Circulating prothymosin alpha and immunoglobulin G3 in acute rheumatic fever and rheumatic heart disease: A case-control study
Gul Afshan, Nicole Tsui, Humera Javed, Tehmina Kazmi, Emma Ndagire, Jafes Pulle, Kristin Huse, Amelia Lias, Shagorika Talukder, Natalie Lorenz, Reuben McGregor, Craig Sable, Andrea Z. Beaton, Nicole J. Moreland, Emmy Okello, Masood Sadiq, Tom Parks

TL;DR
This study compares blood markers in patients with acute rheumatic fever and rheumatic heart disease to find better diagnostic tools.
Contribution
The study provides new evidence on IgG3 as a potential diagnostic marker for acute rheumatic fever in low-resource settings.
Findings
Total IgG3 was significantly elevated in definite ARF compared to controls, possible ARF, and chronic RHD.
PTA levels were similar across groups, contradicting a previous report of elevated PTA in RHD.
IgG3 elevation in ARF was observed in both serum and plasma samples from different regions.
Abstract
The lack of specific diagnostic tests for acute rheumatic fever (ARF) and its consequence rheumatic heart disease (RHD) is a key barrier to effective control of these diseases in low resource settings. We used immunoassays to evaluate blood prothymosin alpha (PTA) and immunoglobulin G3 (IgG3) in patients with ARF, RHD and controls using serum samples from Pakistan and plasma samples from Uganda. Across both sets of samples, we found total IgG3 was significantly elevated in definite ARF (n = 24) compared to controls (n = 36), possible ARF (n = 15) and chronic RHD (n = 11). Whether measured in serum or plasma, PTA levels were similar across these groups. Our findings conflict with a previous report that found PTA was elevated in RHD compared to healthy controls. In contrast, while less marked than before, we found IgG3 was elevated in ARF, extending this observation to settings where…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
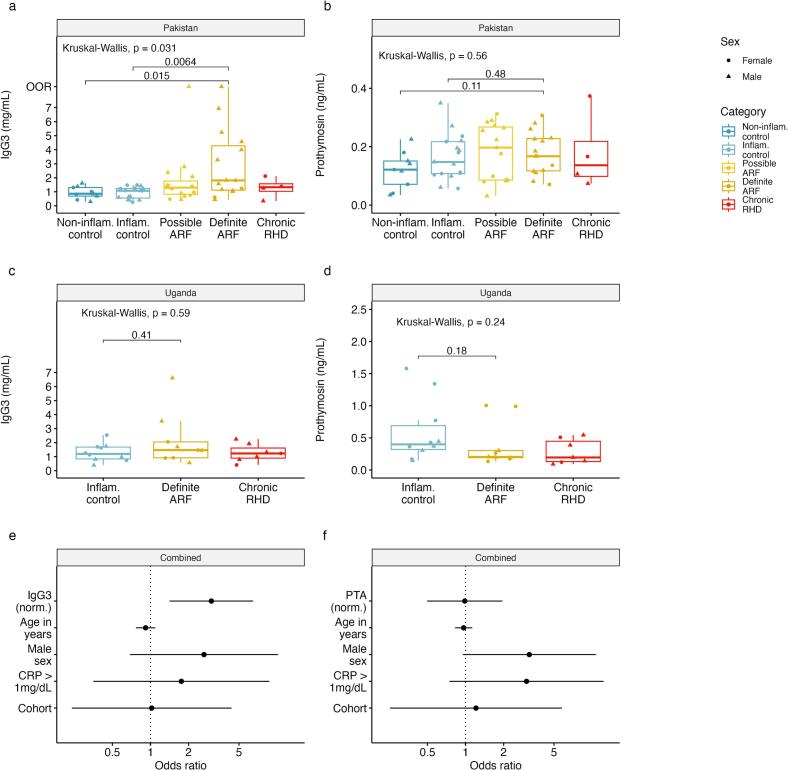 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments · Inflammasome and immune disorders · Dermatological and COVID-19 studies
Acute rheumatic fever (ARF) and its chronic consequence rheumatic heart disease (RHD) are important causes of cardiovascular death and disability across much of the world [1]. Control of these diseases is complicated by the uncertain performance of the Jones' Criteria [2] in low resource settings, exacerbated by an absence of specific diagnostic tests for ARF. Prothymosin alpha (PTA) was recently proposed as a key contributor to RHD immunopathogenesis, as well as a putative biomarker discriminating patients with chronic RHD from healthy controls [3]. Therefore we sought to assess whether blood PTA was elevated in patients with ARF or RHD compared to unwell controls, indicating potential as a diagnostic. We compared this to immunoglobulin G3 (IgG3), which was recently shown to be elevated in ARF, as an additional putative biomarker [4].
Our study was approved by institutional review boards at the Children's Hospital Lahore [25th October 2018; Reference 2018/17], Lahore, Pakistan, and Makerere University, Kampala [17th March 2017; Reference 2017-042], Uganda, and the Imperial College London Research Ethics Committee [12th October 2022; Reference 6360509], London, UK. We undertook a case-control study investigating genetic susceptibility to ARF and RHD at the Children's Hospital Lahore between August 2019 and March 2022, with an interruption in March 2020 due to COVID-19. Here we focus on serum samples from children and young adults recruited during that study aged 5–21 years attending hospital including inpatients and outpatients with ARF, RHD or non-ARF diagnoses obtained after September 2020.
From our Pakistan study, we selected 30 individuals with suspected ARF comprising all 16 in the cohort with C-reactive protein (CRP) greater than 1 mg/dL and an additional 14 with CRP below this threshold. For comparison, we selected all 12 control individuals with non-ARF diagnoses and CRP greater than 1 mg/dL, and 14 non-inflammatory control individuals with CRP less than 1 mg/dL matched where possible by age and sex to the inflammatory cases. Finally, we included all four available samples from children with RHD without concurrent ARF giving a total sample of 60 individuals.
We measured PTA in duplicate in undiluted sera using a sandwich ELISA kit according to the manufacturer's instructions (LSBio; Cat. F50952). Total IgG3 was measured in sera diluted up to 1:50,000 using a bead assay according to the manufacturer's instructions (Merck; Cat. HGAMMAG-301 K) [5]. Preceding streptococcal infections were defined based on an anti-streptolysin O titer of greater than 250 IU/mL measured by automated immunoassay (Abbott, USA). Neither group A streptococcal rapid antigen tests nor anti-DNase B titer measurement were available to the study. The mean rank of groups was compared using a Kruskal-Wallis test while specific groups were compared using the Wilcoxon rank-sum test and multivariable analyses were performed by logistic regression in R software (version 4.4). Sample size was determined by the number of samples available at the time of the study rather than a formal power calculation.
In the Pakistan study, the median age was 12 years and 37 of 60 were male (Table 1). All 30 suspected ARF cases had evidence of carditis, 22 had arthritis or polyarthralgia, and none had chorea. For analysis, we reclassified the 30 suspected ARF cases using the 2015 Jones' Criteria for moderate and high-risk populations [2], giving 15 definite cases (all recurrent) and 15 possible (11 recurrent) not completely fulfilling the diagnostic criteria. Four individuals with possible ARF had received corticosteroids before recruitment. A single individual was excluded due to an invalid IgG3 measurement but otherwise there were no missing data. Total IgG3 was significantly elevated in the definite ARF cases compared to both inflammatory (p = 0.006) and non-inflammatory controls (p = 0.015; Fig. 1a); however, PTA concentrations were similar across all five groups (p = 0.56; Fig. 1b), irrespective of the presence or absence of an inflammatory state.Table 1. Characteristics of the Pakistan cohort.Table 1. Non-inflammatory control (n = 9)Inflammatory control (n = 17)Possible ARF (n = 15)Definite ARF (n = 15)Chronic RHD (n = 4)Age (years), median (IQR)13 (11–17)10 (9–14)12 (10−13)12 (10–14.5)10.5 (10−11)Female, n (%)4 (44)8 (47)6 (40)3 (20)2 (50)Carditis, n (%)0015 (100)15 (100)aJoint involvement, n (%)bb9 (60)13 (87)0CRP (mg/L), median (IQR)3 (0–7)30 (3–47)3 (1−13)20 (10–42)0 (0–1)ASO titer, median (IQR)152 (104–199)127 (67–215)150 (53–214)477 (311–601)80 (61–119)aChronic RHD without acute carditis.bDetails of joint symptoms not recorded.Fig. 1. Elevation of IgG3 but not PTA in ARF. Distribution across study groups of: (a) IgG3 in serum samples from Pakistan; (b) PTA in serum samples from Pakistan; (c) IgG3 in plasma samples from Uganda; (d) PTA in plasma samples from Uganda. Multivariable logistic regression model based on both cohorts comparing definite ARF (n = 25) to the inflammatory and non-inflammatory controls group combined (n = 36). Odds ratios and 95 % confidence intervals are shown for each one unit increase in: (e) normalized IgG3; (f) normalized PTA. Normalization was performed using a Yeo-Johnson Transformation and models are adjustment was made for age in years, male sex, CRP greater than 1 mg/dL and the cohort.OOR, beyond upper limit of detection.Fig. 1
The previous study detected PTA in plasma rather than serum [3]. Accordingly, to confirm the lack of elevation of PTA in the Pakistan cohort was not due our use of sera, we obtained plasma samples from a previously reported prospective epidemiological study of ARF in two regions of Uganda. That study ran between January 2018 and February 2020, recruiting children aged 3–17 years with suspected ARF [6]. For our analysis, we measured PTA in duplicate in plasma diluted 1:4 and IgG3 in serum diluted 1:50,000 as described above. Across the Ugandan cohort, the median age was eight years and half were male (Table 2). We included nine individuals with definite ARF (eight with CRP greater than 1 mg/dL), 10 inflammatory controls with non-ARF diagnoses (all CRP greater than 1 mg/dL), and seven individuals with chronic RHD. Six of the definite ARF cases had carditis while the remaining three had arthritis or polyarthralgia.Table 2. Characteristics of the Uganda cohort.Table 2. Inflammatory control (n = 10)Definite ARF (n = 9)Chronic RHD (n = 7)Age (years), median (IQR)7 (5–10)7 (6–10)10 (7.5–13)Female, n (%)6 (60)5 (56)2 (29)Carditis, n (%)06 (33)aJoint involvement, n (%)9 (90)7 (78)1 (14)CRP (mg/L), median (IQR)44 (29–46)53 (37–85)2 (2–15)ASO titer, median (IQR)115 (81–203)369 (221–676)188 (145–315)aChronic RHD without acute carditis.
Overall plasma PTA concentrations in the samples from Uganda (median 0.3 ng/mL, IQR 0.18–0.49) were higher than in the serum samples from Pakistan (median 0.17 ng/mL, IQR 0.1–0.22); however, plasma PTA concentrations were similar across groups within the Ugandan study (p = 0.24; Fig. 1c), as well as in a combined analysis of the two cohorts (p = 0.52). While there was no significant difference in median serum IgG3 across groups within the Ugandan study (p = 0.59; Fig. 1d), the median IgG3 serum concentration was significantly higher among definite ARF cases compared to all controls in a combined analysis (1.63 mg/mL vs 1.07 mg/mL, p = 0.001). Additionally, the relationship between ARF and IgG3 was robust to adjustment for age, sex, cohort and inflammatory status (p = 0.004; Fig. 1e), while no such relationship was apparent for PTA (p = 0.94; Fig. 1f).
In summary, we found blood PTA levels to be similar across ARF, RHD and controls, conflicting with a previous report that found PTA was elevated in RHD compared to healthy controls [3]. In contrast, total IgG3 was elevated in ARF compared to controls, independent of the acute phase response. To our knowledge, this is the first time elevation of IgG3 in ARF has been described outside of New Zealand, although the difference we observed here was less marked than that reported in previous studies [4,5] We acknowledge that limited diagnostic information were available for the controls and recognise that further work will be needed to characterise levels of IgG3 and PTA in other specific diagnoses. It is notable that the samples from Pakistan were obtained during the COVID-19 pandemic although we do not expect this to have altered our results. While our relatively small sample size was a limitation, it is noteworthy that we had more than twice the sample size available to us in comparison to the previous study [3]. Moreover, the proximity of the median values for PTA in the different diagnostic categories across both cohorts is important, given the large difference observed previously. Further, our study benefited from samples from two distinct ARF studies, inclusion of a spectrum of ARF in addition to RHD, a comparison with unwell controls, and use of both serum and plasma.
It remains unclear why our findings relating to PTA differ from those in the previous report [3]. However, importantly, we used an updated version of the ELISA kit produced by the same manufacturer, designed to detect PTA at 10-fold lower concentrations than that used in the previous study. Although we have not compared the performance of the two products, it is notable that the version that we used was based on mouse monoclonal rather than rabbit polyclonal capture antibodies. Nonetheless, we only had sera available from Pakistan, while our analyses based on plasma were limited to the smaller Ugandan cohort. Accordingly, it is possible we had insufficient power to detect a difference that was specific to plasma, although it is significant that patients with both definite ARF and chronic RHD from Uganda had lower median concentration of PTA than controls, rendering it unlikely that PTA could form the basis of a diagnostic test.
A total of 19 of 24 (79 %) children with definite ARF from Pakistan and Uganda had IgG3 above the previously highlighted threshold of 1 mg/mL. While this is lower than the proportion reported in the study from New Zealand [4], there are differences in the clinical characteristics of the cohorts recruited in Uganda, Pakistan and New Zealand, which may explain this discrepancy. Importantly, we used the definition of definite ARF for moderate and high-risk populations from the latest Jones Criteria revision, which included adjustments intended to improve sensitivity [2]. The impact of these criteria was especially apparent in Uganda since four of the nine children in the definite ARF category had polyarthralgia as a standalone major manifestation. It is notable that a higher proportion of children who met the stricter criteria for ARF intended for low-risk populations – 16 of 19 (84 %) – had IgG3 above the 1 mg/mL threshold, approaching the proportion reported from New Zealand [4]. Although IgG3 is not sufficiently elevated in our analysis to serve as a standalone biomarker, the consistency of our findings from two distinct cohorts with the previous studies from New Zealand is striking, and suggests further work is justified to understand the relationship between the disease and this subclass of antibody.
Accordingly, there is a clear need for ongoing work to identify biomarkers for ARF including measurement of IgG3 and other biomarker candidates in additional cohorts. Furthermore, careful interrogation of large-scale multi-omics datasets using techniques such as machine learning is likely to provide additional candidates suitable for independent validation [7]. We are now following both strategies through the Acute Rheumatic Fever Diagnostic Network (arcdiagnosticnetwork.org).
CRediT authorship contribution statement
Gul Afshan: Writing – review & editing, Resources, Project administration, Investigation. Nicole Tsui: Writing – review & editing, Investigation. Humera Javed: Writing – review & editing, Resources, Investigation. Tehmina Kazmi: Writing – review & editing, Resources, Investigation. Emma Ndagire: Writing – review & editing, Resources, Project administration, Investigation. Jafes Pulle: Writing – review & editing, Project administration, Investigation. Kristin Huse: Writing – review & editing, Investigation. Amelia Lias: Writing – review & editing, Investigation. Shagorika Talukder: Writing – review & editing, Investigation. Natalie Lorenz: Writing – review & editing, Investigation. Reuben McGregor: Writing – review & editing, Conceptualization. Craig Sable: Writing – review & editing, Funding acquisition, Conceptualization. Andrea Z. Beaton: Writing – review & editing, Funding acquisition, Conceptualization. Nicole J. Moreland: Writing – review & editing, Funding acquisition. Emmy Okello: Writing – review & editing, Funding acquisition, Conceptualization. Masood Sadiq: Writing – review & editing, Supervision, Project administration, Methodology, Funding acquisition, Conceptualization. Tom Parks: Writing – original draft, Supervision, Project administration, Methodology, Funding acquisition, Formal analysis, Conceptualization.
Ethical statement
Our study was approved by institutional review boards at the Children's Hospital Lahore [25th October 2018; Reference 2018/17], Lahore, Pakistan, and Makerere University, Kampala [17th March 2017; Reference 2017-042], Uganda, and the Imperial College London Research Ethics Committee [12th October 2022; Reference 6360509], London, UK.
Note
This research was funded in part by the 10.13039/100010269Wellcome Trust [222098/Z/20/Z]. For the purpose of open access, the author has applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this submission.
Funding
The study was supported by the BMA Foundation Josephine Lansdell Grant, the 10.13039/100000968American Heart Association Strategically Focused Research Network Grant, and the 10.13039/501100001674Leducq Foundation Acute Rheumatic Fever Biomarker Project. We also acknowledge funding from the 10.13039/100010269Wellcome Trust [222098/Z/20/Z (TP) and 215539/Z/19/Z (KH)] and 10.13039/501100000265Medical Research Council [MR/W00710X/1 (AL)]. These funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Karthikeyan G.Ntsekhe M.Islam S.Rangarajan S.Avezum A.Benz A.Mortality and morbidity in adults with rheumatic heart disease JAMA 3322202410.1001/jama.2024.8258 PMC 1115437438837131 · doi ↗ · pubmed ↗
- 2Gewitz M.H.Baltimore R.S.Tani L.Y.Sable C.A.Shulman S.T.Carapetis J.R.Revision of the Jones criteria for the diagnosis of acute rheumatic fever in the era of Doppler echocardiography a scientific statement from the American Heart Association Circulation 131202015180618182590877110.1161/CIR.0000000000000205 · doi ↗ · pubmed ↗
- 3Passos L.S.A.Jha P.K.Becker-Greene D.Blaser M.C.Romero D.Lupieri A.Prothymosin alpha: a novel contributor to estradiol receptor alpha–mediated CD 8 + T-cell pathogenic responses and recognition of type 1 collagen in rheumatic heart valve disease Circulation 145720225315483515751910.1161/CIRCULATIONAHA.121.057301 PMC 8869797 · doi ↗ · pubmed ↗
- 4Lorenz N.Mc Gregor R.Whitcombe A.L.Sharma P.Ramiah C.Middleton F.An acute rheumatic fever immune signature comprising inflammatory markers, Ig G 3, and Streptococcus pyogenes-specific antibodiesi Science 278202411055810.1016/j.isci.2024.110558 PMC 1134228639184444 · doi ↗ · pubmed ↗
- 5Chung A.W.Ho T.K.Hanson-Manful P.Tritscheller S.Raynes J.M.Whitcombe A.L.Systems immunology reveals a linked Ig G 3–C 4 response in patients with acute rheumatic fever Immunol. Cell Biol.981202012213174278110.1111/imcb.12298 · doi ↗ · pubmed ↗
- 6Okello E.Ndagire E.Muhamed B.Sarnacki R.Murali M.Pulle J.Incidence of acute rheumatic fever in northern and western Uganda: a prospective, population-based study Lancet Glob. Health 9102021 e 1423 e 14303441923710.1016/S 2214-109X(21)00288-6PMC 11144057 · doi ↗ · pubmed ↗
- 7Ralph A.P.Webb R.Moreland N.J.Mc Gregor R.Bosco A.Broadhurst D.Searching for a technology-driven acute rheumatic fever test: the START study protocol BMJ Open 1192021 e 05372010.1136/bmjopen-2021-053720 PMC 844425834526345 · doi ↗ · pubmed ↗