Clinical Results of Bristow and Latarjet Procedures in Patients With Anterior Shoulder Instability: A Systematic Review and Meta-Analysis
Masaki Karasuyama, Junichi Kawakami, Shuhei Yamamoto, Takashi Ariie, Takashi Tsuruta, Tomohiko Minamikawa, Hiroki Ohzono, Hiroaki Moriyama, Masafumi Gotoh

TL;DR
This study compares two surgical procedures for shoulder instability and finds no significant difference in their effectiveness.
Contribution
A systematic review and meta-analysis comparing Bristow and Latarjet procedures for anterior shoulder instability.
Findings
No redislocation events occurred in either Bristow or Latarjet procedure patients.
No significant difference in instability symptoms or return to sports between the two procedures.
The Rowe score showed a statistically significant but clinically insignificant difference between the procedures.
Abstract
Anterior shoulder instability poses a significant challenge, particularly in active populations. The Bristow and Latarjet surgical approaches address this issue; however, their comparative efficacy remains debated. This study conducted a meta-analysis of randomized controlled trials and observational studies to assess the efficacy of the Bristow and Latarjet procedures in patients with anterior shoulder instability. We searched electronic databases, including CENTRAL, MEDLINE, and EMBASE, for both randomized controlled trials and observational studies from inception to May 2023. To ensure the inclusion of recent evidence, we conducted an updated search in March 2025 to identify studies published between May 2023 and March 2025. We included studies that recruited patients with anterior shoulder instability and compared the Bristow and Latarjet procedures. The primary outcomes included…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
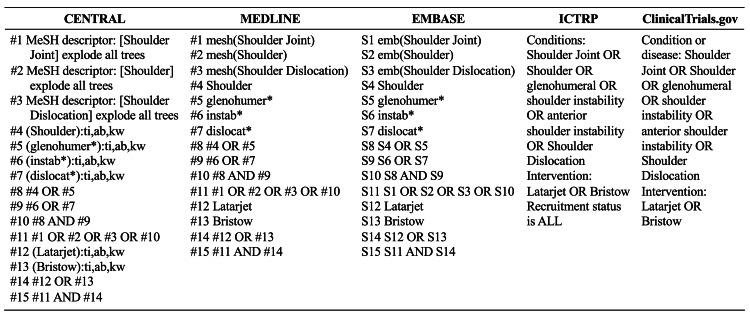 Figure 1
Figure 1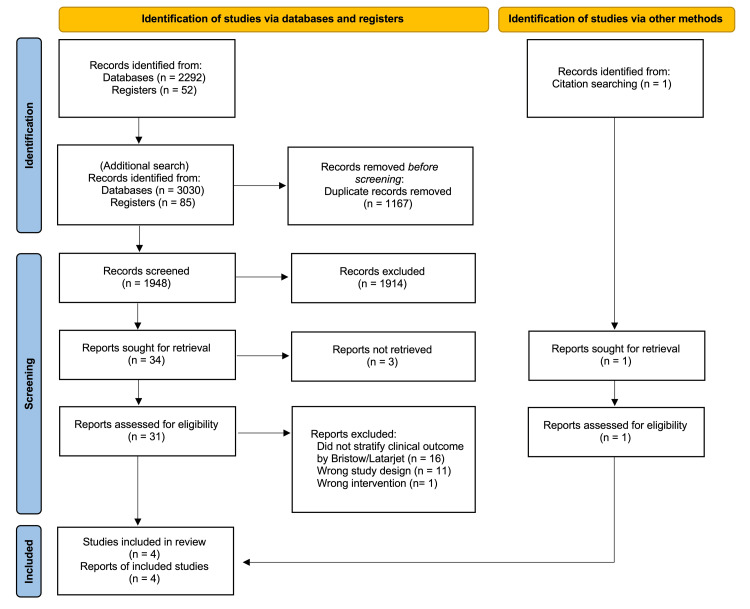 Figure 2
Figure 2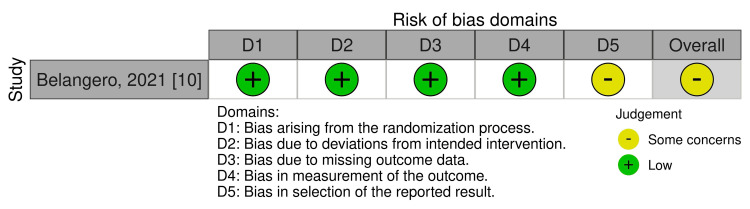 Figure 3
Figure 3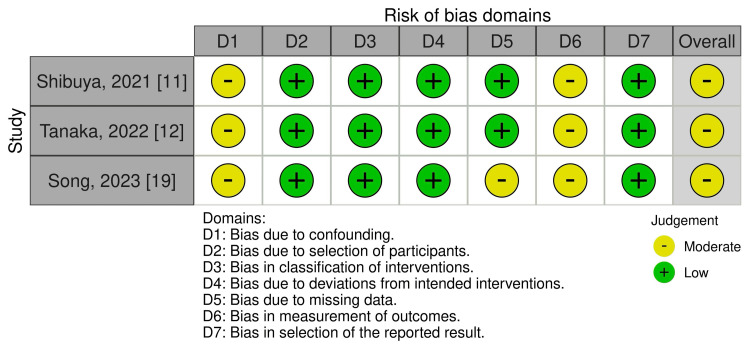 Figure 4
Figure 4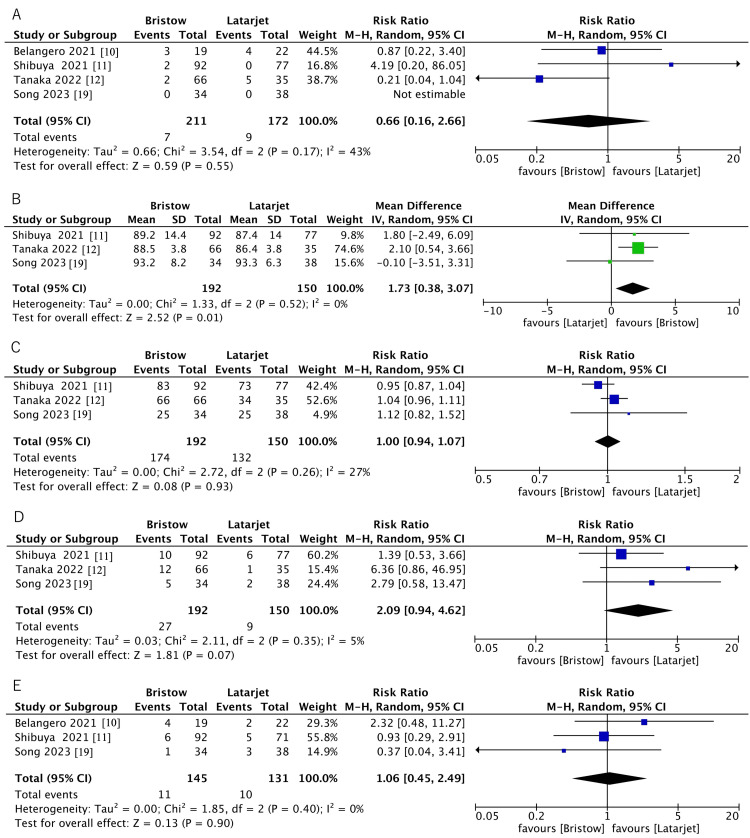 Figure 5
Figure 5| Section and topic | Item # | Checklist item | Location where item is reported |
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | Title Page |
| ABSTRACT | |||
| Abstract | 2 | See the PRISMA 2020 for Abstracts checklist. | Abstract |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | Introduction |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | Introduction |
| METHODS | |||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | Methods |
| Information sources | 6 | Specify all databases, registers, websites, organisations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | Methods |
| Search strategy | 7 | Present the full search strategies for all databases, registers and websites, including any filters and limits used. | Methods |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and if applicable, details of automation tools used in the process. | Methods |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and if applicable, details of automation tools used in the process. | Methods |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g. for all measures, time points, analyses), and if not, the methods used to decide which results to collect. | Methods |
| 10b | List and define all other variables for which data were sought (e.g. participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. | Not applicable | |
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process. | Methods |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g. risk ratio, mean difference) used in the synthesis or presentation of results. | Methods |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis (e.g. tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). | Methods |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics, or data conversions. | Methods | |
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | Methods | |
| 13d | Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used. | Methods | |
| 13e | Describe any methods used to explore possible causes of heterogeneity among study results (e.g. subgroup analysis, meta-regression). | Methods | |
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | Methods | |
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | Methods |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | Methods |
| RESULTS | |||
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | Results |
| 16b | Cite studies that might appear to meet the inclusion criteria, but which were excluded, and explain why they were excluded. | Results | |
| Study characteristics | 17 | Cite each included study and present its characteristics. | Results |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | Results |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g. confidence/credible interval), ideally using structured tables or plots. | Results |
| Results of syntheses | 20a | For each synthesis, briefly summarise the characteristics and risk of bias among contributing studies. | Results |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g. confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | Results | |
| 20c | Present results of all investigations of possible causes of heterogeneity among study results. | Results | |
| 20d | Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. | Results | |
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | Results |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | Results |
| DISCUSSION | |||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | Discussion |
| 23b | Discuss any limitations of the evidence included in the review. | Discussion | |
| 23c | Discuss any limitations of the review processes used. | Discussion | |
| 23d | Discuss implications of the results for practice, policy, and future research. | Discussion | |
| OTHER INFORMATION | |||
| Registration and protocol | 24a | Provide registration information for the review, including register name and registration number, or state that the review was not registered. | Methods |
| 24b | Indicate where the review protocol can be accessed, or state that a protocol was not prepared. | Methods | |
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | Methods | |
| Support | 25 | Describe sources of financial or non-financial support for the review, and the role of the funders or sponsors in the review. | Title page |
| Competing interests | 26 | Declare any competing interests of review authors. | Title page |
| Availability of data, code and other materials | 27 | Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; any other materials used in the review. | Not applicable |
| Author | Year | Study design | Coracoid bone block procedure | Sample size, shoulders | Mean age, yr | Sex (M:F) | Sample extraction | Follow-up |
| Belangero et al. [ | 2021 | Randomized controlled trial | Open Bristow | 19 | 26.4 | 37:4 | High-demand athletes | 60 months |
| Open Latarjet | 22 | |||||||
| Shibuya et al. [ | 2021 | Prospective cohort | Open Bristow | 92 | 18.3 (17.5-19.1) | 169:0 | Rugby players | 32.4 months |
| Open Latarjet | 77 | 19.1 (18.3-20.1) | ||||||
| Tanaka et al. [ | 2022 | Retrospective cohort | Open Bristow | 66 | 18.4 (15-26) | 101:0 | Rugby Players | 73.5 months |
| Open Latarjet | 35 | 17.7 (13-21) | 63.5 months | |||||
| Song et al. [ | 2023 | Retrospective cohort | Arthroscopic Bristow | 34 | 25.6 | 28:6 | Contact-sport athletes | 40.8 months |
| Arthroscopic Latarjet | 38 | 29.3 | 29:9 |
| Outcome | Participants (# studies) | Anticipated absolute effects (95% CI) | Risk with Bristow | CoE (GRADE) | |
| Risk with Latarjet | Risk with Bristow | ||||
| Redislocation | 383 (1 RCTs, 3 Cohort) | 0 per 1,000 | 0 per 1.000 (0 to 0) | Not estimable | ⨁⨁⨁◯ Moderateb |
| Instability symptoms | 383 (1 RCTs, 3 Cohort) | 52 per 1,000 | 35 per 1.000 (8 to 139) | RR 0.66 (0.16 to 2.66) | ⨁⨁◯◯ Lowa,b |
| Rowe score | 342 (3 Cohort) | - | MD 1.73 higher (0.38 higher to 3.07 higher) | - | ⨁⨁⨁◯ Moderateb |
| Return to sports | 342 (3 Cohort) | 880 per 1,000 | 880 per 1.000 (827 to 942) | RR 1.00 (0.94 to 1.07) | ⨁⨁◯◯ Lowa,b |
| Bone nonunion | 342 (3 Cohort) | 60 per 1,000 | 125 per 1.000 (56 to 277) | RR 2.09 (0.94 to 4.62) | ⨁⨁⨁◯ Moderateb |
| Bone resorption | Not pooled | Not pooled | Not pooled | Not pooled | - |
| Complications | 276 (1 RCTs, 2 Cohort) | 76 per 1,000 | 81 per 1.000 (34 to 190) | RR 1.06 (0.45 to 2.49) | ⨁⨁◯◯ Lowa,b |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Shoulder and Clavicle Injuries · Sports injuries and prevention
Introduction and background
Anterior shoulder instability (ASI) predominantly occurs in active populations, with approximately 95% of cases involving the anterior direction of instability [1]. ASI occurs due to disruption of the static and dynamic stabilization mechanisms of the glenohumeral joint, and in some instances, pain [2]. The incidence of ASI, as reported in studies targeting the general population of the United States, is approximately 0.08 individuals per 1000 persons per year [3]. Notably, in males under 30 years of age, a higher incidence of 1.69 individuals per 1000 persons per year is observed [4]. Athletes engaged in sports activities exhibit an incidence rate over twice as high as those participating in recreational activities, signifying an elevated risk of developing ASI within more active populations [5].
Arthroscopic Bankart repair is the most commonly performed surgical treatment for ASI; however, rugby and American football players exhibit elevated redislocation rates [6]. For patients with a heightened risk of redislocation, the Bristow-Latarjet procedure, involving the transfer of the coracoid process to the anterior rim of the glenoid, is employed. The Bristow procedure positions the excised coracoid process in an upright orientation directly below the glenoid, secured with a single screw [7]. In contrast, the Latarjet procedure places the coracoid process in a laid-down orientation after osteotomy at its base, fixing it with two screws to the anterior glenoid, which provides broader bony contact and a larger sling effect for stabilization [8]. Both procedures can be performed using open or arthroscopic approaches. In recent years, arthroscopic techniques have been increasingly adopted for both the Bristow and Latarjet procedures, with reported advantages in visualization and graft positioning.
In 2019, a systematic review was published encompassing 41 studies utilizing the Bristow procedure and 18 studies of the Latarjet procedure in patients with ASI [9]. While this review suggested that the Bristow procedure might lead to a reduced recurrence rate compared with the Latarjet procedure, it lacked randomized controlled trials (RCTs) and observational studies directly comparing these two surgical techniques, precluding the feasibility of conducting a meta-analysis.
In 2021, the first randomized controlled trial comparing the Bristow and Latarjet procedures for ASI was published [10]. Subsequently, several observational studies on these two techniques have been published, contributing to an increasing body of evidence regarding the efficacy of either method for treating ASI [11,12]. By aggregating and analyzing the contents of these studies, further insights could be gained concerning the comparison of postoperative outcomes between the Bristow and Latarjet procedures in patients with traumatic ASI. Therefore, the objective of this study was to elucidate the efficacy of the Bristow and Latarjet procedures in patients with ASI through a meta-analysis of RCTs and observational studies, with the primary research question being whether either technique results in superior clinical outcomes.
Review
Material and methods
This study was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) 2020 (Table 1) [13]. The protocol for this study was registered in the Open Science Framework (https://osf.io/vfwgu/).
Study Identification
We searched the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, and EMBASE electronic databases with no limitations concerning the year of publication or language. The initial search included studies from database inception to May 2023. Since approximately one year had passed since the initial search and to capture newly published data before finalizing the review, we conducted an updated search in March 2025, covering studies published between May 2023 and March 2025. Search strategies were adjusted to meet the specifications of the individual databases (Figure 1). In addition, we checked the reference lists of eligible studies and articles that cited the eligible studies. We searched the World Health Organization International Clinical Trials Platform Search Portal (ICTRP) and ClinicalTrials.gov databases to identify ongoing clinical trials. Two independent reviewers screened the titles and abstracts and assessed their eligibility based on the full text. Disagreements between the two reviewers were resolved through discussion, and if this failed, a third reviewer acted as an arbiter.
Search strategy indicates truncation (e.g., glenohumer* retrieves glenohumeral, glenohumerus, etc.)*
Eligibility Criteria
We included studies that recruited patients with ASI and compared the Bristow and Latarjet procedures. Although RCTs have the most rigorous design for assessing the efficacy of intervention studies, most of the available literature on this topic consists of non-RCTs or observational studies. Therefore, we included RCTs, quasi-randomized controlled trials, and observational studies (cohort, case-control, and cross-sectional studies). We did not apply language or country restrictions. We included all the papers, including published and unpublished articles, conference abstracts, and letters. Literature reviews, expert opinions, nonhuman or cadaver studies, case reports, and clinical studies that did not evaluate the Bristow and Latarjet procedures were excluded.
Assessment of Risk of Bias
Two reviewers independently evaluated the risk of bias using the Cochrane Collaboration's Risk of Bias 2 (RoB 2) tool for RCTs [14]. We summarized the risk of bias judgments for each outcome across the different studies for the five domains: (1) the randomization process, (2) deviations from intended interventions, (3) missing outcome data, (4) measurement of the outcome, and (5) selection of the reported result. We used the signaling questions in RoB 2 and rated each domain as having a low risk of bias, some concerns, or high risk of bias. The overall risk of bias for each outcome reflected the least favorable assessment across these domains. An outcome was judged to be at low risk of bias if all domains were rated as low risk. We assessed an outcome as having some concerns if at least one domain was rated as having some concerns and none were rated as high risk. An outcome was classified as high risk of bias if one or more domains were rated as high risk or if multiple domains were rated as having some concerns.
We evaluated the nonrandomized studies using the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool [15], which assesses seven domains: (1) confounding, (2) selection of participants, (3) classification of interventions, (4) deviations from intended interventions, (5) missing data, (6) measurement of outcomes, and (7) selection of reported results. Each domain and the overall risk of bias are judged as low, moderate, serious, or critical. Disagreements between the two reviewers were discussed; if this failed, a third reviewer acted as an arbiter, if necessary. Disagreements between the two reviewers were discussed; if this failed, a third reviewer acted as an arbiter, if necessary.
Types of Outcome Measures
The primary outcomes were redislocation rates, instability symptoms (including subluxations or positive symptoms of instability, such as an apprehension test), and the Rowe score [9]. The secondary outcomes included return to sports, bone nonunion, bone resorption, and operative complications [16].
Data Synthesis
We pooled the relative risk ratios (RRs) for binary outcomes and mean differences (MDs) for continuous outcomes. Where standard deviations (SD) were missing, which is a necessary component for statistical calculations in meta-analyses, we contacted the corresponding authors for details on the clinical results. If the author named in the report could not be contacted or did not respond, we calculated SDs from standard errors (SEs), 95% confidence intervals (CIs), or P values. For two studies, the SDs for the Rowe score were not available; therefore, we calculated them using a validated estimation formula [11,12]. Specifically, we derived the t statistic from the reported P value and sample sizes, calculated the SE of the MD, and then obtained the pooled within-group SD. The potential influence of using imputed data was examined through sensitivity analysis by excluding these studies from the pooled analysis.
We used the I2 statistic to measure the heterogeneity among the trials in each analysis. We interpreted the I2 statistic as follows: 0%-40% may represent insignificant heterogeneity, 30%-60% may represent moderate heterogeneity, 50%-90% may represent substantial heterogeneity, and 75%-100% may represent considerable heterogeneity.
Meta-analyses were conducted using the Cochrane Collaboration statistical software Review Manager 5.4 (The Cochrane Collaboration, London, England, UK). A random‐effects model was applied for all outcomes, as we anticipated clinical heterogeneity across studies due to differences in sample size, participant characteristics, and surgical procedures. Continuous data are expressed as mean differences and 95% CIs. For dichotomous outcomes, risk ratios (RRs) were calculated with 95% CIs. An effect was considered significant when the P value was < 0.05.
We planned to assess the potential publication bias using funnel plots and the Egger test if more than 10 trials were found. If data were available, we planned to perform a subgroup analysis for major outcomes between collision athletes vs. non-collision athletes. In addition, we planned the following sensitivity analyses for the primary outcomes to assess whether the results of the review were robust to the decisions made during the review process: (1) excluding studies that we judge as “high-risk” for bias, defined as those with a high risk in the domain of the randomization process; (2) excluding studies using imputation statistics.
Assessment of the Certainty of the Evidence
We summarized the findings based on the Cochrane Handbook for Outcomes [17]. We included grading to evaluate the quality of evidence based on the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach for each summary of findings table [18].
Results
Study Selection
In addition to the May 2023 search, we performed an additional search in March 2025. After removing duplicates, 1,948 records were screened for eligibility. After full-text review of 31 studies, four were selected (Figure 2) [10-12,19]. The studies that were excluded during the full-text screening stage are presented in the Appendices.
PRISMA flowchart of the articles included in the systematic reviewPRISMA: Preferred Reporting Items for Systematic Review and Meta-Analyses
Study Characteristics
A total of 354 patients with 383 shoulders (211 shoulders treated with the Bristow technique, and 172 shoulders treated with the Latarjet technique) were included in the four studies [10-12,19].
The average age of patients who participated in these trials was 22.2 years (17.7-29.3 years). The average follow-up duration ranged from 32.4 to 73.5 months (Table 2).
Risk of Bias
One RCT was assessed using RoB 2 and was considered to have some concerns (Figure 3).
RoB 2 risk-of-bias assessmentRoB 2: Risk of Bias 2
Three non-RCT studies were assessed using ROBINS-I, all of which indicated an overall moderate risk of bias (Figure 4).
ROBINS-I risk-of-bias assessmentROBINS-I: Risk of Bias in Non-randomized Studies of Interventions
Primary Outcomes
Redislocation rates were described in four studies, which included 383 shoulders (211 in the Bristow group and 172 in the Latarjet group) [10-12,19]. None of the patients in either the Bristow or Latarjet groups experienced redislocation in any study.
Instability symptoms were described in four studies, which included 383 shoulders (211 in the Bristow group and 172 in the Latarjet group) [10-12,19]. The definition of instability varied among the studies. Belangero et al. assessed instability only by the apprehension test, whereas Shibuya et al. and Tanaka et al. defined it as subluxations [10-12]. Song et al. reported instability using both subluxations and a positive apprehension test [19]. This analysis showed that the Bristow procedure may result in little to no difference in instability symptoms compared to the Latarjet procedure (RR, 0.66; 95% CI, 0.16-2.66; P = 0.55; low certainty of evidence) (Figure 5A; Table 3).
Forest plots of instability symptoms (A), Rowe score (B), return to sports (C), bone nonunion rates (D), and complications (E)
The Rowe score was described in three studies, which included 342 shoulders (192 in the Bristow group and 150 in the Latarjet group) [11,12,19]. The evidence suggests that the Bristow procedure results in a statistically significant difference in Rowe score compared to the Latarjet procedure (MD, 1.73; 95% CI, 0.38-3.07; P = 0.01; moderate certainty of evidence); however, this difference did not exceed the minimal clinically important difference (MCID) of 9.7 points for anterior shoulder instability, indicating that it is unlikely to be clinically meaningful (Figure 5B; Table 3).
Secondary Outcomes
Return to sports was described in three studies that included 342 shoulders (192 in the Bristow group and 150 in the Latarjet group) [11,12,19]. Song et al. evaluated return to sports using a structured four-level classification system (ranging from complete inability to resume sports to full return at the preinjury level) based on clinical assessment and patient-reported outcomes [19]. In contrast, Shibuya et al. and Tanaka et al. reported the timing of return to sports at four to five months after bone union confirmed by CT scans, but did not provide a standardized definition or classification system [11,12]. This analysis showed that the Bristow procedure may result in little to no difference in return to sports compared to the Latarjet procedure (RR, 1.00; 95% CI, 0.94-1.07; P = 0.93; low certainty of evidence) (Figure 5C; Table 3).
Bone nonunion was described in three studies, which included 342 shoulders (192 in the Bristow group and 150 in the Latarjet group) [11,12,19]. Tanaka et al. assessed bone union with CT scans and defined it as continuity of the trabecular bone between the coracoid process and glenoid [12]. Shibuya et al. assessed bone healing with CT scans at three months postoperatively [11]. Song et al. evaluated graft healing with the glenoid at three months and at final follow-up using the method adopted: nonunion was defined as a visible radiolucent line of less than 5 mm, while a radiolucent line greater than 5 mm indicated migration of the bone block; union was classified as bone healing at the graft-glenoid interface [19]. This analysis showed that the Bristow procedure probably results in little to no difference in bone nonunion compared to the Latarjet procedure (RR, 2.09; 95% CI, 0.94-4.62; P = 0.07; moderate certainty of evidence) (Figure 5D; Table 3).
Bone resorption was reported in three studies [10,12,19], but the evaluation methods varied. Belangero et al. assessed bone resorption using radiographs [10]. Song et al. evaluated bone resorption on the latest CT scan using a validated classification system with four grades: grade 0, no resorption; grade I, resorption only near the screw head; grade II, resorption of most of the graft; and grade III, total resorption [19]. Tanaka et al. also assessed bone resorption using CT scans and classified severity into four categories: none, mild, moderate, and severe [12]. Because of these heterogeneous definitions and imaging modalities, a pooled analysis of bone resorption could not be performed.
Complications were described in three studies, which included 276 shoulders (145 in the Bristow group and 131 in the Latarjet group) [10,11,19]. Reported complications encompassed surgical site infection, screw malposition or irritation, transient nerve palsy, and severe postoperative contracture requiring manipulation. This analysis showed that the Bristow procedure may result in little to no difference in complications compared to the Latarjet procedure (RR, 1.06; 95% CI, 0.45-2.49; P = 0.90; low certainty of evidence) (Figure 5E; Table 3).
Additional Analyses
We were unable to assess publication bias using funnel plots or Egger’s test because of the limited number of studies. Among the four included studies, three specifically recruited collision athletes (e.g., rugby or other contact sports), whereas one study included high-demand athletes, comprising both collision and non-collision types, without stratification of outcome data. Due to this inconsistency, subgroup analyses comparing collision versus non-collision athletes could not be performed. A sensitivity analysis for the Rowe score, excluding the study that used imputed statistics, yielded results inconsistent with those of the main analysis (MD, 1.54; 95% CI, -0.33-3.42; P = 0.11).
Discussion
This is the first study to compare the Bristow and Latarjet procedures for ASI by pairwise meta-analysis. The results showed little difference between the Bristow and Latarjet procedures in terms of redislocation rates, symptoms of instability, return to sports, bone nonunion and resorption, and complications; however, the Rowe score may be higher in the Bristow group. However, the difference was only 1.72 points, and considering that the MCID in anterior shoulder instability is at least 9.7 points for the Rowe score, the statistically significant difference in the Rowe score was not considered clinically important [20]. These results suggest that the Bristow and Latarjet procedures have little effect on postoperative clinical outcomes.
In 2019, Garcia et al. systematically reviewed the efficacy of the Bristow and Latarjet procedures for ASI [9]. In this study, 41 studies using the Bristow procedure reported a 1.00 ± 0.20% redislocation rate, and 18 studies using the Latarjet procedure reported a 2.13 ± 0.49% redislocation rate, which is a lower rate with the Bristow procedure than the Latarjet procedure. However, the review did not include RCTs or observational studies that directly compared the two surgical procedures, nor was a pairwise meta-analysis performed. In contrast, the present analysis included only studies that directly compared the Bristow and Latarjet procedures and found that no patients experienced redislocation after either of the two surgical procedures. However, this complete absence of re-dislocation events limited our ability to calculate pooled effect estimates for this outcome. As a result, the statistical power to detect meaningful differences between the procedures was reduced, and the clinical interpretation of their relative effectiveness in preventing redislocation remains uncertain. Nevertheless, a pairwise meta-analysis of instability symptoms suggested little to no difference in perceived instability between the Bristow and Latarjet procedures. However, moderate heterogeneity (I² = 43%) was observed in this outcome. Several factors may explain this inconsistency. First, although the included studies consistently evaluated instability symptoms, the specific definitions varied. Belangero et al. assessed instability solely by a positive apprehension test, Shibuya et al. and Tanaka et al. defined it as recurrent subluxations, and Song et al. combined both patient-reported subluxation episodes and a positive apprehension test [10-12,19]. Second, the study populations differed, with some studies limited to collision athletes such as rugby players, while others included mixed or high-performance athletes with variable recurrence risks. Taken together, these methodological and clinical differences are plausible contributors to the observed heterogeneity and should be considered when interpreting the pooled results.
The Bristow or Latarjet procedures are often applied to collision athletes [21,22]. Shibuya et al. reported no significant difference in the postoperative return-to-sports rates (90.2% for Bristow and 94.8% for Latarjet) for collision athletes using either surgical procedure [11]. Tanaka et al. reported high return-to-play rates for both surgical techniques (100% for Bristow, 96% for Latarjet), suggesting that both procedures were equally effective [12]. In contrast, a significantly higher percentage of collision athletes returned to the same level as before the injury with the Bristow (73.5%) than the Latarjet procedure (65.8%) [19]. The results of the meta-analysis showed that the Bristow and Latarjet procedures may result in little to no difference in return-to-sport rates. Therefore, the results suggest that the two surgical procedures are equally effective in terms of return to sports.
In this study, we analyzed the Rowe score, which was not reported in a previous review [9]. The results showed that the Bristow procedure probably results in little to no difference in the Rowe score compared to the Latarjet procedure (MD, 1.73; 95% CI, 0.38-3.07; P = 0.01). The difference in effect size between the two techniques was so small that, although Bristow appears to be more statistically valid, this difference is not clinically significant. Furthermore, a sensitivity analysis to examine the effect of substituting estimates for missing data found no significant difference in Rowe scores for the two methods (MD, 1.54; 95% CI, -0.33-3.42; P = 0.11). Taken together, these findings indicate that there is no clear difference between the two procedures in terms of the Rowe score, and the apparent effect may be driven by specific studies. However, the inconsistency observed between the primary analysis and the sensitivity analysis weakens the certainty of this outcome. This discrepancy reduces confidence in the robustness of our findings and highlights the need for additional high-quality randomized controlled trials to provide more reliable estimates of the comparative effectiveness of the Bristow and Latarjet procedures.
The condition of the osseous process graft is an important factor affecting the success of the Bristow and Latarjet procedures, with postoperative nonunion or resorption of the osseous process graft likely to result in revision surgery [23]. Two prior reviews reported nonunion rates of 9.4%-10.1% for the Bristow-Latarjet procedure [23,24]. Shibuya et al. compared the nonunion rates for both surgical methods (10.9% for the Bristow procedure and 7.8% for the Latarjet procedure) and reported no significant difference between the two groups [11]. Similarly, Song et al. reported no significant difference in the rate of nonunion (14.7% for the Bristow procedure and 5.3% for the Latarjet procedure) [19]. The results of the present study showed that, although the nonunion rate of the Latarjet procedure (6.9%) was lower than that of the Bristow procedure (11.9%), there was little to no difference between the two groups, similar to the results of a previous study.
Regarding the bone resorption of osseous process grafts, the bone resorption rate was reported to be approximately 70%-90% for the Latarjet procedure and 34.2% for the Bristow procedure [16,18,25,26]. In this meta-analysis, three studies examined bone resorption rates. Song et al. found bone resorption in 8.8% and 2.6% of patients who underwent the Bristow and Latarjet procedures, respectively, with no significant difference [19]. Belangero et al. found bone resorption in one case for each procedure, while Tanaka et al. found it in 6% for Bristow and 100% for Latarjet, but no statistical comparison was made [10,12]. Since these studies were evaluated by X-ray or CT scan, and there were differences in the severity classification of bone resorption between the studies, it was difficult to draw definitive conclusions from a comparison of the bone resorption rates of the two methods. The heterogeneity in bone resorption assessment methods represents a critical methodological issue in this field. The included studies used different imaging modalities (e.g., X-ray and CT scans) and applied inconsistent classification systems for defining and grading bone resorption. This variability not only prevented us from conducting a pooled quantitative analysis but also limited the comparability and interpretability of findings across studies. Such methodological inconsistency may have contributed to the wide variation in reported resorption rates, potentially obscuring the true incidence of this complication. Future studies should adopt standardized imaging protocols and uniform classification criteria to enable more reliable comparisons and synthesis of evidence.
The incidence of postoperative complications of the Bristow-Latarjet procedure in collision athletes ranges from 0.8% to 19.2%, with postoperative infection, postoperative coracoid fracture, severe pain, screw loosening, and screw breakage noted [27]. Three studies reported complications: nerve palsy, postoperative infection, severe contracture, coracoid process avulsion, and screw malpositioning [10,11,19]. Two studies reported complication rates ranging from 2.9% to 21.0% for the Bristow procedure and 7.8% to 9.0% for the Latarjet procedure [10,19]. Shibuya et al. compared the complication rates of both surgical procedures and reported no significant differences between the Bristow (6.5%) and Latarjet (7.0%) procedures [11]. Similarly, the analysis in this study showed that the Bristow (7.5%) and Latarjet procedures (7.6%) may result in little to no difference in complications [10,11,19].
The limitations of this study are as follows. First, the analysis included observational studies as well as RCTs comparing the Bristow and Latarjet procedures. Observational studies inherently have a greater risk of bias because of the non-random allocation of treatments, which limits causal inference and may introduce selection bias. Although some reports suggest that well-designed observational studies in surgical fields can yield results comparable to RCTs [28,29], the predominance of observational evidence in the present analysis remains a major limitation, underscoring the need for further high-quality RCTs to validate the evidence. Second, the participants in these studies were athletes from a variety of sports competitions. Three of the four studies included in this review were conducted with contact athletes, while the remaining study was conducted with high-activity athletes (high-demand athletes) such as soccer, handball, and volleyball players [10-12,19]. Subgroup analyses between collision and non-collision athletes were not performed because of a lack of data. Third, we were unable to assess publication bias using funnel plots or Egger’s test because the number of included studies was insufficient. Therefore, the possibility of publication bias cannot be excluded, which may limit the generalizability of our findings. Fourth, all included studies reported no redislocations in either surgical group. This absence of events limited our ability to perform quantitative analysis for this outcome, thereby reducing the statistical power and interpretability of our findings regarding redislocation. Fifth, the results of this study are based on moderate to low certainty of evidence. The main factor contributing to the low certainty of evidence for many of the outcomes in this study was imprecision. The insufficient sample size and number of events were conspicuous, hindering accurate effect estimates. To address this imprecision issue, ensuring a sufficient sample size in future studies may allow a more accurate capture of the true magnitude of the effects. However, the strength of this study is that it directly compared the clinical outcomes of the Bristow and Latarjet procedures for ASI using a pairwise meta-analysis, providing new insights.
Conclusions
In this study, a pairwise meta-analysis of previously reported clinical outcomes of the Bristow and Latarjet procedures for ASI was conducted and demonstrated little to no difference in redislocation rate, instability symptoms, Rowe score, return to sports, bone nonunion, and complications between the two procedures. However, because the included studies involved athletes from diverse sports, including both collision and non-collision types, without stratification, these findings should be interpreted with caution and may not be fully generalizable across all athlete populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Current concepts in anterior glenohumeral instability: diagnosis and treatment SICOT J Moya D Aydin N Yamamoto N 48720213451963910.1051/sicotj/2021048 PMC 8439181 · doi ↗ · pubmed ↗
- 2The epidemiology and natural history of anterior shoulder instability Curr Rev Musculoskelet Med Galvin JW Ernat JJ Waterman BR Stadecker MJ Parada SA 4114241020172903895110.1007/s 12178-017-9432-5PMC 5685954 · doi ↗ · pubmed ↗
- 3Anterior shoulder instability in the military athlete Sports Health Waterman B Owens BD Tokish JM 514519820162769415110.1177/1941738116672161 PMC 5089361 · doi ↗ · pubmed ↗
- 4Incidence of shoulder dislocation in the United States military: demographic considerations from a high-risk population J Bone Joint Surg Am Owens BD Dawson L Burks R Cameron KL 7917969120091933956210.2106/JBJS.H.00514 · doi ↗ · pubmed ↗
- 5Injuries associated with traumatic anterior glenohumeral dislocations J Bone Joint Surg Am Robinson CM Shur N Sharpe T Ray A Murray IR 18269420122221837810.2106/JBJS.J.01795 · doi ↗ · pubmed ↗
- 6Risk factors for the postoperative recurrence of instability after arthroscopic bankart repair in athletes Orthop J Sports Med Nakagawa S Mae T Sato S Okimura S Kuroda M 2325967117726494520172895969810.1177/2325967117726494 PMC 5593221 · doi ↗ · pubmed ↗
- 7Return to sport after coracoid bone block transfer for shoulder instability: a systematic review HSS J Nadeem IM Vancolen S Horner NS Bedi A Alolabi B Khan M 2963061620203308824310.1007/s 11420-019-09720-z PMC 7534889 · doi ↗ · pubmed ↗
- 8Short-term complications of the Latarjet procedure: a systematic review J Shoulder Elbow Surg Hurley ET Schwartz LB Mojica ES Campbell KA Matache BA Meislin RJ Jazrawi L 169316993020213360733210.1016/j.jse.2021.01.024 · doi ↗ · pubmed ↗