Association between endometrial cancer and subsequent risk of fracture: a national cohort study
Wen-Hsuan Tsai, Min-Shu Hsu, Chia-Sui Weng, Hsin-Yin Hsu, Cheng-Tzu Hsieh, Tzu-Lin Yeh, Kuo-Liong Chien, Chun-Chuan Lee, Ming-Nan Chien, Ming-Chieh Tsai

TL;DR
This study finds that endometrial cancer patients with diabetes have a higher risk of fractures compared to those without diabetes.
Contribution
The study identifies a significant increase in fracture risk among endometrial cancer patients with diabetes mellitus.
Findings
Endometrial cancer patients with diabetes had a higher risk of osteoporotic, hip, and vertebral fractures.
Diabetes mellitus was associated with increased hazard ratios for specific fracture types in endometrial cancer patients.
No significant fracture risk was observed in endometrial cancer patients without diabetes compared to the general population.
Abstract
Most endometrial cancer (EC) cases are estrogen-dependent, and some are associated with diabetes mellitus (DM). We aimed to estimate the risk of fracture among patients with EC and those with DM. A total of 20814 patients with EC were identified from the Taiwan National Cancer Registry from 2007 to 2018, with the outcome ascertainment using the National Health Insurance Research Database from 2004 to 2019. This observational study investigated the hazard ratios (HRs) for fracture and mortality events using Cox proportional hazards regression, with 95% confidence intervals (CIs). We adjusted baseline comorbidities, cancer therapy, cancer staging and grade, and pathological status of estrogen receptor and progesterone receptor. Considering the competing death events, we estimated the subdistribution hazard model to predict the probability of the fracture risk in the competing risks…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
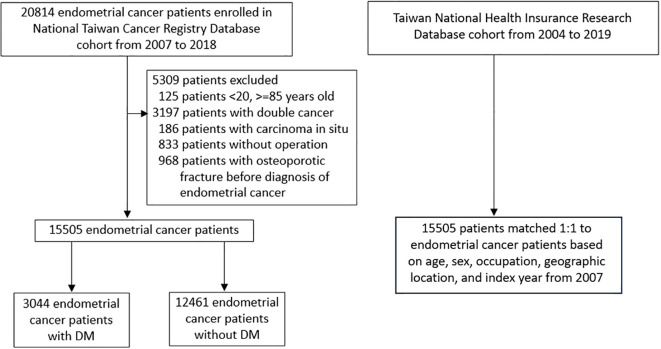 Figure 1
Figure 1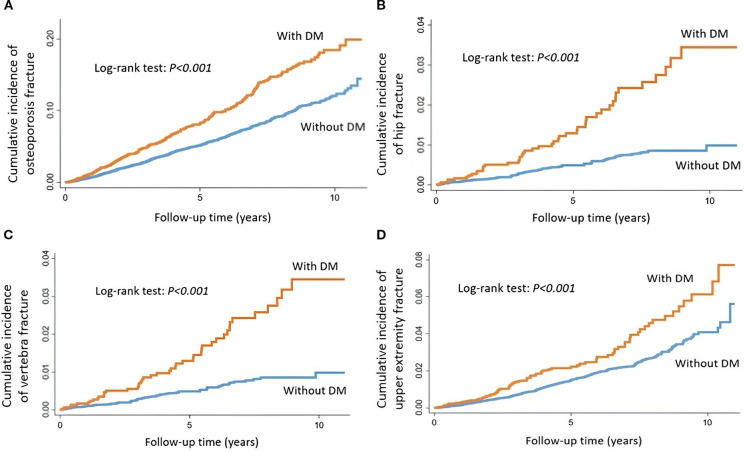 Figure 2
Figure 2| Hip fracture | Vertebral fracture | Upper extremity fracture | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Outcome variables | Without endometrial cancer | With endometrial cancer | Outcome variables | Without endometrial cancer | With endometrial cancer | Outcome variables | Without endometrial cancer | With endometrial cancer | ||||||
|
| 15497 | 15497 |
| 15497 | 15497 |
| 15497 | 15497 | ||||||
|
| 117 | 105 |
| 140 | 121 |
| 267 | 275 | ||||||
|
| 82826.3 | 75019.53 |
| 82826.31 | 74976.61 |
| 82425.95 | 74478.18 | ||||||
|
| 1.4 | 1.4 |
| 1.7 | 1.6 |
| 3.2 | 3.7 | ||||||
|
|
|
|
|
|
|
|
|
| ||||||
|
| 1 | 0.90 | 0.69 | 1.17 |
| 1 | 0.87 | 0.68 | 1.11 |
| 1 | 1.04 | 0.88 | 1.23 |
|
| 1 | 0.90 | 0.69 | 1.17 |
| 1 | 0.87 | 0.68 | 1.11 |
| 1 | 1.04 | 0.88 | 1.23 |
|
| 1 | 0.91 | 0.70 | 1.18 |
| 1 | 0.87 | 0.68 | 1.12 |
| 1 | 1.03 | 0.87 | 1.22 |
|
| 1 | 0.77 | 0.58 | 1.01 |
| 1 | 0.77 | 0.60 | 1.00 |
| 1 | 0.96 | 0.81 | 1.15 |
| Characteristics | Without DM | With DM | p-value | ||
|---|---|---|---|---|---|
| N=12461 | N=3044 | ||||
| n | % | n | % | ||
|
| <0.001 | ||||
| 20-39 | 1013 | 8.13 | 184 | 6.04 | |
| 40-59 | 8304 | 66.64 | 1550 | 50.92 | |
| ≧60 | 3144 | 25.23 | 1310 | 43.04 | |
| mean (SD) | 53.6 (9.91) | 57.5 (10.74) | |||
|
| <0.001 | ||||
| White collar | 1989 | 15.96 | 563 | 18.5 | |
| Blue collar | 6648 | 53.35 | 1366 | 44.88 | |
| Other | 3824 | 30.69 | 1115 | 36.63 | |
|
| 0.006 | ||||
| 1 | 3758 | 30.16 | 996 | 32.72 | |
| 2 | 8703 | 69.84 | 2048 | 67.28 | |
|
| <0.001 | ||||
| <30000 | 9776 | 78.45 | 2543 | 83.54 | |
| ≧30000 | 2685 | 21.55 | 501 | 16.46 | |
|
| |||||
| CVD | 482 | 3.87 | 465 | 15.28 | <0.001 |
| CKD | 2396 | 19.23 | 1915 | 62.91 | <0.001 |
| COPD | 2317 | 18.59 | 810 | 26.61 | <0.001 |
| Rheumatologic disease | 961 | 7.71 | 231 | 7.59 | 0.819 |
| PCOS | 370 | 2.97 | 100 | 3.29 | 0.362 |
|
| <0.001 | ||||
| No | 8728 | 70.04 | 2016 | 66.23 | |
| Yes | 3733 | 29.96 | 1028 | 33.77 | |
|
| 0.002 | ||||
| No | 9554 | 76.67 | 2251 | 73.95 | |
| Yes | 2907 | 23.33 | 793 | 26.05 | |
|
| 0.181 | ||||
| No | 12407 | 99.57 | 3036 | 99.74 | |
| Yes | 54 | 0.43 | 8 | 0.26 | |
|
| 0.843 | ||||
| No | 11618 | 93.23 | 2835 | 93.13 | |
| Yes | 843 | 6.77 | 209 | 6.87 | |
|
| 0.031 | ||||
| I | 9005 | 74.5 | 2173 | 72.48 | |
| II | 720 | 5.96 | 185 | 6.17 | |
| III | 1682 | 13.92 | 479 | 15.98 | |
| IV | 680 | 5.63 | 161 | 5.37 | |
|
| <0.001 | ||||
| 1 and 2 | 5346 | 62.75 | 1267 | 58.15 | |
| 3 | 3173 | 37.25 | 912 | 41.85 | |
|
| 0.184 | ||||
| negative | 3574 | 29.98 | 842 | 28.58 | |
| low | 2612 | 21.91 | 684 | 23.22 | |
| strong | 5736 | 48.11 | 1420 | 48.2 | |
|
| 0.094 | ||||
| negative | 4415 | 37.57 | 1028 | 35.4 | |
| low | 2810 | 23.91 | 721 | 24.83 | |
| strong | 4525 | 38.51 | 1155 | 39.77 | |
|
| <0.001 | ||||
| No | 11788 | 94.6 | 2779 | 91.29 | |
| Yes | 673 | 5.4 | 265 | 8.71 | |
|
| <0.001 | ||||
| No | 12402 | 99.53 | 2998 | 98.49 | |
| Yes | 59 | 0.47 | 46 | 1.51 | |
|
| <0.001 | ||||
| No | 12387 | 99.41 | 2997 | 98.46 | |
| Yes | 74 | 0.59 | 47 | 1.54 | |
|
| <0.001 | ||||
| No | 12260 | 98.41 | 2967 | 97.47 | |
| Yes | 198 | 1.59 | 77 | 2.53 | |
| Osteoporotic fracture | Hip fracture | Vertebral fracture | Upper extremity fracture | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Outcome variables | Without DM | With DM | Outcome variables | Without DM | With DM | Outcome variables | Without DM | With DM | Outcome variables | Without DM | With DM | ||||||||
|
| 12461 | 3044 |
| 12461 | 3044 |
| 12461 | 3044 |
| 12461 | 3044 | ||||||||
|
| 673 | 265 |
| 59 | 46 |
| 74 | 47 |
| 198 | 77 | ||||||||
|
| 58641 | 14061.92 |
| 60391 | 14645.62 |
| 60352 | 14641.71 |
| 59968 | 14527.16 | ||||||||
|
| 11.5 | 18.8 |
| 1 | 3.1 |
| 1.2 | 3.2 |
| 3.3 | 5.3 | ||||||||
| HR | HR | 95% CI | HR | HR | 95% CI | HR | HR | 95% CI | HR | HR | 95% CI | ||||||||
|
| 1 | 1.64 | 1.4 | 1.92 |
| 1 | 3.51 | 2.27 | 5.43 |
| 1 | 2.81 | 1.87 | 4.24 |
| 1 | 1.48 | 1.1 | 1.99 |
|
| 1 | 1.41 | 1.2 | 1.65 |
| 1 | 2.8 | 1.8 | 4.37 |
| 1 | 2.27 | 1.5 | 3.44 |
| 1 | 1.37 | 1.02 | 1.85 |
|
| 1 | 1.39 | 1.18 | 1.64 |
| 1 | 2.78 | 1.78 | 4.33 |
| 1 | 2.19 | 1.44 | 3.32 |
| 1 | 1.36 | 1.01 | 1.83 |
|
| 1 | 1.29 | 1.07 | 1.54 |
| 1 | 2.4 | 1.45 | 3.96 |
| 1 | 1.68 | 1.05 | 2.7 |
| 1 | 1.33 | 0.94 | 1.86 |
|
| 1 | 1.29 | 1.08 | 1.55 |
| 1 | 2.37 | 1.44 | 3.92 |
| 1 | 1.71 | 1.06 | 2.74 |
| 1 | 1.33 | 0.95 | 1.87 |
| Characteritics | Hip fracture | Characteritics | Vertebral fracture | Characteritics | Upper extremity fracture | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| With DM | With DM | With DM | ||||||||||||
| HR | 95% CI |
| HR | 95% CI |
| HR | 95% CI |
| ||||||
|
| 0.011 |
| 0.337 |
| 0.724 | |||||||||
| <60 | 2.34 | 1.08 | 5.04 | 0.03 | 1.74 | 0.84 | 3.58 | 0.134 | 1.33 | 0.87 | 2.03 | 0.184 | ||
| ≧60 | 2.49 | 1.27 | 4.87 | 0.01 | 1.68 | 0.9 | 3.14 | 0.102 | 1.30 | 0.74 | 2.31 | 0.362 | ||
|
| 0.125 |
| 0.993 |
| 0.674 | |||||||||
| negative | 2.72 | 1.11 | 6.63 | 0.028 | negative | 1.76 | 0.7 | 4.42 | 0.233 | negative | 1.59 | 0.8 | 3.14 | 0.185 |
| positive | 2.26 | 1.22 | 4.19 | 0.01 | positive | 1.72 | 0.99 | 2.97 | 0.054 | positive | 1.23 | 0.83 | 1.82 | 0.302 |
|
| 0.31 |
| 0.932 |
| 0.903 | |||||||||
| negative | 2.44 | 1.03 | 5.79 | 0.043 | negative | 1.77 | 0.76 | 4.14 | 0.188 | negative | 1.48 | 0.79 | 2.75 | 0.221 |
| positive | 2.34 | 1.25 | 4.36 | 0.008 | positive | 1.69 | 0.96 | 2.98 | 0.068 | positive | 1.26 | 0.84 | 1.88 | 0.271 |
|
| 0.748 |
| 0.204 |
| 0.176 | |||||||||
| I and II | 2.49 | 1.44 | 4.3 | 0.001 | I and II | 1.61 | 0.95 | 2.74 | 0.078 | I and II | 1.44 | 1.01 | 2.06 | 0.045 |
| III and IV | 2.13 | 0.64 | 7.08 | 0.217 | III and IV | 2.89 | 1.03 | 8.14 | 0.044 | III and IV | 0.51 | 0.17 | 1.49 | 0.216 |
|
| 0.184 |
| 0.333 |
| 0.971 | |||||||||
| No | 3.13 | 1.7 | 5.74 | <0.001 | No | 1.49 | 0.8 | 2.77 | 0.21 | No | 1.48 | 0.97 | 2.25 | 0.07 |
| Yes | 1.3 | 0.53 | 3.19 | 0.564 | Yes | 2.02 | 0.96 | 4.24 | 0.064 | Yes | 1.07 | 0.61 | 1.9 | 0.811 |
|
| 0.578 |
| 0.771 |
| 0.1 | |||||||||
| No | 2.33 | 1.32 | 4.13 | 0.004 | No | 1.54 | 0.91 | 2.62 | 0.109 | No | 1.44 | 1 | 2.08 | 0.05 |
| Yes | 2.59 | 0.9 | 7.48 | 0.078 | Yes | 2.32 | 0.82 | 6.62 | 0.115 | Yes | 0.75 | 0.29 | 1.96 | 0.559 |
|
| 1 |
| 1 |
| 1 | |||||||||
| No | 2.38 | 1.44 | 3.93 | 0.001 | No | 1.7 | 1.06 | 2.73 | 0.027 | No | 1.32 | 0.94 | 1.86 | 0.108 |
| Yes | Yes | Yes | ||||||||||||
|
| 0.684 |
| 0.988 |
| 0.584 | |||||||||
| No | 2.41 | 1.44 | 4.01 | 0.001 | No | 1.97 | 1.21 | 3.2 | 0.006 | No | 1.33 | 0.93 | 1.89 | 0.115 |
| Yes | 3.01 | 0.18 | 51 | 0.445 | Yes | 0 | 0 | 0.997 | Yes | 1.2 | 0.34 | 4.25 | 0.782 | |
|
| 0.968 |
| 0.724 |
| 0.823 | |||||||||
| No | 2.38 | 1.39 | 4.1 | 0.002 | No | 1.62 | 0.97 | 2.72 | 0.067 | No | 1.34 | 0.92 | 1.94 | 0.126 |
| Yes | 2.77 | 0.66 | 11.57 | 0.163 | Yes | 2.527 | 0.68 | 9.36 | 0.165 | Yes | 1.45 | 0.58 | 3.64 | 0.426 |
|
| 0.202 |
| 0.623 |
| 0.659 | |||||||||
| No | 1.64 | 0.74 | 3.64 | 0.224 | No | 1.38 | 0.63 | 3.04 | 0.421 | No | 1.23 | 0.76 | 1.99 | 0.406 |
| Yes | 3.41 | 1.6 | 7.26 | 0.002 | Yes | 1.92 | 1.04 | 3.56 | 0.037 | Yes | 1.41 | 0.86 | 2.31 | 0.178 |
|
| 0.142 |
| 0.691 |
| 0.537 | |||||||||
| No | 3.11 | 1.7 | 5.7 | <0.001 | No | 1.58 | 0.87 | 2.86 | 0.136 | No | 1.48 | 0.97 | 2.26 | 0.067 |
| Yes | 1.28 | 0.52 | 3.14 | 0.592 | Yes | 1.94 | 0.88 | 4.26 | 0.098 | Yes | 1.15 | 0.66 | 2.02 | 0.623 |
|
| 0.137 |
| 0.72 |
| 0.071 | |||||||||
| No | 2.19 | 1.29 | 3.71 | 0.004 | No | 1.82 | 1.09 | 3.03 | 0.022 | No | 1.27 | 0.88 | 1.82 | 0.203 |
| Yes | 7.39 | 1.04 | 52.26 | 0.045 | Yes | 1.16 | 0.27 | 4.97 | 0.846 | Yes | 1.96 | 0.71 | 5.46 | 0.196 |
|
| 1 |
| 1 |
| 0.521 | |||||||||
| No | 2.38 | 1.44 | 3.93 | 0.001 | No | 1.7 | 1.06 | 2.73 | 0.027 | No | 1.29 | 0.91 | 1.82 | 0.149 |
| Yes | Yes | Yes | 4.26 | 0.13 | 144.94 | 0.42 | ||||||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometrial and Cervical Cancer Treatments · Pregnancy-related medical research · Pelvic and Acetabular Injuries
Introduction
With the recent rise in incidence, endometrial cancer (EC) has become the leading gynecological cancer in developed countries (1). According to the notable symptoms, most patients are diagnosed at an early stage, accounting for 70% of endometrial cancer (2). Despite the relatively favorable prognosis, with a 5-year overall survival of 77% (3, 4), 25% of patients die for recurrent endometrial cancer within 5 years since diagnosis (2). Since most patients with EC will be long-term survivors, whether these patients will have different comorbidities from those without EC is a question of particular interest.
Bone loss has been associated with various cancer therapies (5, 6). Previous research on the lumbar spine bone mineral density (BMD) in patients with gynecological cancer demonstrated a positive correlation with body mass index (BMI) (7), but a negative correlation with the age of patients (7). As most EC cases are estrogen-dependent, a rapid decrease in estrogen may cause abrupt changes in BMD. This has been proven by the negative correlation between EC and BMD (7). Diabetes mellitus (DM), as a common comorbidity of EC, is not only a poor prognostic factor for EC, but also a risk factor for the development of EC (8). The underlying mechanism includes obesity, insulin resistance and chronic inflammation, hyperinsulinemia, hyperglycemia and epithelial-mesenchymal transition (EMT) (8). Despite greater BMD among patients with DM than those without DM, the higher risk of fracture in patients with DM may be due to inappropriate distribution of bone mass, deterioration in bone microarchitecture owing to the reduction of bone strength and disturbed repairment and adaptation of bone mechanisms (9, 10). In addition, several studies have reported that older adults with DM have a higher risk of falls when compared to those without DM (11, 12), which may also increase risk of fracture in patients with DM.
Our aim is to evaluate the fracture risk among patients with EC comparing with the general population, and whether EC patients with DM may associate an increased fracture risk when compared with those without DM.
Methods and materials
Data source
The National Taiwan Cancer Registry Database (NTCRD) is a nationally representative cancer dataset based on a 97.8% representative sample of Taiwanese cancer patients, which was designed and administrated by Ministry of Health and Welfare in 1979. Based on the Taiwan National Health Insurance program, which has covered 99.6% of Taiwanese residents under the national healthcare policy since 1995, our study utilized the Taiwan National Health Insurance Research Database (NHIRD). A total of 20814 patients with EC were identified from the NTCRD from January 1, 2007 to December 31, 2018. The demographics ascertained from the NHIRD included participants’ basic characteristics, household economic status, occupation categories, and medical records, encompassing diagnoses, medication prescriptions, and procedures from outpatient clinics, inpatient departments, and emergency departments, covering the period from January 1, 2004, to December 31, 2019. All individuals in both the NTCRD and NHIRD were de-identified and did not require participant consent. This study complied with the Declaration of Helsinki and was reviewed by the Ethics Committee of Mackay Memorial Hospital (21MMHIS398e).
Study design
First, we identified 15,505 patients with EC (2007–2013 ICD-O-FT: T-182; 2013–2018 ICD-O-3: C54.0, C54.1, C54.3, C54.8, and C54.9) who were 20 years of age or older between 2007 and 2018 (Figure 1). We excluded patients with a history of cancer diagnosed before 2007, those with double cancer, and those with fractures before the index date. Because surveillance of osteoporosis is a self-pay examination in Taiwan, only a small proportion of population have received osteoporosis examination. Hence, the ICD coding of osteoporosis may underestimate the accurate proportion of osteoporosis. In addition, since osteoporosis medications are only reimbursed by health insurance with strict criteria, many patients have to use osteoporosis medication by self-pay, which could not be evaluated by NHIRD. Therefore, we only excluded patients with history of osteoporotic fractures. These patients were further stratified into two groups: 3,044 patients with and 12,461 patients without DM (ICD-10-CM codes: E08, E09, E10, E11, and E13; ICD-9-CM codes: 250). The date of the initial diagnosis of EC was designated as the index date. In our observational cohort, EC cases were matched 1:1 to control subjects based on age, sex, occupation, geographic location, and index year, starting from January 1, 2007, in accordance with the enrollment period in the NTCRD.
Flow chart.
Outcome variables
Both EC patients with or without DM were followed until the incident fracture was identified (osteoporotic fracture, hip fracture, vertebral fracture, upper extremities fracture), withdrawal from the insurance, or the end of 2019. The ICD codes of the fractures were listed in Supplementary Table S1. The patients who were newly diagnosed with a fracture at least three times at the outpatient clinic (13) or at least one time during admission (14) between 2007 and 2018 were considered the potential study population. The incidence of fracture was the sum of all events and was calculated per 1,000 person-years.
Variable definitions
Covariates that might be associated with the development of fracture were included in the analyses. These included age (categorized as 20-39, 40-59, >= 60), occupation (categorized as white collar, blue collar, and other), urbanization (municipality and non-municipality), average monthly income (categorized as <35000 NTD, >= 35000 NTD), baseline comorbidities, radiotherapy, chemotherapy, target therapy, hormone therapy, cancer staging, grade, and the pathological status of the estrogen receptor (ER) and progesterone receptor (PR). For sensitivity analysis, we further evaluated the risk for osteoporosis and osteoporotic fracture in patients with EC within the 2011–2018 cohort. This included BMI as a potential risk covariate. Comorbidities included coronary artery disease (15), stroke, heart failure, chronic kidney disease (CKD) (16), chronic obstructive pulmonary disease (COPD) (17), rheumatologic disease (18), polycystic ovary syndrome (PCOS) (19). The ICD codes of the comorbidities were listed in Supplementary Table S1. The medications of hormone therapy included clomifene, raloxifene, bazedoxifene, tamoxifen, gestrinone, progesterone, norethisterone, allylestrenol, medroxyprogesterone, medroxyprogesterone, gestrinone, progesterone, dienogest, hydroxyprogesterone, dydrogesterone, medrogestone, levonorgestrel, ethisterone, letrozole, exemestane, and anastrozole.
Statistical analysis
The prevalence of demographic characteristics and comorbidities was compared between populations with and without EC using t-tests for continuous variables and Chi-squared tests for categorical ones. Cox proportional hazards analysis was used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) for fracture and mortality events. Considering the competing death events, we estimated the sub-distribution hazard model to predict the probability of the fracture risk with adjusted multivariable in the competing risks context using Fine and Gray method. Multivariate analysis, including basic demographics, comorbidities, and cancer-related medical records, was performed to calculate adjusted hazard ratios (aHRs). In the fully adjusted model, we adjusted for age, occupation, income, urbanization and comorbidities.
The basic characteristics and prevalence of comorbidities were compared between EC patients with and without DM. The cumulative incidence of fractures was estimated using the Kaplan–Meier method, and the HRs and 95% CIs for fractures were calculated using Cox proportional hazards models during the follow-up period. Demographic variables, comorbidities, cancer characteristics and treatment were included in multivariable models to estimate the aHRs: Model 1 adjusted for age, Model 2 adjusted for Model 1 variable, occupation, income, and urbanization, Model 3 adjusted for Model 2 variables and comorbidities, and Model 4 adjusted for Model 3 variables, cancer characteristics, and treatment. We also used the Bonferroni test to adjust for multiple comparisons.
For sensitivity analysis, demographic variables (including BMI), comorbidities, cancer characteristics and treatment were included in multivariable models to estimate the aHRs: Model 1 adjusted for age, Model 2 adjusted for Model 1 variable, occupation, income, and urbanization, Model 3 adjusted for Model 2 variables, comorbidities and BMI, and Model 4 adjusted for Model 3 variables, cancer characteristics and treatment. Statistical analyses were conducted with SAS 9.4 and STATA version 14 (StataCorp), with significance defined as a two-tailed p-value of < 0.05.
Results
Fracture risk among patients with and without EC
We identified 15,505 patients with EC between 2007 and 2018 (Figure 1). The competing risk models showed that patients with EC had a no significant association of hip, vertebra, and upper extremity fractures (Table 1). When compared with the general population, patients with EC and DM (HR 0.56 [95% CI 0.37–0.85]) or aged older than 65 years (HR 0.61 [95% CI 0.41–0.9]) had a lower risk of hip fracture than the control group (Supplementary Table S2). When compared with the general population, the interaction effect on vertebral fracture risk differed within the subgroups of age, DM, and COPD (Supplementary Table S3). When compared with the general population, the interaction effect on upper extremity fracture risk differed within the subgroups of age and COPD (Supplementary Table S4).
Fracture risk among patients with EC with and without DM
Of the 15,505 patients with EC from 2007 to 2018, there were 3,044 patients with and 12,461 patients without DM. The mean age of patients with EC, but without DM was 53.6 years. On the other hand, the mean age of patients with EC and DM was 57.5 years (Table 2). Patients with EC and DM had a higher prevalence of CVD, CKD, and COPD. These patients also received more RT and chemotherapy than those without DM. Patients with stages 3, 4, and grade 3 had a higher proportion of DM. Patients with DM had more osteoporotic fracture events (8.71%) than those without DM (5.4%). The cumulative incidence of osteoporotic fracture (log-rank test: P < 0.001), hip fracture (log-rank test: P < 0.001), vertebral fracture (log-rank test: P < 0.001), and upper extremity fracture (log-rank test: P < 0.001) in patients with EC with and without DM were demonstrated in Figure 2. Patients with DM had a significantly higher risk of osteoporotic fracture (HR 1.29 [95% CI 1.08-1.55]) (Table 3), hip fracture (HR 2.37 [95% CI 1.44-3.92]), and vertebral fracture (HR 1.71 [95% CI 1.06-2.74]). Patients with DM had a no significant association of upper extremity fracture (HR 1.33 [95% CI 0.95-1.87]) after they were adjusted for comorbidities, cancer characteristics, and treatment. We used the Bonferroni test for adjustment for multiple comparisons, and the results were demonstrated in Supplementary Table S5. Factors associated with each kind of fracture in patients with EC and DM were demonstrated in Table 4. Only age was demonstrated to have a significant interaction effect on hip fracture. Comorbidities and cancer characteristics seemed to have no interaction effect on fractures.
Cumulative incidence of (A) osteoporotic fracture, (B) hip fracture, (C) vertebral fracture, and (D) upper extremity fracture in endometrial cancer patients with and without DM.
Sensitivity analysis
As for the 2011–2018 cohort, which added BMI as one of the covariates, baseline demographic factors and comorbidities of EC patients with and without DM were demonstrated in Supplementary Table S6. Most of the patients with DM had a BMI ≥25. Patients with EC and DM in the 2011–2018 cohort had a significantly higher incidence of osteoporosis fracture (log-rank test: P < 0.001) (Supplementary Figure S1). Patients with EC and DM in the 2011–2018 cohort had a significantly higher risk of osteoporotic fracture (HR 1.35 [95% CI 1.09–1.69]) (Supplementary Table S7).
Discussion
Our study showed that patients with EC had a no significant association of hip, vertebral, and upper extremity fractures when compared with the general population. In all patients with EC, those with DM had a significantly higher risk of osteoporotic fracture, hip fracture, and vertebral fracture than those without DM. Patients with DM had a no significant association of upper extremity fracture compared with those with EC but without DM.
The present study demonstrated that patients with EC had a no significant association of hip, vertebra and upper extremity fracture when compared to the general population, which was not consistent with another population-based study of 2111 patients with EC (20), which showed a reduced risk of hip fracture in EC patients. This study had fewer patients than the current study (20), and the patients were followed up starting at age 50 (20). The present study included all patients older than 20 years. The previous study also demonstrated that age was not a determinant of the risk of hip fracture (20). On the other hand, we found that patients with EC and DM or aged older than 65 years had a lower risk of hip fracture than patients without EC. Since DM and older age are both well-known risk factors for fractures (21), lower risk of hip fractures in patients with EC may be attributed to higher BMI in patients with EC in the present study (20). Again, when compared with the general population, the interaction effect on vertebral fracture risk differed within subgroups of age, DM, and COPD. The difference between the fracture risk of the hip and vertebra could be attributed to the early bone loss in the trabecular bone, but with increasing age, the bone loss is restricted to the cortical region (22). Vertebral fractures are more common in patients younger than 65 years, and hip fractures are more frequent in patients older than 65 years (22). Previous studies revealed that patients with DM were vulnerable to postural instability due to altered motion perception (11). In addition, severe hypoglycemia was associated with a greater prevalence of falls (23), which may also put patients with DM at risk of fractures. With respect to COPD, smoking (24), reduced physical activity (25), low body weight (26), sarcopenia (27), systemic inflammation (28), glucocorticoid (29), vitamin D deficiency (30), hypoxemia and hypercapnia (31, 32), and anemia (33) were all associated with a higher risk of fracture. When compared with the general population, the interaction effect on upper extremity fracture risk also differed within subgroups of age and COPD.
Our study indicated that when comparing EC patients with and without DM, only age was demonstrated to have a significant interaction effect on hip fracture. Comorbidities, cancer treatment and characteristics seemed to have no interaction effect on fractures. A previous study involving 40 patients with cervical cancer revealed that changes in BMD of the lumbar spine after pelvic RT were not significant (34). Nonetheless, another study with 557 patients with cervical cancer showed that those with higher age, lower body weight, and higher radiation dose may suffer from pelvic fracture (35). In addition, another study of 239 patients, of whom 73 patients were diagnosed with EC, found a significant decrease in BMD after pelvic RT (36). As observed in our study, since patients with DM were diagnosed with more advanced EC, they received more RT and chemotherapy. Those who did not receive adjuvant therapy may suffer more from other comorbidities that restrain them from receiving further treatment. The staging and grade of EC and the diagnosis of DM were not analyzed in previous studies (34–36). Our study showed that cancer staging and grade had no interaction effect on hip, vertebral, and upper extremity fractures. Previous research demonstrated that higher BMI, compared to lower individuals, had a protective effect against fracture incidence (20). In our sensitivity analysis, which added BMI as one of the covariates, patients with EC and DM still demonstrated a significantly higher risk of osteoporotic fracture than patients without DM.
The strength of this study lies in the fact that it uses the largest number of patients’ data to date. The study focused on the fracture risk of EC patients with or without DM. Longer follow-up periods strengthened our evidence compared to previous investigations. Additionally, we conducted subgroup analyses to account for potential confounders, further enhancing the robustness of our findings. There are several limitations acknowledged within the research. First, rather than a randomized control design, the present observational study lacked the sufficient causality between the fracture risk and EC patients with DM. However, the nationally population-based cohort study still demonstrated significant evidence. Second, we could not calculate the window of time in which the 3 outpatient fractures occurred, nor could we determine whether the patients had similar fracture sites or not. Third, hormone therapy in this study included bone-positive and bone-negative effect, which may misestimate the interaction effect of hormone therapy on fracture. Fourth, we only excluded patients with history of osteoporotic fractures because diagnosis of osteoporosis and use of osteoporosis medication may be underestimated by NHIRD. Fifth, there might be persistent unmeasured covariates, particularly concerning cancer characteristics with potential interactions, collinearity, or dependencies among variables related to cancer and its treatment (e.g., estrogen level, ER and PR status, staging, radiotherapy, chemotherapy, targeted therapy, and hormone therapy). Although the basic demographic characteristic and detailed cancer information, such as staging and treatment, were all adjusted in our full model, future studies can benefit from addressing these dependencies through more advanced statistical techniques or alternative study designs, such as calculating variance inflation factors (VIFs), examining correlation matrices, stratification on cancer staging or investigating interaction terms of hormone receptor status which may potential confound the fracture risk.
Conclusion
According to our study, patients with EC had a no significant association of fracture, while DM increased the fracture risk in patients with EC. Age had a significant interaction effect on fracture. Since there were several limitations in the present study, such as lacking more detailed treatment and cancer staging classification, the results should be interpreted cautiously and more comprehensive studies are still required.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Morice P Leary A Creutzberg C Abu-Rustum N Darai E. Endometrial cancer. Lancet (London England). (2016) 387:1094–108. doi: 10.1016/S 0140-6736(15)00130-0, PMID: 26354523 · doi ↗ · pubmed ↗
- 2Colombo N Creutzberg C Amant F Bosse T González-Martín A Ledermann J. ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer: diagnosis, treatment and follow-up. Ann Oncol Off J Eur Soc Med Oncol. (2016) 27:16–41. doi: 10.1093/annonc/mdv 484, PMID: 26634381 · doi ↗ · pubmed ↗
- 3Talhouk A Mc Conechy MK Leung S Yang W Lum A Senz J. Confirmation of Pro Mis E: A simple, genomics-based clinical classifier for endometrial cancer. Cancer. (2017) 123:802–13. doi: 10.1002/cncr.30496, PMID: 28061006 · doi ↗ · pubmed ↗
- 4Mandato VD Mastrofilippo V Palicelli A Silvotti M Serra S Giaccherini L. Solitary vulvar metastasis from early-stage endometrial cancer: Case report and literature review. Medicine. (2021) 100:e 25863. doi: 10.1097/MD.0000000000025863, PMID: 34087828 PMC 8183741 · doi ↗ · pubmed ↗
- 5Pfeilschifter J Diel IJ. Osteoporosis due to cancer treatment: pathogenesis and management. J Clin Oncol Off J Am Soc Clin Oncol. (2000) 18:1570–93. doi: 10.1200/JCO.2000.18.7.1570, PMID: 10735906 · doi ↗ · pubmed ↗
- 6Guise TA. Bone loss and fracture risk associated with cancer therapy. Oncol. (2006) 11:1121–31. doi: 10.1634/theoncologist.11-10-1121, PMID: 17110632 · doi ↗ · pubmed ↗
- 7Lee JE Park CY Lee E Ji YI. Effect of gynecological cancer and its treatment on bone mineral density and the risk of osteoporosis and osteoporotic fracture. Obstetr Gynecol Sci. (2020) 63:470–9. doi: 10.5468/ogs.20012, PMID: 32689773 PMC 7393757 · doi ↗ · pubmed ↗
- 8Han J Zhang L Guo H Wysham WZ Roque DR Willson AK. Glucose promotes cell proliferation, glucose uptake and invasion in endometrial cancer cells via AMPK/m TOR/S 6 and MAPK signaling. Gynecol Oncol. (2015) 138:668–75. doi: 10.1016/j.ygyno.2015.06.036, PMID: 26135947 PMC 4672629 · doi ↗ · pubmed ↗