Polyembolokoilamania and Beyond: A Clinical Case Series on Urological Foreign Bodies of Diverse Aetiologies and Management Strategies
Vijayanand Mani, Bhavyadeep Korrapati, Velmurugan Palaniyandi, Hariharasudhan Sekar, Sriram Krishnamoorthy

TL;DR
This paper presents three unique cases of foreign bodies in the urinary tract, highlighting the challenges in diagnosis and the need for tailored treatment approaches.
Contribution
The paper contributes a clinical case series showcasing diverse causes and management strategies for urological foreign bodies.
Findings
Foreign bodies in urology can arise from self-insertion, trauma, or disease-related migration.
Treatment requires individualized approaches, ranging from endoscopic to surgical interventions.
Multidisciplinary care improves outcomes, especially in complex behavioral or systemic cases.
Abstract
Urological foreign bodies, while uncommon, represent a clinically significant challenge due to their diverse aetiologies. They often lead to complex diagnostic dilemmas and require tailored, sometimes multidisciplinary, therapeutic interventions. These may result from self-insertion, penetrating trauma, or transorganic migration, and are associated with major complications such as infection, obstruction, and fistula formation. This series of cases attempts to demonstrate the varied aetiologies, diagnostic difficulties, and treatment approaches of urological foreign bodies seen in a tertiary referral centre. There are three case presentations, each illustrating a unique mechanism. The first case was a 22-year-old man who self-inserted an electric tube casing into the urethra for autoerotic stimulation - a case of polyembolokoilamania. The second case was a 52-year-old man with a chronic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
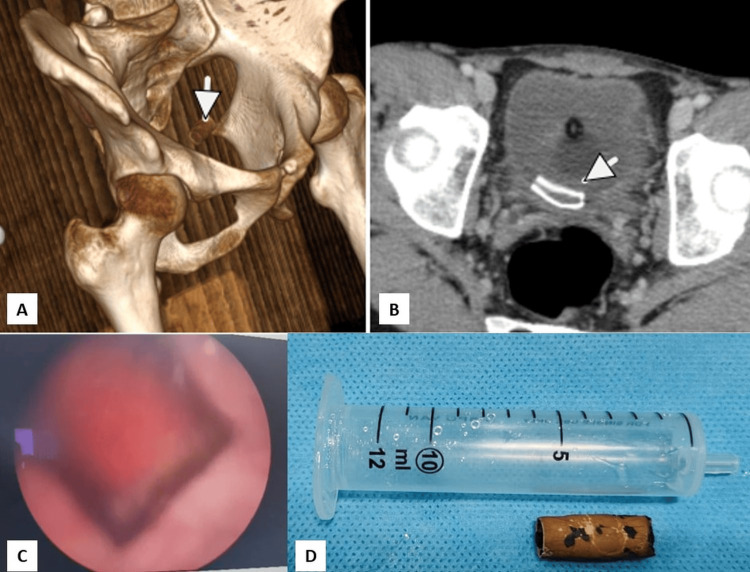 Figure 1
Figure 1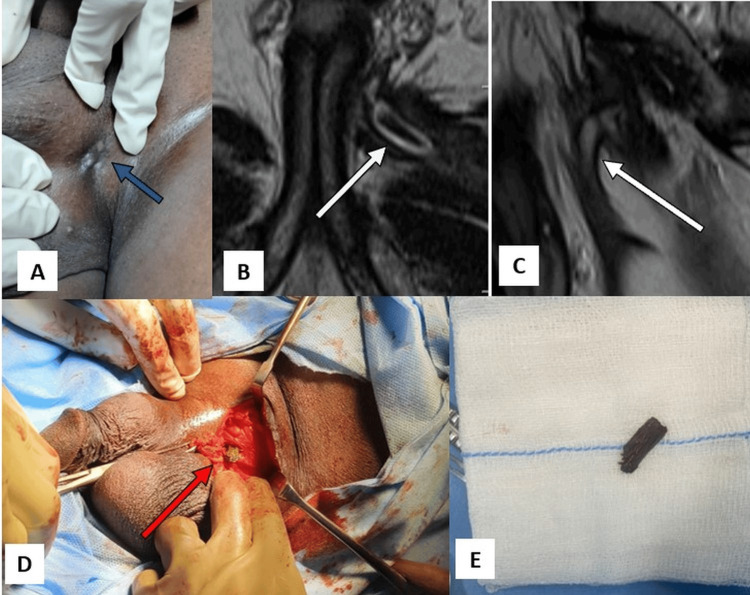 Figure 2
Figure 2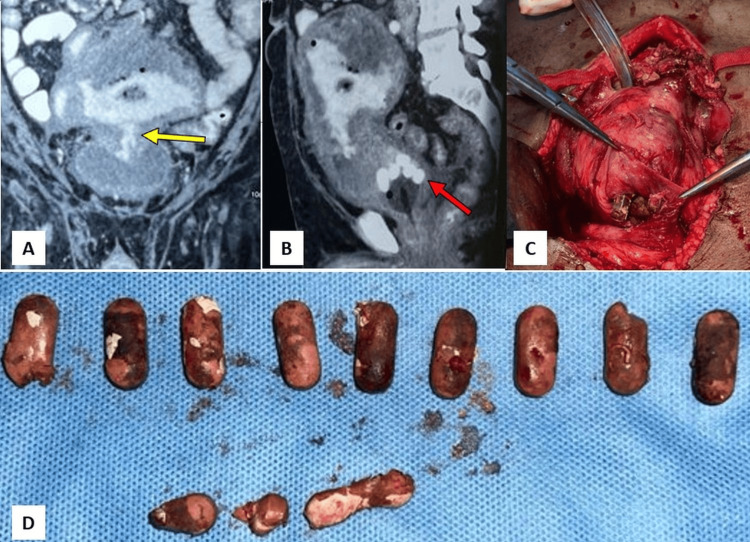 Figure 3
Figure 3| Case | Age/Sex | Aetiology | Complaints | Imaging/Labs | Outcome |
| 1 | 22/M | Self-insertion (autoerotic) | Haematuria, suprapubic discomfort | CT, cystoscopy | Endoscopic retrieval |
| 2 | 52/M | Penetrating trauma | Purulent scrotal discharge | MRI, WBCs: 13,450 cells/mm³ | Open surgical exploration |
| 3 | 64/M | Iatrogenic (Crohn's fistula) | Dysuria, abdominal pain, fever | CT, laparotomy | Open surgery, bladder repair |
| Study | Study Type/Design | Aetiologies Covered | Imaging Modalities | Management | Key Highlights |
| Current study | Case series (n=3) | Self-insertion, penetrating trauma, enterovesical fistula | CT, MRI, cystoscopy | Endoscopic and open surgical removal | Multidisciplinary approach, inclusion of Crohn's related fistula polyembolokoilamania |
| Bansal et al. (2016) [ | Single-centre retrospective study (n=49) | Self-insertion, iatrogenic, migration | X-ray, ultrasonography, cystoscopy | Endoscopic (majority), surgical (minority) | Largest Indian series, focus on retrieval outcomes |
| Eckford et al. (1992) [ | Five-year retrospective review (n=27) | Mainly self-insertion, some iatrogenic | X-ray, cystoscopy | Endoscopic (most cases) | Early UK dataset, focus on sexual gratification cases |
| Unruh et al. (2012)[ | Narrative review with case insight | Polyembolokoilamania (psychiatric context) | Not applicable | Psychiatric evaluation and literature synthesis | Highlights psychiatric diagnosis and implications |
| Jang et al. (2012) [ | Case report | Penetrating trauma | MRI | Open surgical retrieval | Delayed diagnosis due to a radiolucent organic foreign body |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForeign Body Medical Cases · Ureteral procedures and complications · Hemostasis and retained surgical items
Introduction
Urological foreign bodies are an uncommon yet clinically significant entity, associated with substantial morbidity, including urinary tract infections, haematuria, obstruction, and fistula formation. These objects may be introduced through self-insertion (often for sexual gratification), penetrating trauma, migration from adjacent organs, or iatrogenic mechanisms [1-3]. Diagnosis requires a comprehensive clinical history, a high index of suspicion, and advanced imaging modalities, with endoscopic retrieval often preferred due to its minimally invasive nature. However, open surgical approaches may be necessary for complex cases [4].
Polyembolokoilamania, defined as the recurrent self-insertion of foreign objects into body orifices for autoerotic or psychiatric reasons, represents a central aetiology in such cases [5]. These conditions are diagnostically challenging, as patients may be reluctant to disclose insertion history, and some objects (e.g., wood, plastic) are radiolucent and not easily detected on conventional imaging. The clinical significance lies in the risk of delayed diagnosis, leading to infection, chronic inflammation, or fistula formation. While precise epidemiological data are scarce, reports suggest variable incidence globally, with scattered regional data indicating increasing recognition, partly due to evolving sexual practices and complex medical interventions. Other reasons include the rising prevalence of complex inflammatory conditions like Crohn's disease and an increase in invasive medical procedures.
This case series presents three distinct cases of urological foreign bodies managed at a tertiary care centre, highlighting diverse aetiologies, diagnostic strategies, and tailored therapeutic approaches. By elucidating these cases, we aim to contribute to the limited literature on standardised protocols and emphasise the role of multidisciplinary care in achieving optimal outcomes.
Case presentation
Case 1: Urethral self-insertion for autoerotic purposes
Red flag feature: Unexplained haematuria with suprapubic discomfort in a young male.
A 22-year-old male student presented with haematuria and suprapubic discomfort. The physical examination was unremarkable, but the urinalysis confirmed microscopic haematuria. Blood parameters, including complete blood count and renal function, were within normal limits. Contrast-enhanced CT of the abdomen and pelvis revealed a foreign body in the bladder (Figures 1A-1B). Upon establishing rapport and ensuring confidentiality, the patient disclosed a history of inserting an electrical rubber casing into his urethra for autoerotic stimulation. This is a behaviour consistent with polyembolokoilamania. Cystoscopy confirmed the presence of the object, which was retrieved using endoscopic graspers (Karl Storz/Wolf, Germany) (Figures 1C-1D). The patient received counselling on associated risks and was referred for psychiatric evaluation to assess for polyembolokoilamania, a condition characterised by recurrent foreign body insertion. Recovery was uneventful, with no complications noted at the six-month follow-up.
Imaging and retrieval of self-inserted urethral foreign body (Case 1). (A) 3D reconstructed CT scan showing a tubular foreign body within the bladder (white arrowhead). (B) Axial CT scan demonstrating encrustation over the foreign body (white arrowhead). (C) Cystoscopic view of the foreign object within the bladder. (D) Retrieved electrical rubber casing placed adjacent to a 10 mL syringe for scale comparison.
Case 2: Penetrating trauma with an organic foreign body
Red flag feature: Chronic discharging sinus at the scrotal root following trauma.
A 52-year-old male farmer presented with a six-month history of persistent purulent discharge from a sinus at the left hemiscrotum. He attributed it to a penetrating injury sustained during a fall onto farming equipment. Examination revealed a 2 cm discharging sinus at the left scrotal junction (Figure 2A). Laboratory tests showed a mild leukocytosis (13,450 cells/mm³); other parameters were normal. MRI identified a foreign body within the adductor brevis muscle, associated with a 2 cm sinus tract to the scrotum (Figures 2B-2C). Open surgical exploration revealed a wooden splinter, which was removed (Figures 2D-2E). The patient recovered fully, with complete resolution of all symptoms.
Imaging and surgical management of penetrating traumatic urological foreign body (Case 2). (A) Clinical photograph showing a discharging sinus at the left scrotal root (blue arrow). (B) Axial T1-weighted MRI revealing a sinus tract extending into the adductor region (white arrow). (C) Sagittal T1-weighted MRI showing the trajectory of the tract containing the foreign body (white arrow). (D) Intraoperative image demonstrating retrieval of a wooden splinter from the tract (red arrow). (E) Extracted organic foreign body placed on a surgical gauze.
Case 3: Iatrogenic foreign body secondary to enterovesical fistula
Red flag feature: Lower urinary tract symptoms (LUTS) with a history of Crohn’s disease.
A 64-year-old male businessman with a three-year history of Crohn's disease, managed with mesalamine, presented with dysuria, lower abdominal pain, and fever. Contrast-enhanced CT of the abdomen and pelvis revealed a loculated pelvic abscess with air pockets, enteroliths, and an enterovesical fistula, likely from a contained small bowel perforation (Figures 3A-3B). Laparotomy confirmed an inflammatory phlegmon involving the mid-jejunal loops, sigmoid colon, and bladder, adherent to the anterior abdominal wall (Figure 3C). Surgical resection and anastomosis of the affected bowel segments were performed, and the bladder dome was excised. Intraoperatively, multiple intact undissolved mesalamine tablets - colloquially termed "ghost tablets" (i.e., intact but pharmacologically inactive remnants of tablets) - were meticulously extracted from the bladder lumen (Figure 3D). This confirmed their migration via the fistula as the source of the patient's symptoms and radiographic findings. Primary repair was completed with a suprapubic catheter (SPC) (18 Fr Foley catheter; Romsons Scientific & Surgical Pvt. Ltd., Agra, India) placement. The SPC was removed after two weeks, and the postoperative course was uneventful. Symptoms resolved, with no fistula recurrence noted at the six-month follow-up.
Imaging and surgical retrieval of intravesical foreign bodies migrated via enterovesical fistula in Crohn’s disease (Case 3). (A) Coronal contrast-enhanced CT showing a phlegmonous mass with fistulous communication to the bladder (yellow arrow). (B) Sagittal CT revealing multiple hyperdense intravesical foreign bodies (undissolved tablets) mimicking enteroliths (red arrow). (C) Intraoperative image demonstrating the extraction of retained mesalamine tablets through a bladder incision. (D) Multiple undissolved mesalamine tablets (“ghost tablets”) retrieved from the urinary bladder and laid out on a surgical drape.
Summary of the cases
A summary of all three cases is listed in Table 1.
Discussion
The presence of a foreign body should be considered a critical, albeit rare, event. It calls for differential diagnosis in any patient presenting with LUTS, particularly when symptoms are atypical, recurrent, or refractory to standard treatment. Routes of entry include transurethral self-insertion, penetrating trauma, migration from adjacent organs, and iatrogenic introduction. A large case series by Eckford et al. [4] reported that approximately 40% of transurethral cases are associated with sexual gratification, often requiring psychological evaluation for conditions like polyembolokoilamania [5]. Transvesical cases, such as Case 3, are typically iatrogenic or fistula-related.
Clinical presentations vary widely, from dysuria and haematuria to asymptomatic cases, with some objects undetected for years. Diagnosis relies on a detailed history, including sexual practices and prior surgeries, alongside imaging modalities such as X-ray, ultrasonography, CT, or MRI. Cystoscopy is both diagnostic and therapeutic, enabling endoscopic removal in most cases using graspers, baskets, or cutting loops [6-8]. Organic foreign bodies, such as wood (Case 2), are often radiolucent, necessitating MRI or open exploration for diagnosis and management [9].
Endoscopic removal is the treatment of first choice because it is minimally invasive. Large or deeply seated foreign bodies, however, may need open surgery, e.g., laparotomy or suprapubic cystostomy, as in Case 3. Organic foreign bodies have more associated complications, e.g., fistulae and chronic inflammation, because they can cause a greater inflammatory response [10]. In Case 3, undissolved mesalamine tablets ("ghost tablets") were found in the bladder, possibly secondary to rapid transit through the gastrointestinal tract and active inflammation of Crohn's disease, which hindered tablet dissolution. The migration of undissolved mesalamine tablets into the bladder via an enterovesical fistula is an exceedingly rare complication of Crohn's disease. It shows the profound and sometimes unexpected sequelae of uncontrolled intestinal inflammation and fistula formation [11,12].
The present case series adds to the growing but limited body of literature on urological foreign bodies by encompassing diverse aetiologies, ranging from polyembolokoilamania-driven self-insertion to trauma and iatrogenic fistulisation. Bansal et al. (2016) presented the most extensive Indian series, comprising 49 cases, with a primary focus on retrieval outcomes in both self-inserted and iatrogenic cases (Table 2) [1]. Eckford et al. (1992) reported a five-year retrospective review emphasising the predominance of sexual gratification as a motive, reinforcing the need for psychiatric evaluation [4]. Our inclusion of polyembolokoilamania aligns with insights from Unruh et al. (2012), who emphasised psychiatric underpinnings and management strategies [5]. In contrast, Jang et al. (2012) highlighted the diagnostic challenge of radiolucent organic foreign bodies, a challenge echoed in our Case 2 [10]. Unlike prior studies that often focused on one mechanism of foreign body introduction, our series uniquely integrates three distinct mechanisms - self-insertion, penetrating trauma, and enterovesical fistula due to Crohn’s disease - thereby demonstrating the utility of a multidisciplinary diagnostic and therapeutic framework involving urology, radiology, gastroenterology, and psychiatry. This breadth enhances clinical awareness and supports individualised, aetiology-specific management strategies.
The primary limitations of this study are its inherent nature as a small, single-centre case series. It limits statistical power and generalisability, and the relatively short six-month follow-up period may be insufficient to detect late recurrences or long-term psychiatric or gastrointestinal sequelae. The healthcare burden, including the costs of advanced imaging and surgery, is notable, particularly in resource-constrained settings. Future research should prioritise standardised diagnostic algorithms, preventive strategies such as patient education on safe sexual practices, and technological advancements to enhance minimally invasive retrieval. Cross-disciplinary learning from fields like gastroenterology could further inform management strategies.
Conclusions
This series of cases illustrates the varied aetiologies of foreign bodies in urology, from self-insertion and trauma to iatrogenic origins. A favourable prognosis is contingent upon early identification. It requires a high index of clinical suspicion, a thorough and sensitive history, appropriate utilisation of imaging (CT, MRI, or ultrasound), and often diagnostic cystoscopy. It can be followed by a prompt aetiology-specific intervention, whether endoscopic or open surgical. Clinicians should recognise that urological foreign bodies, though uncommon, can present with varied and often nonspecific symptoms. A high index of suspicion, careful history-taking, and appropriate imaging are essential for timely diagnosis. Management should be individualised, ranging from endoscopic retrieval to open surgery when necessary, with multidisciplinary support where indicated. Early recognition and tailored treatment are key to preventing complications and ensuring good patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Foreign bodies in the urinary bladder and their management: a single-centre experience from North India Int Neurourol J Bansal A Yadav P Kumar M Sankhwar S Purkait B Jhanwar A Singh S 2602692020162770601010.5213/inj.1632524.262PMC 5083828 · doi ↗ · pubmed ↗
- 2Foreign body in the male urinary bladder: a case report Cureus Venkataramani S Ghazi NM Kazmi FH Khan I 16202410.7759/cureus.54592 PMC 1095824038523921 · doi ↗ · pubmed ↗
- 3Rare foreign body in bladder: a case report Medicine (Baltimore) Li Y Gao Y Chen X Jiang S 97201810.1097/MD.0000000000010519 PMC 594451329703021 · doi ↗ · pubmed ↗
- 4Intravesical foreign bodies: five-year review Br J Urol Eckford SD Persad RA Brewster SF Gingell JC 4145691992 http://10.1111/j.1464-410x.1992.tb 15456.x 173725210.1111/j.1464-410x.1992.tb 15456.x · doi ↗ · pubmed ↗
- 5Insertion of foreign bodies (polyembolokoilamania): underpinnings and management strategies Prim Care Companion CNS Disord Unruh BT Nejad SH Stern TW Stern TA 1114201210.4088/PCC.11f 01192 PMC 335756522690353 · doi ↗ · pubmed ↗
- 6Intravesical foreign bodies: review and current management strategies Urol J Rafique M 22323152008 https://journals.sbmu.ac.ir/urolj/index.php/uj/article/view/28/2719101894 · pubmed ↗
- 7The time-less urologic question, “Now why would you do that?” A case series and literature review of self-inserted urethral foreign bodies J Clin Urol Boyle A Martinez DR Mennie PA Rafiei A Carrion R 16516972013
- 8Urethral foreign bodies: clinical presentation and management Urology Palmer CJ Houlihan M Psutka SP Ellis KA Vidal P Hollowell CM 2572609720162726118210.1016/j.urology.2016.05.045 · doi ↗ · pubmed ↗