Cocaine- and Levamisole-Induced Vasculitis (CLIV)
Zahra Vaezi, Afshin Amini

TL;DR
This paper reviews cases of a rare vasculitis caused by cocaine and levamisole, focusing on symptoms, diagnosis, and treatment.
Contribution
A systematic review of CLIV cases from 2015-2024, clarifying clinical features and management strategies.
Findings
CLIV commonly presents with skin, kidney, and lung involvement.
Early diagnosis and stopping drug exposure improve prognosis.
Treatment includes corticosteroids and immunosuppressants in severe cases.
Abstract
Cocaine- and levamisole-induced vasculitis (CLIV) is a distinct form of drug-induced vasculitis characterized by dual antineutrophil cytoplasmic antibody (ANCA) positivity, rapidly progressive glomerulonephritis (RPGN), and diffuse alveolar hemorrhage (DAH). This systematic review synthesizes data from case reports, case series, and reviews published between 2015 and 2024 to clarify clinical presentations, diagnostic approaches, and management strategies. A comprehensive search of PubMed and Google Scholar using terms such as “levamisole-induced vasculitis,” “cocaine-associated vasculitis,” “dual ANCA vasculitis,” “RPGN,” and “DAH” identified 312 records. After removing 84 duplicates, 228 records were screened, 52 were assessed for eligibility, and 18 were included in the final analysis. Most patients presented with cutaneous, renal, and pulmonary involvement. Diagnostic tools included…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
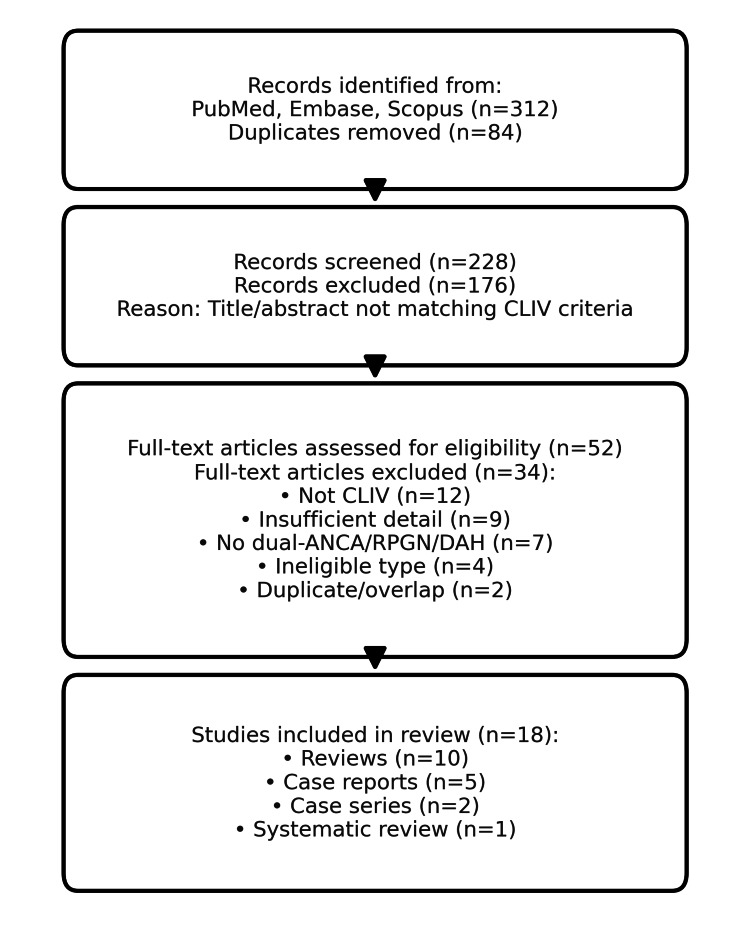 Figure 1
Figure 1| Author(s) | Year | Study type | Organ involvement | ANCA status |
| Yaseen et al. [ | 2022 | Review | Systemic | Dual ANCA+ |
| Iorio et al. [ | 2024 | Review | Renal, pulmonary | Dual ANCA+ |
| Marquez et al. [ | 2017 | Review | Skin, renal | Dual ANCA+ |
| Berman et al. [ | 2016 | Review | Skin | Variable |
| Ruffer et al. [ | 2023 | Review | Systemic | Dual ANCA+ |
| Misra et al. [ | 2021 | Review | Renal | MPO/PR3+ |
| Younger [ | 2021 | Review | CNS | Not reported |
| Puac-Polanco et al. [ | 2024 | Review | CNS | Not reported |
| Underner et al. [ | 2020 | Review | Pulmonary | Variable |
| Grau [ | 2015 | Review | Systemic | Dual ANCA+ |
| Subesinghe et al. [ | 2018 | Case series | Renal, pulmonary | Dual ANCA+ |
| Roberts and Chévez-Barrios [ | 2015 | Case report | Skin | Dual ANCA+ |
| Bucur et al. [ | 2023 | Systematic review | Renal, pulmonary | Dual ANCA+ |
| Lötscher et al. [ | 2019 | Case review | Renal | Dual ANCA+ |
| Patnaik et al. [ | 2015 | Case report | Skin | Dual ANCA+ |
| Kunzler et al. [ | 2018 | Case report | Skin | ANCA- |
| Mudoni et al. [ | 2018 | Case report | Renal, muscle | Not reported |
| Jin et al. [ | 2018 | Review | Renal, pulmonary | Dual ANCA+ |
| Author(s) | Diagnostic tools |
| Yaseen et al. [ | ANCA, biopsy |
| Iorio et al. [ | ANCA, imaging |
| Marquez et al. [ | ANCA, biopsy |
| Berman et al. [ | Biopsy |
| Ruffer et al. [ | ANCA, imaging |
| Misra et al. [ | ANCA |
| Younger [ | Imaging |
| Puac-Polanco et al. [ | Imaging |
| Underner et al. [ | Imaging |
| Grau [ | ANCA |
| Subesinghe et al. [ | ANCA, biopsy |
| Roberts and Chévez-Barrios [ | Biopsy |
| Bucur et al. [ | ANCA, imaging |
| Lötscher et al. [ | ANCA, biopsy |
| Patnaik et al. [ | ANCA |
| Kunzler et al. [ | Biopsy |
| Mudoni et al. [ | Labs, imaging |
| Jin et al. [ | ANCA, biopsy |
| Author(s) | Treatment | Outcome |
| Yaseen et al. [ | Immunosuppressants | Improved |
| Iorio et al. [ | Steroids, rituximab | Improved |
| Marquez et al. [ | Steroids | Improved |
| Berman et al. [ | Steroids | Improved |
| Ruffer et al. [ | Steroids, rituximab | Improved |
| Misra et al. [ | Steroids | Improved |
| Younger [ | Steroids | Improved |
| Puac-Polanco et al. [ | None specified | Not specified |
| Underner et al. [ | Steroids | Improved |
| Grau [ | Steroids | Improved |
| Subesinghe et al. [ | Steroids, plasmapheresis | Improved |
| Roberts and Chévez-Barrios [ | Steroids | Improved |
| Bucur et al. [ | Steroids, plasmapheresis | Improved |
| Lötscher et al. [ | Steroids | Improved |
| Patnaik et al. [ | Steroids | Improved |
| Kunzler et al. [ | Steroids | Improved |
| Mudoni et al. [ | IV fluids, supportive | Recovered |
| Jin et al. [ | Steroids, rituximab | Improved |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Pain Mechanisms and Treatments · Takotsubo Cardiomyopathy and Associated Phenomena
Introduction and background
Drug-induced vasculitis (DIV) is a rare but significant subtype of vasculitis, typically associated with small-vessel involvement and triggered by various pharmacologic or illicit substances [1]. Among these, levamisole-adulterated cocaine has emerged as a key contributor to DIV, leading to a condition now widely recognized as cocaine- and levamisole-induced vasculitis (CLIV) [2,3]. Levamisole, once used as an antihelminthic agent and immunomodulator, is commonly added to cocaine to increase bulk and enhance stimulant effects [2,4]. However, its immunologic side effects include the development of antineutrophil cytoplasmic antibody (ANCA)-positive vasculitis, leukocytoclastic vasculitis, and thrombotic vasculopathy [5-7]. The co-administration of cocaine and levamisole is linked to endothelial injury, neutrophil activation, and immune complex deposition-pathogenic mechanisms shared with primary ANCA-associated vasculitis (AAV) [6,8]. CLIV has been increasingly reported over the past decade, with most affected patients presenting with painful purpura, skin necrosis, or retiform purpura, commonly involving the ears, face, and extremities [9,10]. Systemic manifestations may include pulmonary hemorrhage, rapidly progressive glomerulonephritis (RPGN), and rare central nervous system (CNS) involvement [11-13]. The overlap in clinical features between CLIV and idiopathic AAV often results in diagnostic delays and mismanagement [14-16]. Despite the growing body of literature, awareness of CLIV remains suboptimal. Many patients are initially treated for primary vasculitis without adequate history-taking or toxicology screening [5,17]. A better understanding of the epidemiology, pathogenesis, and treatment of CLIV is essential to guide clinicians in early diagnosis and appropriate management [2,18]. This review synthesizes data from published case reports, series, and reviews from 2015 to 2024 to provide a comprehensive overview of CLIV, with particular attention to its clinical spectrum, diagnostic markers, treatment approaches, and outcomes.
Review
We conducted a systematic search of PubMed/MEDLINE, Embase, Scopus, and CENTRAL from January 1, 2015, through July 31, 2024: PubMed (final strategy): ((levamisole[Title/Abstract] OR levamisole-adulterated[Title/Abstract]) AND cocaine[Title/Abstract]) AND (vasculitis[Title/Abstract] OR vasculopathy[Title/Abstract] OR ANCA[Title/Abstract]) with filters: Humans; English; 2015-2024. Database-specific controlled vocabulary and syntax were used for Embase (Emtree) and Scopus; full strings, run dates, and hit counts are in Supplemental material 1. We also screened the reference lists of the included reports. CENTRAL returned no eligible randomized trials. The inclusion criteria include primary reports of cocaine- and/or levamisole-associated vasculitis with dual ANCA, RPGN, and/or diffuse alveolar hemorrhage (DAH) (case reports/series/cohorts). The exclusion criteria include non-CLIV vasculitides, insufficient clinical detail, ineligible article type, and duplicates/overlaps (see the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) [19] flow diagram in Figure 1 and Supplemental materials 1, 2).
PRISMA 2020 flow diagram of study selection.CLIV: cocaine- and levamisole-induced vasculitis; ANCA: antineutrophil cytoplasmic antibody; RPGN: rapidly progressive glomerulonephritis; DAH: diffuse alveolar hemorrhage; PRISMA: Preferred Reporting Items for Systematic reviews and Meta-Analyses
Two reviewers screened the titles/abstracts; one reviewer performed full-text extraction with senior adjudication for uncertainties. We extracted demographics, exposure confirmation (toxicology vs. self-report), organ involvement, ANCA serology (MPO, PR3), biopsy type/pathology, imaging, treatment, outcomes, follow-up, and abstinence/relapse. Risk of bias (RoB) [20] was assessed with JBI [21] checklists for case reports and case series; ROBINS-I was planned for any non-randomized comparative designs. Certainty of evidence was appraised with GRADE [22]. RoB and GRADE summaries appear in Supplemental material 3. Primary outcomes include (1) renal remission: ≥50% reduction in serum creatinine from peak or dialysis independence by 4-12 weeks; (2) pulmonary remission: cessation of DAH and oxygen independence; and (3) cutaneous response: re-epithelialization or resolution of retiform purpura/necrosis by clinical assessment. The secondary outcomes include relapse (any recurrence after initial response), need for plasmapheresis, ICU admission, and adverse events. Abstinence status was recorded when reported (toxicology-confirmed vs. patient-reported). Given the heterogeneous designs and outcomes and sparse comparative data, we did not perform quantitative pooling. We present a structured narrative synthesis of primary studies and a separate narrative of secondary reviews. Where outcomes were variably defined or missing, we report ranges and qualitatively explore sources of heterogeneity (study design, exposure confirmation). Data extraction included demographics, organ involvement, ANCA status, diagnostic methods, treatment, and outcomes. RoB was assessed qualitatively; case reports and small series had inherent selection bias, while reviews varied in search rigor. Eighteen studies met the inclusion criteria (Table 1).
Reviews such as Yaseen et al. [1] and Iorio et al. [2] provided overviews of systemic, renal, and pulmonary manifestations, reinforcing the high prevalence of dual ANCA positivity. Case reports, including Patnaik et al. [15] and Kunzler et al. [16], illustrated severe cutaneous necrosis and variable ANCA patterns. Case series, like Subesinghe et al. [11], documented both renal and pulmonary diseases with high relapse rates in those continuing cocaine use. The largest systematic review (Bucur et al. [13]) pooled over 100 patients and confirmed the skin and kidney as the most frequently involved organs. Treatment regimens were heterogeneous but most commonly initiated with corticosteroids, often escalated to rituximab or cyclophosphamide for severe or refractory disease. Plasmapheresis was used in fulminant cases, particularly with DAH or RPGN. Outcomes were favorable in most patients achieving drug cessation, while ongoing cocaine use was strongly linked to relapse. RoB analysis indicated that most evidence came from low-level observational reports, with frequent underreporting of drug cessation status and inconsistent ANCA testing. Nevertheless, recurrent findings across multiple studies strengthened the reliability of clinical patterns described. Eighteen studies were included after screening (see Figure 1 for PRISMA), comprising narrative reviews [1-5,7-10,18], a systematic review [13], two case series [11], and multiple single-patient case reports highlighting sentinel presentations [12,15-17]. Collectively, these sources describe a consistent phenotype of cocaine- and/or levamisole-associated vasculitis with prominent cutaneous, renal, and pulmonary involvement. Cutaneous disease-often retiform purpura or necrosis involving the ears and extremities-was repeatedly described across reviews and reports [2-4,12,15,16]. Renal involvement commonly manifested as RPGN, typically crescentic on biopsy when performed [11,13,14,18]. Pulmonary disease included DAH or alveolar infiltrates on imaging in severe cases [2,9,11,18]. Several sources also noted hematologic toxicity associated with levamisole exposure (e.g., neutropenia), which may coexist with vasculitic features [2-5].
Dual ANCA profile and diagnostics
A defining feature across the literature is dual ANCA positivity with both MPO-ANCA and PR3-ANCA detected in a substantial subset of cases, a pattern that should raise suspicion for levamisole adulteration when present alongside relevant exposure history [1-3,5,10,13,14,18]. Diagnostic confirmation varied: while some reports included comprehensive serologies, kidney or skin biopsy, and toxicology testing, others relied on clinical assessment and self-reported drug use, underscoring variability in case ascertainment [1-3,11-14,18]. Table 2 summarizes commonly used diagnostic modalities (ANCA testing, biopsy, and targeted imaging).
Yaseen et al. [1] and Iorio et al. [2] synthesize the broader landscape of DIV and delineate the CLIV spectrum, emphasizing dual ANCA patterns and multiorgan involvement. Marquez et al. [3] and Berman et al. [4] detail cutaneous necrosis and classic auricular involvement. Ruffer et al. [5] discuss systemic features and reinforce the importance of exposure history. Misra et al. [6] focus on immunopathologic mechanisms relevant to AAV. Younger [7] and Puac-Polanco et al. [8] address neurologic/CNS and imaging considerations, respectively, while Underner et al. [9] highlight pulmonary manifestations. Grau [10] provides an earlier review framing dual ANCA as a diagnostic clue. Subesinghe et al. [11] present a case series with renal and pulmonary disease and note relapse risk with continued cocaine use. Roberts and Chévez-Barrios [12] describe a prototypical cutaneous case. Bucur et al. [13] offer a systematic review synthesizing organ involvement patterns, and Lötscher et al. [14] concentrate on renal disease. Patnaik et al. [15] and Kunzler et al. [16] report severe skin presentations (including ANCA-negative variants), Mudoni et al. [17] expand the spectrum to myopathic involvement, and Jin et al. [18] review renal-pulmonary overlap. Initial management frequently involved high-dose corticosteroids, with escalation to rituximab or cyclophosphamide in organ-threatening disease; plasmapheresis was used in fulminant RPGN/DAH [2,11,13,14,18]. Across reports, sustained abstinence from cocaine/levamisole was repeatedly linked to improved outcomes and lower relapse risk, whereas ongoing use correlated with recurrence [2,3,11,13]. Table 3 summarizes reported regimens and outcomes with source-level citations that favor immunosuppressive therapy in appropriately selected patients.
Given the heterogeneous designs and limited comparative data, we did not perform quantitative pooling and instead present a structured narrative synthesis. Consistent with Table 2, most studies incorporated ANCA serology (MPO and PR3), with biopsy (skin or kidney) when feasible to confirm small-vessel vasculitis or crescentic glomerulonephritis (GN); imaging (e.g., chest radiography/CT) supported DAH or pulmonary involvement when suspected [1-3,9-12,14,18]. Urine toxicology and explicit documentation of exposure were variably reported, affecting case certainty in several reports [2,3,11,13].
RoB analysis
The majority of included studies were case reports and small case series, which inherently carry a high risk of selection and publication bias, as they often highlight unusual or severe presentations while underreporting milder or self-limiting cases. Several reviews included in this analysis lacked explicit search strategies or inclusion criteria, increasing the likelihood of selection bias. Across studies, there was substantial heterogeneity in diagnostic confirmation-while some patients underwent comprehensive ANCA testing (both MPO and PR3), others were diagnosed solely on clinical grounds without confirmatory laboratory data, introducing potential misclassification bias. Reporting bias was common, with incomplete documentation of treatment regimens, follow-up duration, and patient outcomes. Moreover, drug cessation status-a key determinant of prognosis-was inconsistently reported, limiting interpretation of long-term outcomes. No included study was a randomized controlled trial; thus, the certainty of evidence regarding treatment efficacy remains low to very low according to the GRADE criteria. Despite these limitations, the recurrence of consistent clinical patterns-particularly dual ANCA positivity with concurrent renal and pulmonary involvement-across diverse study designs and settings supports the validity of the observed associations.
Discussion
CLIV remains underrecognized, despite its rising prevalence due to widespread cocaine adulteration. This systematic review reinforces the clinical importance of recognizing CLIV in patients presenting with dual ANCA positivity [2,3,5], especially when accompanied by RPGN and DAH [13,14]. The pathophysiology of CLIV is multifactorial. Levamisole, an immunomodulatory agent [2,3,18], induces vasculitis through neutrophil activation, NETosis, and autoantibody production [6], often resulting in dual ANCA (MPO and PR3) positivity. Cocaine itself can contribute to endothelial injury and promote autoimmunity. The overlap of these mechanisms explains the aggressive nature of CLIV and its rapid progression to renal and pulmonary involvement. Clinically, CLIV mimics idiopathic AAV but differs in patient demographics and exposure history. Young to middle-aged adults with a history of substance use are commonly affected. Cutaneous manifestations such as retiform purpura [12,15,16] and skin necrosis, especially involving the ears and extremities, are frequently observed. Renal biopsy often reveals crescentic GN [13,14], while lung imaging may show diffuse alveolar infiltrates [9] due to hemorrhage. Diagnostic workup should include detailed substance use history, ANCA serologies, urine drug screen [2,3], and confirmatory biopsy where feasible. The presence of both MPO-ANCA and PR3-ANCA is highly suggestive of levamisole involvement. Management hinges on cessation of cocaine/levamisole exposure and immunosuppression. Steroids remain first-line, while severe cases may require rituximab, cyclophosphamide, and plasmapheresis [13,14]. Supportive care, including dialysis or mechanical ventilation, is essential in organ-threatening disease. Relapse is common in patients who continue cocaine use. Long-term outcomes depend on sustained abstinence, emphasizing the need for addiction counseling [2,3].
Conclusions
CLIV is a serious but potentially reversible vasculitis syndrome that requires prompt recognition and intervention. Early identification in cocaine users with suggestive clinical features-particularly dual ANCA positivity, RPGN, and DAH-is critical to preventing irreversible organ damage. Successful management hinges on both targeted immunosuppression and sustained cessation of cocaine/levamisole use. Multidisciplinary care involving nephrology, rheumatology, pulmonology, and addiction services is recommended to optimize patient outcomes. Long-term follow-up is essential to monitor for relapses and address the psychosocial components of substance use, which remain integral to preventing recurrence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A spotlight on drug-induced vasculitis Curr Rheumatol Rep Yaseen K Nevares A Tamaki H 3233362420223612963110.1007/s 11926-022-01088-0 · doi ↗ · pubmed ↗
- 2Cocaine- and levamisole-induced vasculitis: defining the spectrum of autoimmune manifestations J Clin Med Iorio L Davanzo F Cazzador D 51161320243927432810.3390/jcm 13175116 PMC 11396482 · doi ↗ · pubmed ↗
- 3Cocaine-levamisole-induced vasculitis/vasculopathy syndrome Curr Rheumatol Rep Marquez J Aguirre L Muñoz C Echeverri A Restrepo M Pinto LF 361920172861233210.1007/s 11926-017-0653-9 · doi ↗ · pubmed ↗
- 4Cocaine-induced vasculitis Rambam Maimonides Med J Berman M Paran D Elkayam O 07201610.5041/RMMJ.10263 PMC 510101027824551 · doi ↗ · pubmed ↗
- 5Cocaine-induced vasculitis and mimics of vasculitis (Article in German)Z Rheumatol Ruffer N Krusche M Holl-Ulrich K Kötter I Lötscher F 6066148220233561266010.1007/s 00393-022-01217-1PMC 10495486 · doi ↗ · pubmed ↗
- 6Mechanisms of thrombosis in ANCA-associated vasculitis Clin Rheumatol Misra DP Thomas KN Gasparyan AY Zimba O 480748154020213410949110.1007/s 10067-021-05790-9PMC 8189705 · doi ↗ · pubmed ↗
- 7Cerebral vasculitis associated with drug abuse Curr Opin Rheumatol Younger DS 24333320213318624210.1097/BOR.0000000000000766 · doi ↗ · pubmed ↗
- 8Imaging of drug-related vasculopathy Neuroimaging Clin N Am Puac-Polanco P RoviraÀ Shah LM Wiggins RH Rivas Rodriguez F Torres C 1131283420243795169710.1016/j.nic.2023.07.003 · doi ↗ · pubmed ↗