Comparative analysis of external beam radiotherapy versus portal vein stent implantation combined with local and systemic therapy in hepatocellular carcinoma patients with portal vein tumor thrombus: a real-world retrospective study
Wenping Luo, Guodong Wang, Shaojun Chen, Zhe Wang, Chuang Li, Chunwang Yuan, Jingsong Mao, Wenqi Liu

TL;DR
This study compares radiotherapy and stent implantation combined with other treatments for liver cancer patients with vein tumor blockage, finding radiotherapy improves survival.
Contribution
This study provides real-world evidence that EBRT combined with local and systemic therapies improves survival in HCC patients with PVTT.
Findings
EBRT group had significantly higher 6-month objective response and disease control rates compared to PVSI group.
Median overall survival was longer in the EBRT group (35 months vs 19 months).
EBRT and AFP < 400 ng/mL were identified as independent predictors of improved survival.
Abstract
To compare the effectiveness and safety of External Beam Radiotherapy (EBRT) versus Portal Vein Stent Implantation (PVSI) when combined with local interventional therapy and TKI plus ICIs in patients with hepatocellular carcinoma (HCC) and portal vein tumor thrombus (PVTT), providing real-world evidence for clinical decision-making. This retrospective cohort study included patients with HCC and PVTT who received either EBRT or PVSI in combination with transarterial interventional therapy, TKIs, and ICIs between January 2019 and January 2025. The primary effectiveness outcomes were overall survival (OS) and progression-free survival (PFS), which were analyzed using the Kaplan-Meier method and compared using the log-rank test. Secondary outcomes included objective response rate (ORR) and disease control rate (DCR) based on mRECIST criteria. Safety outcomes were assessed by documenting…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1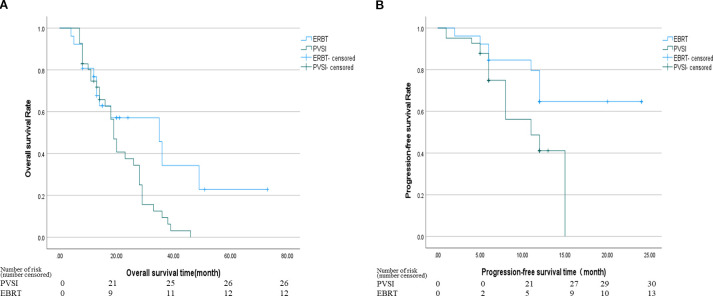 Figure 2
Figure 2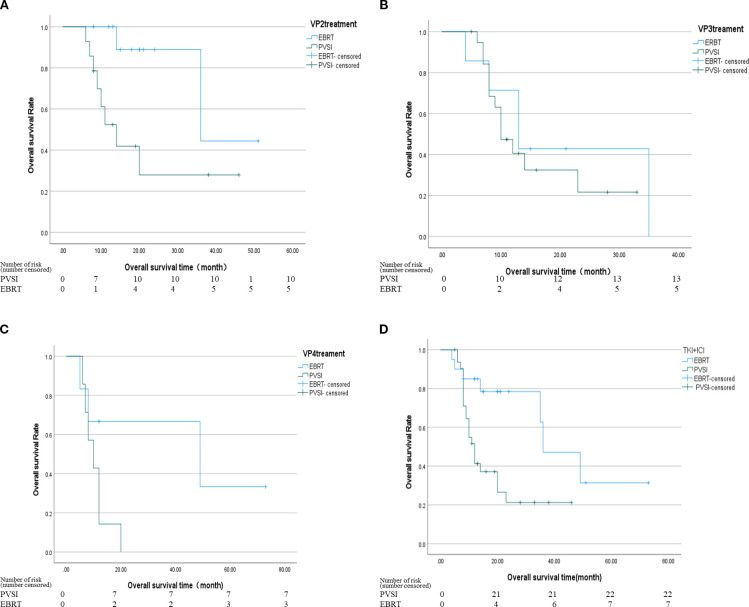 Figure 3
Figure 3| Variables | Group PVSI (n=41) | Group EBRT (n=26) | P Value |
|---|---|---|---|
| Sex | 1 | ||
| Male | 36 (87.8) | 23 (88.5) | |
| Female | 5 (12.2) | 3 (11.5) | |
| Age(years) | 1 | ||
| >60 | 8 (19.5) | 5 (19.2) | |
| ≤60 | 33 (80.5) | 21 (80.8) | |
| ECOG Score | 0.658 | ||
| 0-1 | 37 (90.2) | 23 (88.5) | |
| 2 | 4 (9.8) | 3 (11.5) | |
| CNLC stage | 0.378 | ||
| IIIa | 24 (58.5) | 18 (69.2) | |
| IIIb | 17 (41.5) | 8 (30.8) | |
| Child-Pugh class | 0.727 | ||
| A | 36 (87.8) | 22 (84.6) | |
| B | 5 (12.2) | 4 (15.4) | |
| AFP (ng/ml) | 0.87 | ||
| ≥400 | 26 (63.4) | 17 (65.4) | |
| <400 | 15 (36.6) | 9 (34.6) | |
| tumor size (cm) | 0.245 | ||
| ≥5 | 38 (92.7) | 21 (80.8) | |
| <5 | 3 (7.3) | 5 (19.2) | |
| Extrahepatic metastasis | 1 | ||
| Lung | 7 (41.2) | 3 (37.5) | |
| Bone | 5 (29.4) | 3 (37.5) | |
| Retroperitoneal | 5 (29.4) | 2 (25.0) | |
| Portalhypertension | 0.765 | ||
| Absent | 33 (80.5) | 20 (76.9) | |
| Present | 8 (19.5) | 6 (23.1) | |
| Systemic therapy | 0.642 | ||
| TKI+ICIs | 32 (78) | 19 (73.1) | |
| None | 9 (22) | 7 (26.9) | |
| Portal vein tumor thrombus grading | 0.205 | ||
| VP1 | 0 | 0 | |
| VP2 | 14 (34.1) | 13 (50) | |
| VP3 | 20 (48.8) | 7 (26.9) | |
| VP4 | 7 (17.1) | 6 (23.1) | |
| Local interventional therapy | 0.057 | ||
| RFA(lesions) | 41 (46.6) | 47 (53.4) | |
| TACE (cases) | 72 (52.9) | 64 (47.1) |
| Time | Response | Group PVSI(n=41) | Group EBRT(n=26) | P Value |
|---|---|---|---|---|
| 3 months | CR | 0 (0.0) | 4 (15.4) | |
| PR | 10 (24.4) | 6 (23.1) | ||
| SD | 19 (46.3) | 14 (53.8) | ||
| PD | 12 (29.3) | 2 (7.7) | ||
| ORR | 25 (24.4) | 10 (38.5) | 0.072 | |
| DCR | 29 (70.7) | 24 (92.3) | 0.34 | |
| 6 months | CR | 0 (0.0) | 4 (15.4) | |
| PR | 6 (14.6) | 6 (23.1) | ||
| SD | 18 (43.9) | 12 (46.2) | ||
| PD | 16 (36.6) | 5 (19.2) | ||
| ORR | 6 (14.6) | 10(38.5) | 0.028 | |
| DCR | 24(58.5) | 22 (84.6) | 0.025 |
| Variables | Univariate | Multivariate | ||
|---|---|---|---|---|
| HR (95%CI) | P Value | HR(95%CI) | P Value | |
| Age, <60 vs. ≫60 | 0.859 (0.609-1.211) | 0.386 | 0.573 (0.254-1.297) | 0.182 |
| Portal hypertension, absent vs. present | 0.852 (0.579-1.253) | 0.416 | 0.523 (0.223-1.227) | 0.136 |
| Sex, man vs. woman | 1.077 (0.698-1.622) | 0.736 | 2.185 (0.776-6.154) | 0.139 |
| Classification of portal vein tumor thrombus, VP2 vs. VP3 vs. VP4 | 1.172 (0.471-1.107) | 0.457 | 0.514 (0.210-1.260) | 0.146 |
| Child-Pugh class, A vs. B | 1.124 (0.748-1.689) | 0.574 | 0.889 (0.321-2.461) | 0.821 |
| Tumor size, ≪5 vs. >5 | 0.814 (0.568-1.165) | 0.260 | 0.835 (0.365-1.913) | 0.670 |
| CNLC stage, IIIa vs. IIIb | 1.011 (0.742-1.379) | 0.944 | 0.970 (0.468-2.012) | 0.935 |
| AFP, <400 vs. ≥400 ng/ml | 0.701 (0.496-0.990) | 0.044 | 0.329 (0.137-0.791) |
|
| Treatment, EBRT vs. PVSI | 2.340 (1.187-4.613) | 0.014 | 2.247 (1.090-5.404) |
|
| Interventional therapy, TACE vs RFA | 0.284(0.111-0.725) | 0.080 | 0.354 (0.120-1.045) | 0.060 |
| TKI+ICI vs None TKI+ICI | 0.496(0.227-1.080) | 0.077 | 0.457 (0.185-1.132) | 0.091 |
| Adverse events | Grading | Group PVSI | Group EBRT | P Value |
|---|---|---|---|---|
| Abdominal pain | 1-2 | 5 (12.2) | 4 (15.4) | 0.727 |
| 3-4 | 0 (0) | 0 (0) | ||
| Leukopenia | 1-2 | 3 (7.3) | 12 (46.2) | <0.001 |
| 3-4 | 1 (2.4) | 0 (0) | ||
| Thrombopenia | 1-2 | 5 (12.2) | 8 (30.8) | 0.061 |
| 3-4 | 2 (4.9) | 3 (11.5) | 0.369 | |
| Skin rash | 1-2 | 5 (12.2) | 7 (26.9) | 0.191 |
| 3-4 | 1 (2.4) | 0 (0) | ||
| Hepatic-dysfunction | ||||
| TBIL | 1-2 | 13 (31.7) | 7 (26.9) | 0.677 |
| 3-4 | 9 (22) | 2 (7.7) | 0.181 | |
| ALT | 1-2 | 8 (19.5) | 4 (15.4) | 0.753 |
| 3-4 | 1 (2.4) | 0 (0) | ||
| AST | 1-2 | 29 (70.7) | 10 (38.5) | 0.009 |
| 3-4 | 3 (7.3) | 2 (7.7) | 1 | |
| ALB | 1-2 | 22 (53.7) | 10 (38.5) | 0.225 |
| 3-4 | 8 (19.5) | 2 (7.7) | 0.294 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatocellular Carcinoma Treatment and Prognosis · Liver Disease and Transplantation · Liver Disease Diagnosis and Treatment
Introduction
1
GLOBOCAN 2023 reports 960,000 new cases of Hepatocellular Carcinoma (HCC) worldwide (623,000 in men and 337,000 in women), with an age-standardized mortality rate (ASDR) of 8.3 per 100,000. 47.1% of cases originate from China (1). Since 44% to 62.2% of patients present with Portal vein tumor thrombus(PVTT), HCC is often diagnosed at advanced stages, increasing the risk of variceal hemorrhage and preventing curative surgery (2). The median survival without treatment ranges from 2.7 to 4.0 months (3).
The Barcelona Clinic Liver Cancer (BCLC) staging system classifies hepatocellular carcinoma (HCC) with portal vein tumor thrombosis (PVTT) as BCLC-C, for which the 2022 guidelines recommend systemic therapy (4). In contrast, China’s Primary Liver Cancer Diagnosis and Treatment Guidelines (2024) advocate for combining systemic and local therapies for China Liver Cancer Staging (CNLC) IIIa/IIIb HCC with PVTT (5). Transcatheter arterial chemoembolization (TACE) and External beam radiotherapy (EBRT) are types of local therapies. Among radiotherapy options, external beam radiotherapy (EBRT) precisely targets tumors while sparing healthy tissue, making it suitable for patients with compromised liver function. Portal vein stent implantation with radioactive seeds (PVSI) enhances portal blood flow and tumor control by integrating mechanical stenting with continuous radiation (6–9). The increasing use of targeted therapies and immunotherapies has prompted numerous investigations into their combination with local treatments like TACE and radiotherapy to enhance patient survival outcomes. Current evidence indicates that combining EBRT with TKIs or TKI-ICI regimens achieves superior outcomes compared to TKI monotherapy or TKI-ICI combinations without radiotherapy (10–12). For HCC patients with PVTT, a multimodal strategy incorporating iodine-125 seed strands, portal vein stents, TACE, lenvatinib, and anti-PD-1 antibodies has demonstrated both safety and efficacy (13, 14). The comparative effectiveness of EBRT versus PVSI remains unexplored in previous research. This retrospective analysis assesses their respective safety profiles, treatment outcomes (including objective response rate, duration of response, overall survival, and progression-free survival), and the prognostic value of PVTT grading.
Materials and methods
2
This retrospective study enrolled patients with advanced hepatocellular carcinoma and portal vein tumor thrombosis treated at Liuzhou Workers’ Hospital between January 2019 and January 2025
2.1
HCC diagnosis required clinical or histological confirmation (15, 16), with staging based on the Barcelona Clinic Liver Cancer (BCLC) system (BCLC-C (17)) or China Liver Cancer (CNLC) classification (CNLC IIIa/IIIb). PVTT was assessed using Cheng’s classification in unresectable cases among patients aged 18–75 years. Eligible patients had Child-Pugh A or B liver function (18), an ECOG performance status of 0–2 (19), and PVTT confirmed by triphasic dynamic CT (20) within seven days before treatment; those unsuitable for liver transplantation or percutaneous radiofrequency ablation were included. Exclusion criteria comprised recurrent HCC, distant metastases, prior anticancer therapies (surgery or systemic treatment), Child-Pugh C status, and hepatitis C or HIV coinfection. The study received ethical approval from Liuzhou Workers’ Hospital, with waived informed consent due to its retrospective design. Patients lost to follow-up or with incomplete data were excluded. Given the retrospective nature of this study and its minimal risk to participants, the Ethics Committee of Liuzhou Workers' Hospital waived the requirement for informed consent.
Treatment Measures
2.2
The EBRT group received 3D-CRT or IMRT (5) at a recommended dose of 50–60 Gy. The gross tumor volume (GTV) encompassed intrahepatic PVTT and adjacent lesions, unless excluded due to minimal liver volume or high tumor burden. The planning target volume (PTV) was defined as GTV plus a 3–5 mm margin. Dose constraints included a mean liver dose of <28–30 Gy for Child-Pugh A patients and <6 Gy for Child-Pugh B patients; radiation therapy was contraindicated for Child-Pugh C cases (21, 22). Additional constraints were V5 <5% for the small bowel, V45 <45% for the stomach (maximum dose <54 Gy), spinal cord maximum <45 Gy, and mean kidney dose <15 Gy The maximum dose for both the stomach and the small intestine should be less than 54 Gy, with V for the stomach <45% and V for the small intestine ≤5%. The average dose of both kidneys is ≤15Gy. If the average dose of one kidney is greater than 19Gy, the other kidney should be avoided as much as possible. The maximum dose to the spinal cord is <45 Gy (23).
Group PVSI: (1) Preoperative planning using the TPS system involved precise delineation of the portal vein tumor thrombus target area on portal venous phase contrast-enhanced CT scans. The treatment plan used 125I seeds with 0.6-0.8 mCi activity per seed, delivering a prescribed internal radiotherapy dose of 70–150 Gy. The planned target volume achieved over 90% coverage of the tumor thrombus (V90 > 90%), with dosimetric parameters meeting D90 > 90%, BED10 > 140 Gy, and EQD2 > 80 Gy. To prevent severe complications such as radiation-induced ulcers, perforations, or fistulas, the gastrointestinal tract (including the duodenum and stomach) should receive a D1cc below 30–40 Gy, with an absolute maximum dose (Dmax) not exceeding 50 Gy. The liver V30 must remain under 30% to minimize the risk of radiation-induced liver disease. The Dmax to the portal vein wall hotspot should be constrained to 150–200 Gy to avoid vascular rupture and bleeding, while the common bile duct Dmax should be kept below 100 Gy to prevent radiation-induced stenosis. The spinal cord Dmax must not exceed 20–25 Gy, and the kidney V15 should be limited to less than 30%. (2) Seed chain preparation followed the TPS plan by loading seeds into the implant gun and connecting them to a 4F drainage catheter. The push rod sequentially advanced seeds to form a densely packed chain, confirmed under DSA fluoroscopy to span the entire tumor thrombus length. (3) The hybrid CT-DSA procedure for seed stent implantation began with CT-guided selection of an optimal percutaneous puncture route to the portal vein branch subsegment. After standard sterile preparation, an 18G coaxial needle punctured the portal vein branch, followed by guidewire exchange and 8F sheath placement. DSA guidance facilitated 6F guiding catheter insertion using a double-stiff-wire technique, with angiography confirming tumor thrombus location and guidewire positioning. A portal vein stent (88×12 mm or 100×20 mm) was deployed over the stiff wire, followed by custom seed chain delivery through the 6F catheter. Post-deployment DSA verified proper seed chain positioning within the stent lumen. An 8F balloon expanded the stent to compress the seed chain, with final angiography confirming optimal stent placement and portal vein patency. The procedure concluded with sheath removal, pressure dressing application, and 4-hour monitoring. Postoperative day 1, abdominal ultrasound and complete blood count were assessed for complications.
Systemic therapy included TKIs (lenvatinib, donafenib, or sorafenib) administered per guidelines, paused three days before and after intervention. ICIs (camrelizumab, tislelizumab, or sintilimab) were infused at 200 mg every three weeks. All patients received at least one cycle (3–4 weeks) of systemic therapy with TKI plus ICI before local treatment (EBRT or PVSI), ensuring an initial systemic response before commencing local intervention. Commonly used first-line TKI combined with ICI regimens include "Lenvatinib + Tislelizumab", "Sintilimab + Sorafenib", and "Apatinib + Camrelizumab". Discontinue treatment upon disease progression, intolerable adverse reactions, or patient withdrawal of consent. Adjuvant TACE or RFA was completed within one month post-PVSI or EBRT. For patients with hepatocellular carcinoma presenting with portal vein tumor thrombosis, the choice between external beam radiotherapy and portal vein stent implantation depends on specific clinical indications, tumor anatomy, and hepatic functional reserve. This determination was made following evaluation by a multidisciplinary team in accordance with established consensus guidelines. Such a collaborative decision-making approach reflects our institutional standard of care. All patients receive comprehensive counseling regarding the potential benefits and risks of each treatment option, tailored to their individual disease status. The final treatment plan incorporates both the multidisciplinary team’s recommendation and the patient’s fully informed consent. (Figure 1).
Patient selection flow chart.
Data collection and monitoring
2.3
We recorded treatment parameters (EBRT dose, seed activity) and baseline characteristics (age, HBV status, cirrhosis, Child-Pugh score, PVTT grade, AFP levels). Follow-up assessments occurred monthly after treatment initiation, with tri-monthly CT scans and blood tests measuring tumor biomarkers and hepatic function; MRI supplemented these evaluations when clinically indicated. Outcomes included tumor response, progression-free survival (PFS), overall survival (OS), objective response rate (ORR), disease control rate (DCR), and adverse events (AE). PFS spanned from treatment commencement to disease progression or death, while OS extended from treatment initiation to death. ORR quantified patients achieving partial or complete responses (PR/CR), whereas DCR encompassed those with stable disease (SD), PR, or CR. Tumor response adhered to the modified Response Evaluation Criteria in Solid Tumors (mRECIST) (24). Adverse events were graded per the National Cancer Institute’s Common Terminology Criteria for Adverse Events (NCI-CTCAE) (25) version 5.0.
Statistical analysis
2.4
IBM Corp.’s SPSS v27.0 was used to analyze the data. Means ± standard deviation (SD) and percentages (%) were used for continuous and categorical data, respectively. PFS and OS were estimated using Kaplan-Meier curve analysis and compared with the log-rank test. Cox regression was performed as a univariate analysis. Subgroup analysis: Treatment (with or without systemic therapy) and PVTT grade (VP2/3/4) were stratified.
Results
3
Features of the patient
3.1
This retrospective study analyzed 67 HCC patients with PVTT (Table 1). The cohort comprised 41 patients receiving portal vein stent implantation combined with TACE/RFA and TKI+ICIs, and 26 patients treated with external beam radiation (EBRT) plus TACE/RFA and TKI+ICIs; both groups exhibited similar age distributions and male predominance. The baseline characteristics, including ECOG scores, Child-Pugh classification, AFP levels, PVTT severity, tumor type, and the distribution of maximum tumor diameters, were similar across all groups. No statistically significant differences were observed among the groups (P > 0.05), confirming their comparability. The EBRT group received a median radiation dose of 54.0 ± 1.0 Gy (range: 50–60 Gy). No seed migration occurred in the PVSI group, which had a median implantation of 35.0 ± 11.5 125I seeds (range: 25-60). RFA treated 88 lesions (47 in EBRT, 41 in PVSI), while 136 TACE procedures were performed across 67 patients (64 in EBRT, 72 in PVSI). Combined TKI+ICIs therapy averaged 3.2 ± 1.8 cycles (range: 2-5) in the EBRT group and 2.8 ± 1.5 cycles (range: 1-4) in the PVSI group. The distant metastasis patterns of the two groups were largely similar, with the lungs, bones, and retroperitoneal lymph nodes serving as the primary sites.
Survival analysis
3.2
Table 2 demonstrates superior short-term efficacy in the EBRT group compared to PVSI (median follow-up 21.0 months; range 4–72 months), with significantly higher 6-month ORR (38.5% vs. 24.4%, p=0.028) and DCR (84.6% vs. 58.5%, p=0.025). Figures 2A, B reveal that the median OS was 35 months (95%CI, 14.5-55.5 ) in group EBRT and 19 months in group PVSI (95%CI, 16.9-21.1) (p = 0.044), the median PFS was not reached in the EBRT group and 11 months (95% CI, 6.2-15.8) in the PVSI group (p = 0.037). Multivariate analysis confirmed that EBRT treatment (HR=2.247, 95% CI, 1.090–5.404, P=0.030) and AFP < 400 ng/ml (HR=0.329, 95% CI, 0.137-0.791, P=0.013) were independent predictors of overall survival (Table 3). Further subgroup analysis revealed a particularly pronounced survival benefit from EBRT in patients with VP2-type portal vein tumor thrombus and in those treated with TKI plus ICI therapy. For patients with VP2 thrombus, median overall survival was 36 months (95% CI: 5.1–66.9) in the EBRT group compared to 14 months (95% CI: 8.0–20.0) in the PVSI group (p = 0.017). Among those receiving TKI and ICI combination therapy, median overall survival was 36 months (95% CI: 20.1–51.9) with EBRT versus 12 months (95% CI: 9.7–14.3) with PVSI (p = 0.005) (Figures 3A–D).
(A) The median OS was 35 months (95% CI, 14.5-55.5) in the EBRT group and 19 months (95% CI, 16.9-21.1) in the PVSI group (p = 0.044). (B) The median PFS was not reached in the EBRT group and 11 months (95% CI, 6.2-15.8) in the PVSI group (p = 0.037).
(A) The median OS was 36 months (95% CI, 5.1-66.9) in the EBRT group and 14 months in the PVSI group (95% CI, 8.0-20.0) (p = 0.017); (B) The median OS was 13 months (95% CI, 6.6-19.4) in the EBRT group and 10 months (95% CI, 7.0-13.0) in the PVSI group (p = 0.507); (C) The median OS was 49 months (95% CI, 0.0-110.4) in the EBRT group and 10 months (95% CI, 4.9-15.1) in the PVSI group (p = 0.066); (D) The median OS was 36 months (95% CI, 20.1-51.9) in the EBRT group and 12 months (95% CI, 9.7-14.3) in the PVSI group (p = 0.005).
Safety analysis
3.3
The treatment did not induce severe side effects such as radiation hepatitis, liver abscess, acute liver failure, or abdominal bleeding. The most frequent grade 1–2 adverse events were fever, fatigue, nausea, vomiting, abdominal discomfort, rash, abnormal liver function, and bone marrow suppression. Leukopenia occurred more often in the EBRT group than in the PVSI group (46.2% vs. 7.3%, P < 0.001). For patients presenting with grade 1–2 hematologic toxicity, EBRT treatment was not routinely interrupted. All patients received prophylactic supportive care, including oral leukocyteelevating agents such as Leukine. EBRT or TKI treatment was suspended only in cases of grade 3 or higher hematologic toxicity, with adjunct use of recombinant human granulocyte colony-stimulating factor (G-CSF). No patient in this study permanently discontinued treatment due to hematologic toxicity. Conversely, grade 1–2 AST elevation was more prevalent in the PVSI group (70.7% vs. 38.5%, P = 0.009), suggesting greater liver dysfunction in these patients. Grade 3–4 adverse events were rare in both groups, though the PVSI group exhibited nearly 20% rates of TBIL and ALB abnormalities. All adverse events were resolved with symptomatic management. Table 4 summarizes the adverse reactions observed in both cohorts.
Discussion
4
This study compared the safety and effectiveness of external Beam Radiotherapy (EBRT) versus Portal Vein Stent Implantation (PVSI) when combined with local interventional therapy and TKI plus ICIs in patients with hepatocellular carcinoma (HCC) and portal vein tumor thrombus (PVTT) in a real-world setting. The findings showed that the EBRT group experienced significantly greater survival benefits than the PVSI group: the 6-month objective response rate (ORR) and disease control rate (DCR) were notably higher (38.5% vs. 24.4%; 84.6% vs. 58.5%), median overall survival (OS) nearly doubled (35 months vs. 19 months, P = 0.044), and the progression-free survival (PFS) of the EBRT group did not reach the endpoint. Compared with the EBRT group in this study, Sahai et al. (26) reported a median OS of 10.9 months for radiotherapy combined with systemic therapy and DEB-TACE, and observed significantly prolonged survival among patients with PVTT remission, indicating that radiotherapy effectively controls PVTT. These findings offer external validation for the survival outcomes observed in the EBRT group of this study. The results are consistent with previous findings by Tang (27), who demonstrated the therapeutic benefits of radiotherapy for HCC with PVTT. Their study revealed that tumor antigen exposure induced inflammatory responses, modulated immune markers, and promoted tumor necrosis. However, our results differ from those reported by Tan et al. (28). Their subgroup analysis demonstrated superior overall survival (11.7 vs. 7.6 months, p < 0.001) for VP4-type PVTT patients receiving PVSI compared to EBRT, supporting the conclusion that PVSI + TACE yields better survival outcomes for PVTT HCC patients than RT + TACE. One possible explanation is that most PVTT cases in this study were of the VP2 type, whereas Tan’s study mostly involved VP4 type PVTT (50 out of 53 cases). This further suggests that PVSI can quickly open blood vessels in fully blocked VP4 thrombi, while EBRT can precisely target tumors in VP2 thrombi with partial blood flow. Additionally, this study combined TACE/RFA and (TKI+ICIs), whereas Tan’s study used only TACE. The increased effectiveness of TKI+ICIs might partly explain the survival benefit observed in the EBRT group. Furthermore, the use of TKI+ICIs for liver cancer treatment may have been enhanced by irradiation (27), as Tan’s research did not incorporate systemic treatments beyond that, which could limit long-term effectiveness. The third reason is that this study employed a conventional single-row particle chain, whereas Tan et al. used a four-row I-125 particle scaffold offering 360 coverage. This configuration may promote rapid vascular expansion. Consequently, for patients with VP4-type tumors, the PVSI approach did not yield superior outcomes compared to EBRT in this investigation.
According to the study’s subgroup analysis, the median overall survival (OS) for patients with VP2 type tumor thrombus following EBRT was 36 months, compared to 14 months in the PVSI group (P = 0.017), indicating that tumor thrombus classification is a significant predictor of success. Radiotherapy can more effectively treat the local lesion and preserve liver function in cases of VP2 type tumor thrombus, which involves the secondary branch of the portal vein and does not completely block the main blood flow. However, VP3/VP4 classifications may better guide goal-oriented PVSI due to their association with more extensive tumor thrombus invasion (29). This stratified outcome emphasizes the need for customized care, and moving forward, a type-specific approach based on imaging characteristics should be developed. Given the relatively small sample size of the VP3/VP4 subgroup, this analysis remains exploratory, and its findings require validation through larger future studies.
The EBRT group exhibited significantly higher hematological toxicity, with grade 1–2 leukopenia occurring in 46.2% of patients versus 7.3% in the PVSI group (P < 0.001), reflecting bone marrow suppression and underscoring the importance of enhanced hematopoietic monitoring. Liver function abnormalities were more pronounced in the PVSI group, where AST levels rose in 70.7% of cases compared to 38.5% (P = 0.009), likely due to localized particle radiation and mechanical injury to hepatic sinusoidal endothelial cells during stent placement. These findings corroborate the mechanisms reported by Tan et al. (28, 30). Among the grade 3 adverse events, the most common were thrombocytopenia, elevated bilirubin, elevated AST, and elevated ALB. The incidence of each event, however, remained below 20%. Both groups showed relatively low rates of severe adverse events (》grade 3). There was no statistically significant difference, suggesting that the toxicity profiles of both treatments align with their known effects and are safe and manageable within the study cohort.
Multivariate analysis identified EBRT treatment (HR=2.247) and AFP < 400 ng/ml (HR = 0.329) as independent prognostic factors. Lower AFP levels correlated with improved response to comprehensive treatment, consistent with its established role as a biomarker for hepatocellular carcinoma aggressiveness. These findings reinforce the utility of AFP in pretreatment risk stratification and corroborate the PVTT prognostic model reported by Peng et al. (31). In addition to the prognostic relevance of alpha-fetoprotein (AFP) that we observed in our research, there is also a growing interest in incorporating serum biomarkers such as AFP and des-gamma-carboxy prothrombin (DCP) into the diagnostic algorithms for screening and monitoring hepatocellular carcinoma (HCC), especially in high-risk populations. For these patients, especially those with markedly elevated AFP and DCP alongside vascular invasion or high risk of early recurrence, more aggressive local therapies like external beam radiotherapy (EBRT) may be warranted over transarterial chemoembolization (TACE) or other interventional approaches. Such cases often respond poorly to conventional interventional treatments, whereas EBRT can achieve broader local control, particularly for tumors in challenging locations or with extensive vascular involvement (32).
Limitations and prospects
5
The study has several limitations, including potential selection bias due to its retrospective design. The small sample size (n = 67) may limit the reliability of subgroup analyses, particularly since the VP3/VP4 subgroup did not exhibit significant differences. The observation period should be extended, since the median PFS in the EBRT group did not reach the threshold, suggesting insufficient follow-up. Furthermore, the impact of radiotherapy techniques such as SBRT on survival has not been evaluated. The analysis did not account for subsequent second or third-line treatments, which may confound the attribution of survival benefits. Another constraint is the limited number of patients in the VP2 subgroup. These results should thus be interpreted as preliminary and warrant validation in larger prospective studies. In this study, the absolute number of grade 3 or higher adverse events was relatively small. Further confirmation of these findings is needed in a larger cohort in the future. Sensitivity analysis was not conducted to assess the potential impact of unmeasured confounding factors. While this study did not investigate novel mechanisms or biomarkers, our clinically derived findings illuminate a path for future translational research. Subsequent studies could explore which biomarkers—such as specific genetic mutations or features of the immune microenvironment — might identify patient subgroups most likely to benefit from EBRT- or PVSI-based combination strategies.
Conclusion
6
Hepatocellular carcinoma (HCC) patients with portal vein tumor thrombus (PVTT) exhibit significantly improved survival when treated with combined external beam radiotherapy (EBRT), local interventional procedures, and tyrosine kinase inhibitors plus immune checkpoint inhibitors (TKI+ICIs). Patients with VP2-type PVTT achieve a median survival of nearly three years with this approach. Clinicians must remain vigilant regarding hematological toxicity. Clinical decision-making should incorporate four-dimensional assessments, including bone marrow tolerance, hepatic functional reserve, AFP levels, and tumor thrombus classification. While portal vein stent implantation (PVSI) serves as a crucial alternative for patients with compromised liver function or VP3/VP4-type PVTT, EBRT remains the preferred option for VP2-type cases with preserved bone marrow function. Further investigations should prioritize refining radiation techniques, optimizing dosing protocols, developing advanced particle stent materials, and implementing biomarker-guided personalized therapies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1International Agency for Research on Cancer. Global cancer observatory: liver cancer fact sheet 2023. Lyon, France: World Health Organization (2023).
- 2Ellis L Canchola AJ Spiegel D Ladabaum U Haile R Gomez SL. Trends incancer survival by health insurance status in california from 1997 to 2014. JAMA Oncol. (2018) 4(3):317–23. doi: 10.1001/jamaoncol.2017.3846, PMID: 29192307 PMC 5885831 · doi ↗ · pubmed ↗
- 3Soin A Lesurtel M Bhangui P Cocchi L Bouattour M Clavien PA. Are patients with hepatocellular carcinoma and portal vein tumor thrombosis candidates for liver transplantation? J Hepatol. (2023) 78:1124–9. doi: 10.1016/j.jhep.2023.03.032, PMID: 37208099 · doi ↗ · pubmed ↗
- 4Reig M Forner A Rimola J Ferrer-Fàbrega J Burrel M Garcia-CriadoÁ. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J Hepatol. (2021) 76(3):681–93. doi: 10.1016/j.jhep.2021.11.018, PMID: 34801630 PMC 8866082 · doi ↗ · pubmed ↗
- 5National Health Commission of the People's Republic of China. Guidelines for the diagnosis and treatment of primary liver cancer (2024 edition). J Clin Hepatol. (2024) 40:893–918. doi: 10.21147/j.issn.1000-9604.2019.02.02, PMID: 31156298 PMC 6513740 · doi ↗ · pubmed ↗
- 6Li S Guo JH Lu J Wang C Wu H Wang H. I 125 irradiation stent for treatment of hepatocellular carcinoma with portal vein thrombosis: A meta-analysis. Cancer Radiother. (2021) 25:340–9. doi: 10.1016/j.canrad.2020.12.003, PMID: 33455874 · doi ↗ · pubmed ↗
- 7Zhang ZH Zhang W Gu JY Liu QX Ma JQ Liu LX. Treatment of hepatocellular carcinoma with tumor thrombus using iodine-125 seed strand implantation and transarterial chemoembolization: a propensity-score analysis. J Vasc Interv Radiol. (2018) 29:1085–93. doi: 10.1016/j.jvir.2018.02.013, PMID: 29754851 · doi ↗ · pubmed ↗
- 8Hong D Zhou Y Wan X Su H Shao H. Brachytherapy with Iodine-125 seeds for treating portal vein-branch tumor thrombus in patients with hepatocellular carcinoma. BMC Cancer. (2021) 21:1020. doi: 10.1186/s 12885-021-08680-0, PMID: 34521375 PMC 8439081 · doi ↗ · pubmed ↗