially fatal if left untreated.•Silent iatrogenic RVP may develop following radiofrequency catheter ablation.•Cardiac computed tomography angiography is valuable for diagnosis of RVP.
Introduction
1
Ventricular pseudoaneurysms may occur in association with myocardial infarction, trauma, infection, catheter-related procedures, cardiac surgery, or idiopathic (1). Cardiac pseudoaneurysms often occur in the left ventricle, whereas right ventricular pseudoaneurysms (RVP) are rare (2). We describe a unique case of silent iatrogenic RVP secondary to radiofrequency catheter ablation (RFCA).
Case description
2
An 88-year-old woman was admitted with symptomatic paroxysmal supraventricular tachycardia that had persisted for three years. The patient had a history of severe aortic stenosis for which transapical transcatheter aortic valve replacement was performed seven years ago. Her initial vital signs were blood pressure of 79/60 mmHg and heart rate of 164 beats/min. The physical examination findings were unremarkable. Laboratory test revealed elevated serum level of brain natriuretic peptide (171.6 pg/ml, reference: <18.4 pg/ml). Electrocardiography revealed narrow QRS tachycardia with a short RP (Supplementary Figure S1A). Tachycardia was terminated with rapid intravenous administration of adenosine triphosphate (Supplementary Figure S1B). However, the patient experienced frequent paraoxymal supraventricular tachycardia episodes. Echocardiography revealed no structural or functional heart abnormalities (Figure 1A; Supplementary Video S1). Unenhanced computed tomography scans showed no biventricular abnormalities suggestive of myocardial infarction or aneurysm. An electrophysiological study was performed four days after admission. Catheters were placed in the high right atrium, the His bundle region, coronary sinus, and right ventricular (RV) apex. Premature ventricular contractions frequently occurred during RFCA, and, hence, the RV pacing catheter was held tightly to avoid the unintended catheter movement. Based on the electrophysiological study, slow/fast atrioventricular nodal reentrant tachycardia was diagnosed. Subsequent successful anatomical slow-pathway ablation was performed according to standard techniques (Figures 1B,C). We excluded any complications, including cardiac tamponade, on postprocedural echocardiography. Follow-up echocardiography revealed RV apical outpouching on postprocedural day 2 (Figures 1D–F; Supplementary Video S2). The patient was asymptomatic, and her vital signs were stable. Physical examination and electrocardiographic findings were unremarkable (Supplementary Figures S1C,D). Follow-up laboratory tests were close to normal. Differential diagnoses of ventricular outpouching include true aneurysms and pseudoaneurysms. Cardiac computed tomography angiography (CCTA) further characterized the morphology and features of the RV apical outpouching (Figures 2A–D). Note the presence of contrast-filled RV outpouching at the apex that protruded during systole, with a maximum diameter of 12.1 mm and a narrow orifice of 1.5 mm with an orifice-to-maximum diameter ratio of 12.4%, suggestive of RVP. CCTA revealed normal coronary arteries (Figures 2E,F). Pericardial effusion was not observed. A detailed review of the computed tomography images confirmed the absence of RVP before the RFCA procedure and its presence after the procedure (Figure 3). Given the temporal relationship between RFCA and the occurrence of RVP without any other identifiable cause, a final diagnosis of iatrogenic RVP was made. After multidisciplinary discussion, taking into consideration that a ventricular pseudoaneurysm is susceptible to cardiac rupture, the patient underwent urgent surgical repair of the RVP. No bleeding was observed in the pericardial sacs. There was no evidence of pericarditis, intrapericardial bleeding, or cardiac rupture except for a slight bulge at the RV apex. Epicardial echocardiography was used to identify the pseudoaneurysm, as such pseudoaneurysm was difficult to identify by visual examination. Subsequent vertical mattress suture repair with Teflon-felt reinforcement was performed for the RVP. The patient's postoperative course was uneventful, and she remained asymptomatic at the one-year follow-up (Supplementary Figure S2).
Transthoracic echocardiography and ablation images. Preprocedural transthoracic echocardiography (apical 4-chamber view) shows normal biventricular function with normal anatomy (A) Radiographs of the right anterior oblique [RAO; (B)] and left anterior oblique [LAO; (C)] views show the radiofrequency ablation catheter (ABL) positioned at the posterior right atrial septum. Other catheters were positioned at the high right atrium (HRA), His-bundle (HIS), coronary sinus (CS), and right ventricle (RV). Red arrows indicate the tip of the indwelling RV catheter. Postprocedural transthoracic echocardiography (apical 4-chamber view) reveals an outpouching of the right ventricular apex (arrowheads) (D) Color Doppler echocardiography using an off-axis view reveals outpouching of the right ventricular apex (arrowheads) during diastole (E) and systole (F) The expansion with the antegrade flow at systole, suggests communication between the outpouching and right ventricle (yellow arrow). LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.
Cardiac computed tomography angiography image after ablation. 4-chamber view and volume-rendering images during diastole (A,C) and systole (B,D). Outpouching with a narrow neck at the apex of the right ventricle is markedly prominent during systole (arrows). No significant pericardial effusion was observed. cMPR images of RCA (E) and LAD (F) * Denotes the remnants of felt in the left ventricular apex after transapical aortic valve replacement. Ao, aorta; cMPR, curved multi-planar reformation; LAD, left anterior descending artery; LV, left ventricle; RCA, right coronary artery; RV, right ventricle.
Computed tomography images before and after RFCA. Preprocedural unenhanced computed tomography images confirm normal right ventricular anatomy (A–C). Postprocedural cardiac computed tomography angiography images reveal apical outpouching of the right ventricle (arrows) (D–F). Ao, aorta; LV, left ventricle; pAn; pseudoaneurysm; RFCA; radiofrequency catheter ablation; RV, right ventricle.
Discussion
3
Here, we describe a unique case of silent iatrogenic RVP after RFCA. Our case provides the following clinical lessons: We reviewed the previously reported cases of RFCA-associated cardiac aneurysms (3–25), which were published in English in PubMed between 1985 and 2024 (Table 1). The left ventricle was the most common site of origin of the cardiac aneurysm, followed by the right ventricle, mitral-aortic intervalvular fibrosa, and right atrium. As in previous studies (26), nearly 30% of the patients had no clinical symptoms. The literature documents the triggers, characteristics, management, and outcomes of RVP after RFCA in two cases (6, 11). Notably, RVP developed at a site far from the ablation target site in the present case. Given the histological nature of the RV, which is composed of fragile pectinate muscles with wall thinning, age-related RV myocardial degeneration, physical stress on the RV myocardium due to prior temporary pacing wire placement and improper manipulation of the RV catheter tip might have triggered the RVP. Thus, for medical specialists in RFCA, recognizing these rare RFCA-related complications may aid in early detection and proper management. CCTA with good temporal and spatial resolutions can clearly differentiate ventricular outpouchings (27). Ventricular pseudoaneurysms are characterized by a narrow opening that connects to the cardiac chamber. Pseudoaneurysms expand outward in response to the increased intraventricular pressure during systole. Indeed, CCTA was valuable for the accurate diagnosis of silent iatrogenic RVP in the present case. There are currently no guidelines for the appropriate management of ventricular pseudoaneurysms. Given the high risk of cardiac rupture, surgical repair has been considered the first-line treatment of choice for ventricular pseudoaneurysms (1). Although surgical repair was performed, there was no evidence of impending cardiac rupture in the present case. Considering the high surgical mortality rate of 7%–23% (28), conservative management to reduce the risk of cardiac rupture might be another treatment option (26, 29). Percutaneous embolization with coils offers another promising therapeutic alternative, limited to midterm outcomes (29, 30). Owing to the nature of our hospital, which did not have an experienced interventionalist but had many experienced cardiac surgeons on staff, we decided to opt for surgical treatment in this case. Moreover, in our review, nearly half the patients received conservative management with a favorable prognosis. Noninvasive treatment strategies may be feasible in elderly patients with stable hemodynamics and no risk of cardiac rupture. Data on the long-term outcomes of the above treatments is lacking, and future evidence is awaited to be built up through data accumulation.
Iatrogenic cardiac pseudoaneurysm have been reported in various clinical reports. Left ventricular pseudoaneurysms (LVPs) are the most frequent type of iatrogenic cardiac pseudoaneurysm, with approximately one-third arising from surgical procedures involving mitral valve replacement (1). Percutaneous device interventions predominantly including transapical transcatheter aortic valve replacement can often cause iatrogenic LVP (31, 32). Cases of transcatheter mitral valve implantation and ventricular septal defect closure device-related LVP (33, 34) have also been reported. Although iatrogenic RVPs are very rare, various case reports describe them in connection with endomyocardial biopsy (35), lead extraction (36), pericardiocentesis (30), Swan-Ganz catheter (37), valve in valve treatment of tricuspid valves (38), placement of a hemodialysis catheter (39), surgery for atrio-ventricular septal defect with tetralogy of Fallot (40) and insertion of central venous line (41). Considering the above diverse case reports, our case highlights that RVP can complicate even a routine procedure.
Limitation
4
Our case was finally diagnosed as iatrogenic RVP based on the temporal relationship between RFCA and evidence of de novo RVP, but the direct causal relationship and detailed mechanism remain unclear. In addition, histological analysis could not be performed in this case. Early onset and the absence of reactive pericardial effusion observed in our case suggests that it may have been a specific subtype of RVP with residual cardiomyocytes that are vulnerable but have not yet ruptured. Future systematic and comprehensive pathological analyses of RFCA-associated ventricular aneurysms are warranted.
Conclusions
5
This is a rare case of silent iatrogenic RVP after RFCA. This case report highlights the importance of recognizing iatrogenic RVP and the clinical significance of CCTA for diagnosis of RVP. Therefore, clinicians should be aware of RVP as a possible complication after RFCA and understand the imaging techniques useful for its early diagnosis and determine appropriate treatment options.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Frances C Romero A Grady D. Left ventricular pseudoaneurysm. J Am Coll Cardiol. (1998) 32:557–61. 10.1016/s 0735-1097(98)00290-39741493 · doi ↗ · pubmed ↗
- 2Csapo K Voith L Szuk T Edes I Kereiakes DJ. Postinfarction left ventricular pseudoaneurysm. Clin Cardiol. (1997) 20:898–903. 10.1002/clc.49602010219377830 PMC 6655895 · doi ↗ · pubmed ↗
- 3Salazer TL Bacharach JM Bresnahan JF Seward JB Danielson GK. Fistulous pseudoaneurysm complicating surgical accessory pathway interruption for wolff-Parkinson-white syndrome. Mayo Clin Proc. (1992) 67:663–6. 10.1016/s 0025-6196(12)60722-81434901 · doi ↗ · pubmed ↗
- 4Mabo P Le Breton H De Place C Daubert C. Asymptomatic pseudoaneurysm of the left ventricle and coronary artery fistula after closed-chest ablation of an accessory pathway. Am Heart J. (1992) 124:1637–9. 10.1016/0002-8703(92)90089-e 1462930 · doi ↗ · pubmed ↗
- 5Gill KS Bansal RC Pai S Timothy P. Left ventricular pseudoaneurysm as a complication of electrophysiologic study. J Am Soc Echocardiogr. (2001) 14:228–30. 10.1067/mje.2001.10854011241019 · doi ↗ · pubmed ↗
- 6Wolf DA Burke AP Patterson KV Virmani R. Sudden death following rupture of a right ventricular aneurysm 9 months after ablation therapy of the right ventricular outflow tract. Pacing Clin Electrophysiol. (2002) 25:1135–7. 10.1046/j.1460-9592.2002.01135.x 12164457 · doi ↗ · pubmed ↗
- 7Benezet-Mazuecos J Marcos-Alberca P Farre J. Images in cardiology: giant left ventricular thrombus after radiofrequency ablation of post-infarction ventricular tachycardia: what to do? Heart. (2005) 91:1532. 10.1136/hrt.2004.05960016287735 PMC 1769203 · doi ↗ · pubmed ↗
- 8Mansour F Basmadjian AJ Bouchard D Ibrahim R Guerra PG Khairy P. Images in cardiovascular medicine. Left ventricular pseudoaneurysm: a late complication of low-energy DC ablation. Circulation. (2006) 113:e 780–1. 10.1161/CIRCULATIONAHA.105.59100816735682 · doi ↗ · pubmed ↗