Evaluation of Olfactory Function in Asymptomatic Children With Congenital Cytomegalovirus Infection
Chrysanthi-Eleni Loizou, Sofia Karagiannidou, Garyfallia Syridou, Vassiliki Papaevangelou

TL;DR
This study found no difference in smell function between asymptomatic children with congenital CMV and healthy children.
Contribution
First evaluation of olfactory function in asymptomatic congenital CMV-infected children.
Findings
No significant difference in olfactory function between cCMV and control groups.
Sub-analyses by age and COVID-19 history also showed no differences in smell function.
Results suggest asymptomatic cCMV does not affect olfactory function in children.
Abstract
Background and aim Congenital cytomegalovirus (cCMV) is the most prevalent congenital infection worldwide, associated with numerous long-term sequelae, even in infants asymptomatic at birth. However, data are lacking for asymptomatic-at-birth children, who account for the majority of cases. Thus, the aim of the study was to evaluate the olfactory function of asymptomatic cCMV-infected children and compare it to matched healthy controls using a validated odor Identification test. Methods A case-control study was conducted. Asymptomatic cCMV-infected children and healthy controls without cCMV history over the age of five were included. Cases and controls were matched at a 1:2 ratio for age and sex. Exclusion criteria included other conditions associated with transient or permanent olfactory dysfunction. A U-Sniff odor identification test (Kids Ident Test "U-Sniff"; Burghart Messtechnik…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
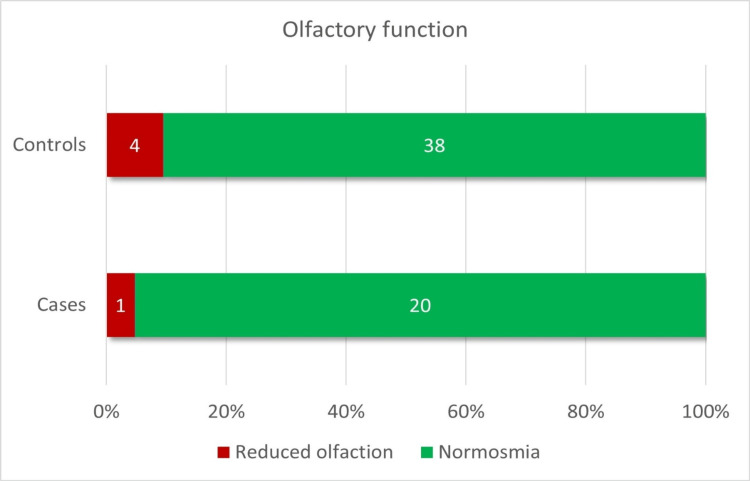 Figure 1
Figure 1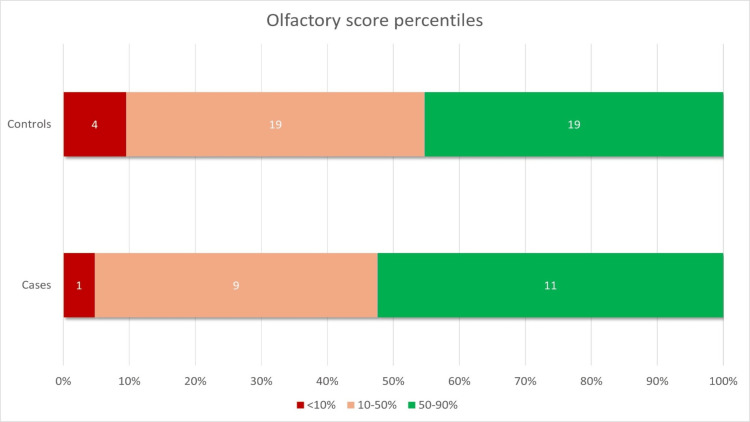 Figure 2
Figure 2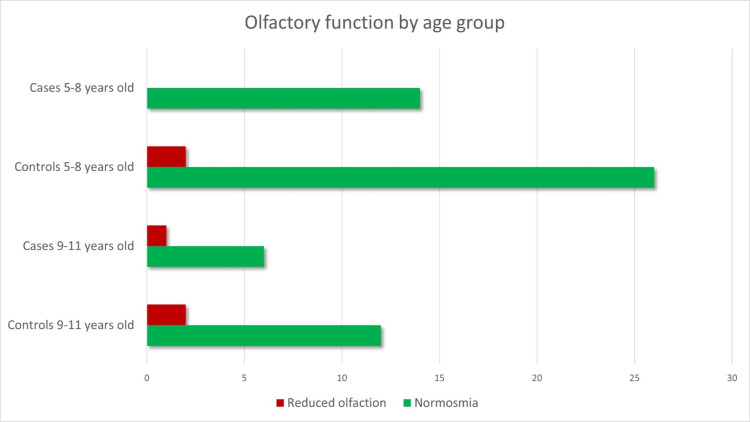 Figure 3
Figure 3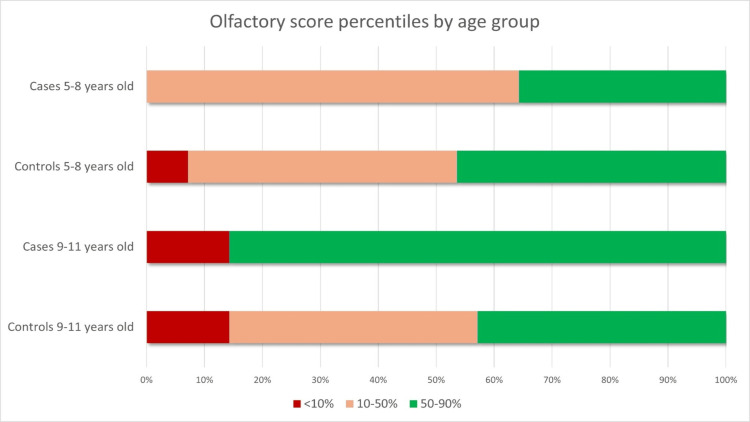 Figure 4
Figure 4| Parameters | Cases (n=21), n (%) | Controls (n=42), n (%) | p-value | Statistical numerical value | |
| Sex | Male | 8 (38.1%) | 16 (38.1%) | 1.000* | <0.0001 |
| Female | 13 (61.9%) | 26 (61.9%) | |||
| Gestational Age (weeks) | Median (25th-75th %) | 38+1 (37+5, 39+1) | Information not available | N/A | N/A |
| Trimester of infection | 1st | 9 (42.9%) | N/A | N/A | N/A |
| 2nd | 6 (28.6%) | ||||
| 3rd | 2 (9.5%) | ||||
| Unknown | 4 (19%) | ||||
| Age (years) | Median (25th-75th%) | 7 (6-9.5) | 7 (6-9.5) | 1.000^ | 441,000 |
| Age group | 5-8 years | 14 (66.7%) | 21 (66.7%) | 1.000* | <0.0001 |
| 9-11 years | 7 (33.3%) | 14 (33.3%) | |||
| Comorbidities | Yes | 1 (4.8%) | 23 (54.8%) | <0.0001* | 14,841 |
| No | 20 (95.2%) | 19 (45.2%) | |||
| Medication | Yes | 0 (0%) | 15 (35.7%) | 0.005* | 9,844 |
| No | 21 (100%) | 27 (64.3%) | |||
| COVID-19 infection history | Yes | 18 (85.7%) | 33 (78.6%) | 0.735** | 0.463 |
| No | 3 (14.3%) | 9 (21.4%) | |||
| LTI | Yes | 6 (28.6%) | N/A | N/A | N/A |
| No | 15 (71.4%) | ||||
| Type of LTI | No LTI | 15 (71.4%) | N/A | N/A | N/A |
| SNHL | 2 (9.5%) | ||||
| NDI | 3 (14.3%) | ||||
| SNHL and NDI | 1 (4.8%) |
| Department | Controls (n=42 ), n (%) | Reasons for visit |
| Pediatric Endocrinology | 22 (52.4%) | Hypothyroidism, early puberty, growth hormone deficiency, diabetes mellitus, congenital adrenal hyperplasia, obesity |
| General Pediatrics | 12 (28.6%) | Routine vaccination, routine blood workup; accompanying sibling that was brought for examination |
| Pediatric Infectious Disease | 4 (9.5%) | Parasitic – helminthic infections, recurrent urinary tract infections |
| Pediatric Lipid Disorders | 3 (7.1%) | Increased LDL, increased triglycerides |
| Pediatric Nephrology | 1 (2.4%) | Ureteral stenosis |
| Parameter | Cases (n=21), n (%) | Controls (n=42), n (%) | p-value | Statistical numerical value | |
| Reported sense of smell | Normal | 21 (100%) | 42 (100%) | N/C | N/C |
| Reduced | 0 (0%) | 0 (0%) | |||
| Olfactory result | Normosmia | 20 (95.2%) | 38 (90.5%) | 0.657* | 0.434 |
| Reduced olfaction | 1 (4.8%) | 4 (9.5%) | |||
| Olfactory score percentile | < 10th | 1 (4.8%) | 4 (9.5%) | 0.853* | 0.500 |
| 10th-50th | 9 (42.9%) | 19 (45.2%) | |||
| 50th-90th | 11 (52.4%) | 19 (45.2%) |
| Parameter | Cases (n=21), n (%) | Controls (n=42), n (%) | p-value | Statistical numerical value | ||
| Reported sense of smell | 5-8 years | Normal | 14 (100%) | 28 (100%) | N/C | N/C |
| Reduced | 0 (0%) | 0 (0%) | ||||
| 9-11 years | Normal | 7 (100%) | 14 (100%) | N/C | N/C | |
| Reduced | 0 (0%) | 0 (0%) | ||||
| Olfactory result | 5-8 years | Normosmia | 14 (100%) | 26 (92.9%) | 0.545* | 1,050 |
| Reduced olfaction | 0 (0%) | 2 (7.1%) | ||||
| 9-11 years | Normosmia | 6 (85.7%) | 12 (85.7%) | 1.000* | <0.0001 | |
| Reduced olfaction | 1 (14.3%) | 2 (14.3%) | ||||
| Olfactory score percentile | 5-8 years | < 10th | 0 (0%) | 2 (7.1%) | 0.472* | 1,431 |
| 10th-50th | 9 (64.3%) | 13 (46.4%) | ||||
| 50th-90th | 5 (35.7%) | 13 (46.4%) | ||||
| 9-11 years | < 10th | 1 (14.3%) | 2 (14.3%) | 0.088* | 4,475 | |
| 10th-50th | 0 (0%) | 6 (42.9%) | ||||
| 50th-90th | 6 (85.7%) | 6 (42.9%) |
| Parameter | Cases (n=21), n (%) | Controls (n=42), n (%) | p-value | Statistical numerical value | ||
| Reported sense of smell | SARS-CoV-2 infection history | Normal | 18 (100%) | 33 (100%) | N/C | N/C |
| Reduced | 0 (0%) | 0 (0%) | ||||
| No SARS-CoV-2 infection history | Normal | 3 (100%) | 9 (100%) | N/C | N/C | |
| Reduced | 0 (0%) | 0 (0%) | ||||
| Olfactory result | SARS-CoV-2 infection history | Normosmia | 17 (94.4%) | 29 (87.9%) | 0.645* | 0.568 |
| Reduced olfaction | 1 (5.6%) | 4 (12.1%) | ||||
| No SARS-CoV-2 infection history | Normosmia | 3 (100%) | 9 (100%) | N/C | N/C | |
| Reduced olfaction | 0 (0%) | 0 (0%) | ||||
| Olfactory score percentile | SARS-CoV-2 infection history | < 10th | 1 (5.6%) | 4 (12.1%) | 0.694* | 0.877 |
| 10th-50th | 6 (33.3%) | 13 (39.4%) | ||||
| 50th-90th | 11 (61.1%) | 16 (48.5%) | ||||
| No SARS-CoV-2 infection history | < 10th | 0 (0%) | 0 (0%) | 0.509* | 1,333 | |
| 10th-50th | 3 (100%) | 6 (66.7%) | ||||
| 50th-90th | 0 (0%) | 3 (33.3%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOlfactory and Sensory Function Studies · Cytomegalovirus and herpesvirus research · Herpesvirus Infections and Treatments
Introduction
Congenital cytomegalovirus (cCMV) is the most common viral congenital infection worldwide and a leading cause of non-genetic sensorineural hearing loss (SNHL) and neurodevelopmental impairment (NDI) [1-3]. Symptoms at birth are associated with long-term sequelae; however, 15-20% of children asymptomatic at birth (90%) may also present late-onset sequelae, mainly SNHL [2-4].
Cytomegalovirus (CMV) is a neurotropic virus, with its impact on the developing nervous system being well acknowledged after years of extensive research. Affected children may suffer from SNHL, epilepsy, motor deficits, and mild NDI [2-5]. However, the olfactory function of cCMV-infected children has not been adequately studied. Olfactory bulb malformations have been detected in both a pathology study of infected fetuses [6] and an animal model study [7]. Recently, a cranial MRI of a neonate with symptomatic cCMV infection revealed increased signal intensity in the central portion of the olfactory bulb in the T2 sequence [8], while another study reported reduced olfactory function in cCMV-infected children who are symptomatic at birth, using a house-made odor discrimination test [9].
The aim of this study is to provide data on the olfaction of asymptomatic cCMV-infected children, compared to children without known cCMV infection. To our knowledge, this is the first study attempting to assess the olfactory function of asymptomatic cCMV-infected children using a validated pediatric test.
Materials and methods
Study design
This was a single-center, prospective, case-control study (1:2) conducted in the Pediatric Infectious Disease Unit of University Hospital “Attikon”, Athens, Greece, between May 2023 and March 2024. The study was approved by the Scientific Council of University General Hospital "Attikon" (reference number: ΕΒ∆233/03-04-2023). The parents of both cases and controls provided written informed consent.
Study population
Cases consisted of asymptomatic cCMV-infected children born before January 2018, prospectively followed up in our center. The age criterion was required since the olfactory test used has been validated for children older than five years [10,11]. cCMV infection was confirmed by a positive urine polymerase chain reaction (PCR) for CMV during the first 21 days of life, while asymptomatic status was defined as lack of cCMV-related clinical symptoms at birth, as per European Congenital Cytomegalovirus Initiative guidelines [4]. Controls were recruited from the Outpatient Pediatric Clinic of our Department between June and October 2023, and they were matched with cases (1:2) for age and sex.
Exclusion criteria for both groups included a history of allergic rhinitis, chronic rhinosinusitis, herpetic meningoencephalitis, traumatic brain injury, and syndromic genetic disorders associated with anosmia. Moreover, both cases and controls were excluded if they presented with an acute respiratory tract infection on the day of the scheduled olfactory test.
Data collection
A data collection form was constructed for the purposes of the study. Demographic data (date of birth, sex) and medical history (including current medication regimen and previous SARS-CoV-2 infection) were noted.
Olfactory assessment
Assessment of olfactory function was conducted using a U-Sniff odor identification test [11] (Kids Ident Test "U-Sniff"; Burghart Messtechnik GmbH, Holm, Pinneberg, Germany). The test consists of 12 cards depicting four different items each and 12 markers, each containing a different mono-odorant. Cards and markers are uniquely matched to each other via a number (1-12) written at their top. The items depicted and odors contained include food, beverages, and plants. Testing was conducted following a standardized process, based on the manufacturer’s instructions. Children were presented with a card and were asked to inform the examiner in case they needed clarification of the items depicted. Then, the respective marker was placed 2 cm below their nostrils for two to three seconds. After its withdrawal, they were asked to point at the item on the card that best described the odor of the marker. The process was repeated 12 times. The sum of correct responses created the olfactory score of the child, which was interpreted as normosmia or reduced olfactory function according to the cut-off provided for the patient’s age; for patients aged 5-8 years, normosmia was defined as a score of 7 or higher, while for patients aged 9-11 years, normosmia was defined as a score of 9 or higher. Additionally, the patient’s olfactory function percentile for age (<10%, 10-50%, and 50-90%, respectively) was determined using age-adjusted charts.
Sample size
Currently, there is no data on the prevalence of olfactory dysfunction in healthy children or among asymptomatic cCMV-infected children. Moreover, the prevalence of olfactory dysfunction in symptomatic cCMV-infected children has been estimated using a house-made test with mono-odorants and binary mixtures that has not been validated for children [9]. Therefore, we used a sample of 21 asymptomatic cCMV children and 42 matched (1:2) controls, based on convenience sampling.
Statistical analysis
Statistical analysis was conducted using IBM SPSS Statistics for Windows version 25.0 (IBM Corp., Armonk, New York, United States). Descriptive statistics are presented as absolute (N) and relative frequencies (%) for categorical variables and as median (25th-75th percentile) for continuous, not-normally distributed variables. Univariate analysis between categorical variables was performed using the Chi-square test of independence (with Fisher’s exact method when one or more expected values were less than 5). The Mann-Whitney non-parametric test was used to make comparisons between categorical variables and continuous, not-normally distributed variables. Significance level was set at α=0.05. Bonferroni correction was applied to adjust for multiple comparisons.
Results
Overall, 51 cCMV-infected children were eligible for inclusion in our study. We were able to contact 41 parents (six parents could not be contacted since up-to-date contact information was not available, and four did not respond to multiple communication attempts). Of the 41 parents contacted, parents of two children refused participation due to follow-up at another hospital, parents of eight children reported they did not want their child to be tested as they did not present any cCMV-related LTI and they felt testing would be redundant, and 10 children could not be tested because of social reasons (residence outside of Athens and serious family problems unrelated to cCMV that rendered their visit at our hospital difficult). Thus, a total of 21 asymptomatic-at-birth cCMV-infected children were evaluated, leading to a response rate of 51.2%.
Of the total 21 participants, 61.9% were female, while the participants' median age was seven years (range, 5-11 years). The median gestational age of cCMV-infected children enrolled was 38+1 weeks (range, 37+5, 39+1 weeks). One of the children had a comorbidity unrelated to cCMV (increased levels of lipoprotein A), while none of the children were on any medications at the time of assessment. Six children (28.5%) had cCMV-related long-term sequelae; two had isolated SNHL, three had NDI requiring intervention, while one child presented with both conditions. For those children presenting with NDI requiring intervention, it was deemed by developmental medicine assessments that their ability to complete the olfactory test was not impacted. Additionally, 42 healthy controls were recruited. The characteristics of the study cohort can be found in Table 1.
**Table 1: Cohort characteristicsData have been presented as n (%) except for continuous not-normally distributed variables (gestational age, age), which are presented as median (25th-75th %).p-values were considered significant if <0.05 and are marked in bold (*chi-square test of independence, Fisher's exact test, ^Mann-Whitney non-parametric test)SNHL: sensorineural hearing loss; NDI: neurodevelopmental impairment; LTI: long-term impairment; N/A: not applicable
Statistically significant differences between cases and controls were noted in terms of comorbidities and medication regimen, which was expected since controls were recruited from an outpatient pediatric clinic. Reasons for visit of controls on the day of recruitment and associated comorbidities can be found in Table 2. Since no olfactory impairment was associated with these conditions, we considered our sample of healthy controls appropriate.
Parents of all cases and controls reported that their children had a normal sense of smell. According to the 10th percentile threshold of the U-Sniff test for normosmia, one patient in the cCMV group (4.8%) and four patients in the healthy control group (9.5%) presented with a reduced olfactory function (Figure 1). Interestingly, the child in the cCMV group with reduced olfactory function had no long-term sequelae. There were no differences in the olfactory function nor the olfactory score percentiles for age between cases and controls (p=0.657 and p=0.853, respectively) (Figure 1, Figure 2, Table 3).
Olfactory function results of the entire cohortData are represented as absolute (N) frequencies in the bars and relative (%) frequencies in the x-axis.Reduced olfaction is defined as an olfactory score below the 10th percentile for age.
Distribution of olfactory score percentiles in the entire cohortData are represented as absolute (N) frequencies in the bars and relative (%) frequencies in the x-axis.Reduced olfaction is defined as an olfactory score below the 10th percentile for age.
**Table 3: Olfactory assessment resultsData have been presented as absolute (n) and relative frequencies (%). p-value is considered significant if <0.05 (*Fisher's exact test).N/C: not compu
No differences were detected in a sub-analysis where participants were divided into two age groups, namely 5-8 and 9-11 years (Figure 3, Figure 4, and Table 4).
Olfactory function by age groupData are represented as absolute (N) frequencies in the x-axis.Reduced olfaction is defined as an olfactory score below the 10th percentile for age.
Olfactory score percentiles by age groupData are represented as relative (%) frequencies in the x-axis.Reduced olfaction is defined as an olfactory score below the 10th percentile for age.
**Table 4: Olfactory assessment results by age groupData has been represented as absolute (N) and relative frequencies (%). p-value is considered significant if <0.05 (*Fisher's exact test).N/C: not compu
Finally, we stratified results based on the history of previous SARS-CoV-2 infection to evaluate whether olfaction was affected by COVID-19, confounding our results. Most children, 18 cases (85.7%) and 33 controls (78.6%), reported a known history of SARS-CoV-2 infection. Importantly, all five children with a reduced olfactory function result reported a history of previous SARS-CoV-2 infection. However, the results of our study were not altered when cases and controls were compared based on their reported history of previous SARS-CoV-2 infection (Table 5).
**Table 5: Stratification of olfactory assessment results by reported SARS-CoV-2 infection historyData has been represented as absolute (N) and relative frequencies (%). p-value is considered significant if <0.05 (*Fisher's exact test).N/C: not compu
Discussion
cCMV infection is associated with multiple neurologic long-term sequelae, including cerebral palsy, epilepsy, SNHL, and NDI [2-4]. To date, only one study has attempted to evaluate olfactory function in cCMV-infected children [9]. The study used a house-made odor discrimination test to assess olfactory function in symptomatic cCMV children versus controls, demonstrating a significant difference between groups (73.5% of symptomatic cCMV versus 44.1% of controls with a threshold olfactory score <4, p=0.025). However, this test has not been validated for children, the cut-off value used for normosmia was arbitrarily set, and it is not commercially available. Moreover, the study did not include asymptomatic cCMV children.
Assessment of olfactory function is challenging, especially in young children whose attention span is short, linguistic and cognitive skills are not fully developed, and familiarity with odors is limited. Threshold and suprathreshold methods exist for olfactory assessment; suprathreshold methods (odor discrimination and odor identification tests) are used as screening methods, while more specialized tests, including threshold tests, are employed when reduced olfactory function is detected. Odor discrimination tests’ use is limited since no validated tests for children exist. Odor identification tests, which require the child to identify the odorant in a forced-choice manner from pictures or words presented to them, are more frequently used [12]. The U-Sniff Odor Identification Test is the only commercially available test that has been validated for children in 27 countries, including Greece [11,13]. This is the first study to report the use of a validated, standardized odor Identification test to evaluate olfactory function in asymptomatic cCMV-infected children.
Our study was conducted during the post-COVID-19 period, while it has been well established that SARS-CoV-2 can cause olfactory dysfunction [14]. Thus, we suspected that previous COVID-19 infection could be a confounder for olfactory performance. However, the results of this study were not altered when children previously affected by COVID-19 were compared to those with a negative history of a previous SARS-CoV-2 infection. Notably, we did not perform antibody tests to confirm a negative history of previous COVID-19 infection, although this study took place during a period where seropositivity rates among children in Greece were very high [15,16].
Our study has important limitations. First, this is a small study; therefore, differences between cases and controls could be detected in a larger study. Possible recruitment bias cannot be excluded, since a 51.2% response rate was achieved. Also, we cannot exclude that amongst our controls an undiagnosed asymptomatic child with cCMV infection was included, since cCMV screening at birth is not conducted in Greece. Although CMV serology is tested during pregnancy to detect primary maternal infection, the possibility of a non-primary maternal infection cannot be excluded. Additionally, our control group included children with comorbidities, which, even though they have not been associated with an olfactory dysfunction in the literature, their potential influence cannot be completely excluded. Furthermore, we did not perform serology testing to confirm the reported absence of exposure to SARS-CoV-2 infection. Finally, we did not collect data on passive smoking; therefore, such analyses were not conducted.
Conclusions
Olfactory dysfunction is an important sensory deprivation which has gained popularity in the post-COVID-19 era. In this small, exploratory study, which employed a validated, odor identification test for the first time, no statistically significant differences were detected between asymptomatic cCMV-infected children and healthy controls matched for age and sex. Importantly, this is the first report on the olfactory function of asymptomatic cCMV-infected children. While our data does not support routine olfactory assessment of asymptomatic cCMV-infected children, studies with larger samples are needed in order to confirm these preliminary findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Congenital cytomegalovirus infection burden and epidemiologic risk factors in countries with universal screening: a systematic review and meta-analysis JAMA Netw Open Ssentongo P Hehnly C Birungi P 04202110.1001/jamanetworkopen.2021.20736 PMC 838313834424308 · doi ↗ · pubmed ↗
- 2Newborn hearing screening--a silent revolution N Engl J Med Morton CC Nance WE 2151216435420061670775210.1056/NEJ Mra 050700 · doi ↗ · pubmed ↗
- 3New estimates of the prevalence of neurological and sensory sequelae and mortality associated with congenital cytomegalovirus infection Rev Med Virol Dollard SC Grosse SD Ross DS 3553631720071754205210.1002/rmv.544 · doi ↗ · pubmed ↗
- 4Consensus recommendation for prenatal, neonatal and postnatal management of congenital cytomegalovirus infection from the European congenital infection initiative (ECCI)Lancet Reg Health Eur Leruez-Ville M Chatzakis C Lilleri D 1008924020243859094010.1016/j.lanepe.2024.100892 PMC 10999471 · doi ↗ · pubmed ↗
- 5What are the neurodevelopmental outcomes of children with asymptomatic congenital cytomegalovirus infection at birth? A systematic literature review Rev Med Virol Smyrli A Raveendran V Walter S 034202410.1002/rmv.2555 PMC 1126242439031854 · doi ↗ · pubmed ↗
- 6Cytomegalovirus-induced brain malformations in fetuses J Neuropathol Exp Neurol Teissier N Fallet-Bianco C Delezoide AL 1431587320142442363910.1097/NEN.0000000000000038 · doi ↗ · pubmed ↗
- 7Congenital cytomegalovirus infection alters olfaction before hearing deterioration in mice J Neurosci Lazarini F Katsimpardi L Levivien S Wagner S Gressens P Teissier N Lledo PM 10424104373820183034118110.1523/JNEUROSCI.0740-18.2018 PMC 6596252 · doi ↗ · pubmed ↗
- 8In vivo magnetic resonance imaging evidence of olfactory bulbs changes in a newborn with congenital citomegalovirus: a case report Ital J Pediatr Bianchi A Coviello C Leonardi V 2274720213478493410.1186/s 13052-021-01170-w PMC 8594161 · doi ↗ · pubmed ↗