Macaroni Sign in Takayasu Arteritis
Harsh Jain, Sankar J, Kartik Sivasami, AVS Anil Kumar, Neeraj Kumar, Nidhi Goel, Ashish Chandwani, Vivek Vasdev

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
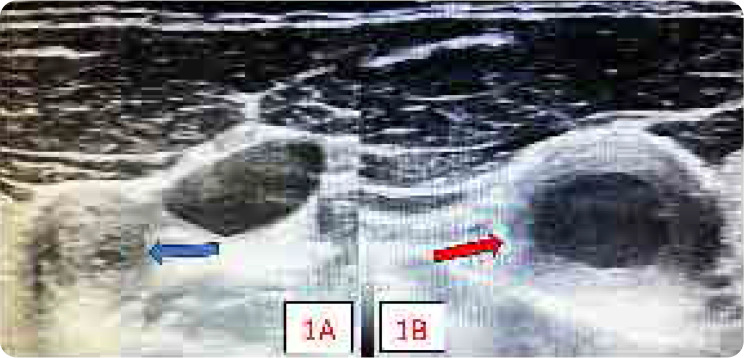 Figure 1
Figure 1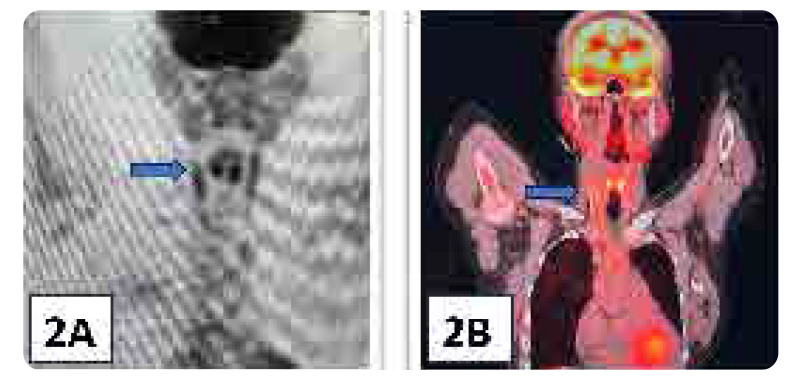 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Renal Diseases and Glomerulopathies · Renal and Vascular Pathologies
An 18-year-old female presented with an 18-month history of limb claudication affecting all four limbs, along with weight loss, tender subcutaneous nodules, and high-grade fever. Examination revealed a systolic blood pressure difference of 20 mmHg between the arms, absent peripheral pulses in both lower limbs, bilateral common carotid artery with a bruit over the right and carotidynia on the left CCA. Laboratory tests showed significantly elevated inflammatory markers, with an erythrocyte sedimentation rate (120 mm/hour) and C-reactive protein (93 mg/L; normal <10). Ultrasonography demonstrated near-complete occlusion of the left common carotid artery at its origin, while the right CCA exhibited homogeneous, mid-echoic circumferential wall thickening (Figure 1A–B). Ultrasonography examination was performed using a 16 MHz hockey stick probe. This ultrasonographic finding is pathognomic of Takayasu’s arteritis (TAK) and has been designated the “macaroni sign”.^1^
Positron emission tomography (PET) revealed features of type V TA along with vessel wall inflammation. Involvement of the left common carotid artery (CCA) showed long-segment narrowing approximately 4 cm from its origin with a minimal luminal diameter of 1 mm due to significant circumferential wall thickening. Beyond this segment, there was a gradual reduction in wall thickness, with an improvement in CCA calibre, reaching a maximum diameter of approximately 3.5 mm. The right CCA exhibited 50–60% luminal narrowing due to vessel wall thickening. PET findings were consistent with the ultrasonographic assessment of the CCA (Figure 2A–B).
Takayasu arteritis is a large-vessel vasculitis of unknown cause, primarily affecting the aorta and its major branches. This leads to segmental narrowing, occlusion, or aneurysm formation. Early diagnosis is crucial, as vascular inflammation is still reversible at this stage. Delayed detection results in fibrosis of the arterial wall, leading to permanent stenosis and occlusion. Comparative research directly evaluating CDS against other imaging modalities remains limited. However, a case series by Czihal et al. demonstrated a strong agreement (83%) between CDS and 18F-fluorodeoxyglucose positron emission tomography (PET) in identifying proximal arm involvement in patients with LVV.^2^ While angiography remains the gold standard for diagnosing TAK, ultrasonography offers a non-invasive alternative, allowing for the identification of characteristic circumferential, long, and homogeneous arterial wall thickening in early disease and monitoring disease activity over time.^3^
AUTHOR CONTRIBUTIONS
All authors made substantial contributions to the conception or design of the work, or the acquisition, analysis, or interpretation of data. All authors were involved in drafting the manuscript or revising it critically for important intellectual content, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Harsh Jain, Sankar J, Nidhi Goel and AVS Anil Kumar contributed to data collection and analysis. Harsh Jain, Sankar J, Neeraj Kumar and S. Kartik contributed to the study design and critical revision of the manuscript. Harsh Jain, Nidhi Goel, Ashish Chandwani, and Vivek Vasdev contributed to data interpretation and manuscript preparation. All co-authors take full responsibility for the integrity and accuracy of all aspects of the work.
PATIENT CONSENT
Written informed consent was taken from the patient.
CONFLICT OF INTEREST
Authors declare no conflict of interest. No ethics/authorship issues related to reported images.
FUNDING
NA.
DATA AVAILABILITY STATEMENT
All available data is included in the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Meini S De Franco V Auteri A Pieragalli D. Images in cardiovascular medicine. Takayasu’s arteritis: the “macaroni sign”. Circulation 2006;114(16):e 544. doi:10.1161/CIRCULATIONAHA.106.62820617043171 · doi ↗ · pubmed ↗
- 2Czihal M Tato F Forster S Rademacher A Schulze-Koops H Hoffmann U. Fever of unknown origin as initial manifestation of large vessel giant cell arteritis: diagnosis by colour-coded sonography and 18-FDG-PET. Clin Exp Rheumatol 2010;28:549–52.20659410 · pubmed ↗
- 3Ghembaza MEA Boulenouar F Lounici A. “Macaroni Sign” in Takayasu Arteritis. J Cardiovasc Imaging 2018;26(3):186–187. doi:10.4250/jcvi.2018.26.e 1830310886 PMC 6160815 · doi ↗ · pubmed ↗