Disseminated cryptococcosis in an HIV patient with hepatitis C as the associated risk factor
Pallavi Dhawan, Varsha Gupta, Monica Gupta, Parakriti Gupta, Nidhi Singla

TL;DR
This paper reports a case of severe fungal infection in an HIV patient with hepatitis C, highlighting the complex medical challenges involved.
Contribution
The study presents a rare case linking hepatitis C with increased susceptibility to disseminated cryptococcosis in an HIV patient.
Findings
Cryptococcus neoformans was detected in both blood and cerebrospinal fluid samples.
Hepatitis C may contribute to neuroinflammation and blood-brain barrier disruption, increasing infection risk.
Comorbidities like HIV and hepatitis C complicate the diagnosis and treatment of opportunistic infections.
Abstract
In the context of HIV/AIDS, cryptococcosis emerges as one of the most common opportunistic infections, with a predilection for affecting individuals with compromised immune function. This study aimed to present a compelling case of disseminated cryptococcosis in a 29-year-old male with a complex medical history, marked by HIV infection, hepatitis C, and a longstanding history of intravenous drug abuse. Blood sample of the patient as well as the cerebrospinal fluid sample grew Cryptococcus neoformans. Immunochromatographic test performed on CSF and serum sample was also positive. Chronic Hepatitis C Virus can disrupt the blood-brain barrier and cause neuroinflammation predisposing the central nervous system to hematogenous seeding during fungemia. Multifaceted medical background of the patient underscored the challenges in the management of comorbidities.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
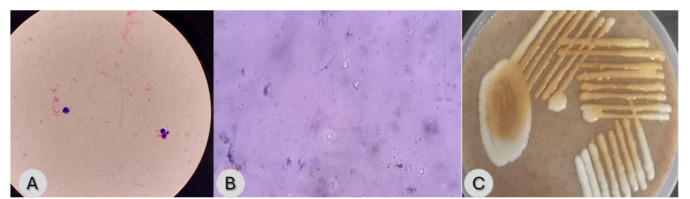 Figure 1
Figure 1| Name of parameter | On date 14.3.2024 | On date 23.3.2024 | On date 1.4.2024 (after 2 weeks of anti-fungal therapy) | Reference value |
|---|---|---|---|---|
| Haemoglobin | 7.2 | 6.2 | 8.8 | 12-18 g/dl |
| PCV | 23 | 20 | 27 | 36-54% |
| MCV | 84 | 82 | 89 | 80-96 fL |
| Platelets count | 17 | 43 | 65 | 150k-450 k/µL |
| Reticulocyte% | - | 2.6 | 4.55 | 0.2-2% |
| TLC | 12.04 | 8.2 | 6.58 | 4k-11 k/µL |
| DLC (N/L/E) | 59.3/15/11.5 | 79.4/16.6/4 | 71.8/17.8/8.1 | N- 40-75%, L- 20-45% |
| Sodium | 137 | 142 | 137 | 135-145 mEq/L |
| Potassium | 4.3 | 4.2 | 4.6 | 3.5-5.5 mEq/L |
| Chloride | 107 | 111 | 103 | 98-107 mEq/L |
| Urea | 99 | 136 | 108 | 15-45 mg/dL |
| Creatinine | 3.7 | 2.4 | 2 | 0.80-1.80 mg/dL |
| Bilirubin (Total/Conjugated) | 0.8/- | - | 0.4/- | Total-0.2-1.0 mg/dL, Conjugated-0-0.25mg/dL |
| ALP | 748 | 618 | 532 | 40-130 IU/L |
| AST | 103 | 25 | 57 | 5-40 IU/L |
| ALT | 42 | 20 | 42 | 5-40 IU/L |
| Total Protein | 7.6 | 6.7 | 5.2 | 6-8gm % |
| Albumin | 2.1 | 1.7 | 2.4 | 3.8-5.5 gm/dL |
| PT | 15 | - | - | 12-15 seconds |
| aPTT | 50 | - | - | 28-32 seconds |
| Amylase/lipase | 62/43 | - | - | 22-80 IU/L/13-60 IU/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies
Introduction
Cryptococcosis is a fungal infection caused by the genus Cryptococcus with two species commonly involved in human infections: Cryptococcus neoformans and Cryptococcus gattii. It poses a formidable challenge in infectious diseases, particularly among immunocompromised individuals. Spectrum of cryptococcal disease ranges from localized pulmonary involvement to disseminated infection, with the latter presenting a significant clinical concern due to its potential for severe morbidity and mortality [ 1 ]. Disseminated cryptococcosis occurs when the pathogen spreads beyond the lungs to involve various organs, including the central nervous system (CNS), leading to meningitis, making early recognition and intervention paramount in patient management. The interplay between Human Immunodeficiency Virus (HIV)-induced immunosuppression and the pathogenicity of Cryptococcus species underscores the importance of vigilance in the recognition and management of this potentially life-threatening condition [ 2 , 3 ].
Through a comprehensive examination of this case, this study aimed to elucidate the clinical features, diagnostic modalities, and therapeutic strategies employed in the management of disseminated cryptococcosis in a patient with co-infection of HIV and Hepatitis C Virus (HCV). This case highlighted the role of prompt diagnosis and tailored antifungal therapy in the achievement of favorable clinical outcomes. Additionally, it serves as a reminder to consider opportunistic infections in the differential diagnosis of immunocompromised patients and emphasizes the necessity of a multidisciplinary approach to patient care, integrating infectious disease expertise with specialized knowledge in HIV/Acquired Immunodeficiency Syndrome (AIDS) management and substance abuse rehabilitation.
Case Report
A 29-year-old male presented to the emergency department with complaints of abdominal pain predominantly in the right hypochondrium associated with loose stools (3-4 episodes/day). Additionally, he had a high-grade fever that persisted for two weeks. The patient had a history of intravenous drug abuse for three years and was known to have coexisting HIV and HCV infection. There were no reported symptoms of chest pain, cough, hemoptysis, nausea, vomiting, diarrhea, or neck swelling. He had experienced one episode of melena 15 days prior but did not seek medical attention.
Upon examination, the patient exhibited fever (100 °F) and severe pallor and was also malnourished with a body mass index of 19 kg/m^2^. There was evidence of terminal neck rigidity but no other significant abnormalities were observed on neurological examination. The patient remained lucid and responsive. He did not have oral thrush, oral/genital ulcers, or any significant lymphadenopathy. Fundus examination showed grade 2 papilledema and abdominal examination revealed mild hepatosplenomegaly.
The chest radiograph was non-contributory. Abdominal ultrasound revealed hepatosplenomegaly with a heterogenous pancreas. Although he had a history of infective endocarditis, the transthoracic echocardiography was normal. Weekly trends of hematological and biochemical parameters are shown in Table 1. Haemoglobin ranged from 5.9 to 7.2 g/dL initially, and there was thrombocytopenia for which he received four units of random donor platelets. Renal function tests were deranged with urea and creatinine peaking at 149 mg/dL and 4.0 mg/dL respectively. Elevated liver enzymes [alkaline phosphatase (ALP), aspartate aminotransferase (AST), and alanine aminotransferase (ALT)] were noted on more than two occasions attributed to HCV infection and acute liver injury due to systemic infection. There was no evidence of intrahepatic or extrahepatic obstruction. Low protein and albumin levels were consistent with the underlying conditions.
Blood culture samples were sent for routine culture and sensitivity. An automated blood culture system (Biomérieux BACT/ALERT® 3D) detected growth after overnight incubation. Direct Gram stain from the positive flagged bottle revealed gram-positive yeast cells (7-8 µm) with capsulated appearance. India ink preparation was also made which was positive for capsulated budding yeast cells suggestive of Cryptococcus sp. (Figure 1). Subculture on Sabouraud’s dextrose medium grew creamy pasty mucoid colonies (incubated aerobically at 37 ℃ overnight) which were confirmed to be Cryptococcus sp. on bird seed agar (HiMedia). On bird seed agar, Cryptococcus sp. produces brown pigmented colonies due to melanin under the action of phenol oxidase enzyme (Figure 1).
A: Gram-stained smear showing Gram-positive budding yeast cell with pink halo suggestive of a capsule. Figure 1B: India ink preparation showing budding yeast cells with capsule suggestive of Cryptococcus sp. Figure 1C: Brown-colored colonies on Bird Seed Agar.
Lumbar puncture was initially withheld due to thrombocytopenia but was performed after improvement. The cerebrospinal fluid (CSF) analysis confirmed Cryptococcus sp. and matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS, VITEK® MS PRIME, Biomerieux) identified the isolate as C. neoformans. Cryptococcal antigen lateral flow assay (CryptoPS, Biosynex, Strasbourg, France) on serum and CSF was also positive, supporting the diagnosis.
Treatment and outcome
The patient was administered liposomal amphotericin B (5 mg/kg per day) and fluconazole (800 mg daily) for 14 days. Renal and hepatic functions along with electrolytes were closely monitored. Renal function gradually improved and hepatic enzymes, particularly ALP, showed moderate improvement. The patient responded well during hospitalization with improvement of neurological symptoms. At discharge, he was advised to continue fluconazole (400 mg daily for another eight weeks) and follow up in the antiretroviral therapy (ART) clinic. He was started on highly active antiretroviral therapy (HAART) and HCV treatment, post-anti-fungal therapy and demonstrated clinical improvement.
Discussion
Cryptococcosis is a significant global health concern, particularly among HIV/AIDS patients, accounting for approximately 152,000 deaths in 2020 due to cryptococcal meningitis [ 4 ]. The burden is higher in low-resource regions, like sub-Saharan Africa and parts of Asia, including India, where gaps in ART coverage, delayed diagnosis, and limited access to antifungal medications contribute to higher mortality rates [ 4 , 5 ]. India reports an estimated 11,526 annual cases of cryptococcal meningitis, predominantly linked to advanced HIV disease [ 5 ]. High-resource settings, with robust ART programs and early screening, have lower prevalence rates, underscoring the need for global health equity to combat this preventable disease [ 4 , 5 ].
Cryptococcus neoformans employs strategies to evade the immune system, including a polysaccharide capsule and melanin production. The capsule inhibits phagocytosis, reduces antigen presentation, and suppresses inflammatory cytokines, blunting the immune response. Melanin neutralizes oxidative stress, diminishes cytokine reactivity, and reduces antifungal treatment efficacy, enhancing virulence [ 6 ].
This immune compromise is compounded in individuals with HIV/AIDS, where C. neoformans often thrives. The HIV-induced immunosuppression significantly increases the risk of opportunistic infections, with cryptococcosis being considered an AIDS-defining illness. The presented case aligns with existing studies demonstrating the heightened susceptibility to disseminated cryptococcosis in HIV-infected individuals, highlighting the importance of early recognition and treatment in this population [ 7 , 8 ].
Diagnosis of cryptococcosis in patients with HIV, HCV, and IV drug use is challenging due to overlapping clinical features with other opportunistic infections, such as tubercular or bacterial meningitis. Cryptococcal antigen testing, particularly lateral flow assay, offers good sensitivity and specificity facilitating early detection in serum and CSF. These tools provide evidence especially in resource-limited settings [ 9 ].
Coexistence of HCV infection and IV drug abuse complicates cryptococcosis management in HIV patients. Immunomodulatory effects of substance abuse coupled with HCV-induced hepatotoxicity, compromise immune function. Liver disease reduces T cell response, lymphocytic activity, and complement components, like C5b-9, lowering antimicrobial defense [ 10 ]. Chronic HCV can disrupt the blood-brain barrier and cause neuroinflammation predisposing the CNS to hematogenous seeding during fungemia [ 11 ]. El Serag et al. [ 12 ] found that patients with HCV infection had a significantly higher prevalence rate of Cryptococcal infection, compared to the controls (0.4% vs. 0.1%). Decompensated liver disease is also an important risk factor for the dissemination of cryptococcal infection. Baddley et al. [ 13 ] reported that cirrhosis (due to any cause, including HBV or HCV infection) leads to a 5.8-fold increase in the risk of extrapulmonary dissemination of cryptococcal infection. Liver disease patients develop collateral circulation which allows Cryptococcus sp. to bypass the liver scavenger system and lead to spill over into circulation and hence, dissemination [ 14 , 15 ]. The IV drug use alters immune responses, further heightening susceptibility to infections [ 10 , 16 , 17 ]. The HCV infection in IV drug users is present in 60-80% of cases [ 18 ]. The HIV and HCV co-infection is common, sharing transmission routes, like IV drug use.
Prompt initiation of liposomal amphotericin B therapy aligns with current recommendations for disseminated cryptococcosis. Three-phase treatment approach of WHO, consisting of induction therapy with liposomal amphotericin B, flucytosine, and fluconazole for rapid fungal clearance, followed by consolidation and maintenance with fluconazole is effective but challenging in low-resource settings due to financial and logistic barriers [ 19 , 20 ]. Patients with HIV and liver disease are particularly vulnerable, facing heightened risks of nephrotoxicity from amphotericin and hepatotoxicity from fluconazole. Similarly, IV drug users encounter unique adherence challenges and complications due to co-occurring infections and substance use disorders. Tailored treatment strategies and integrated care models are essential for overcoming these challenges, as demonstrated in this case.
Conclusion
This case emphasized the need for a multidisciplinary approach in the management of patients with complex medical histories, particularly those with IV drug use and multiple comorbidities. Early recognition and treatment of opportunistic infections, such as cryptococcosis, are essential in the improvement of patient outcomes and reduction of morbidity and mortality associated with these conditions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maziarz EK Perfect JR Cryptococcosis Infect Dis Clin North Am 2016 301792062689706710.1016/j.idc.2015.10.006PMC 5808417 · doi ↗ · pubmed ↗
- 2Madhavan A Sachu A Samuel A Vasudevapanicker J Cryptococcal antigen prevalence in HIV patients from a tertiary care centre in South India Iran J Microbiol 2022 147407453653181910.18502/ijm.v 14i 5.10970 PMC 9723432 · doi ↗ · pubmed ↗
- 3Okurut S Boulware DR Olobo J Meya DB Landmark clinical observations and immunopathogenesis pathways linked to HIV and Cryptococcus fatal central nervous system co‐infection Mycoses 2020 638408533247272710.1111/myc.13122 PMC 7416908 · doi ↗ · pubmed ↗
- 4Kabir Z Cunningham C The global burden of cryptococcosis—a neglected tropical disease? Lancet Infect Dis 2022 2212165816603604948710.1016/S 1473-3099(22)00516-3 · doi ↗ · pubmed ↗
- 5Ray A Aayilliath K A Banerjee S Chakrabarti A Denning DW Burden of s Serious fungal infections in India Open Forum Infect Dis 2022912 ofac 6033658948410.1093/ofid/ofac 603PMC 9792086 · doi ↗ · pubmed ↗
- 6Yang C Huang Y Zhou Y Zang X Deng H Liu Yetal Cryptococcus escapes host immunity: What do we know? Front Cell Infect Microbiol 20221210410363631087910.3389/fcimb.2022.1041036 PMC 9606624 · doi ↗ · pubmed ↗
- 7Bramantono B Danial A Hadi U A case of an AIDS patient with Cryptococcus neoformans infection Pan Afr Med J 2020 36883277464710.11604/pamj.2020.36.88.20406 PMC 7392875 · doi ↗ · pubmed ↗
- 8Longhitano A Woolley I Upjohn L Korman T New diagnosis of HIV with Cryptococcus neoformans infection presenting as a pleural syndrome AIDS 2022 36161116133597983510.1097/QAD.0000000000003303 · doi ↗ · pubmed ↗