Pulmonary Pleomorphic Carcinoma With Mesenchymal-Epithelial Transition Factor (MET) Mutation: An Aggressive Entity
Yuta Takemura, Kazuki Fukumoto, Akinori Sasaki

TL;DR
This paper discusses a rare aggressive lung cancer case where genomic testing identified a MET mutation, but treatment was delayed, leading to death.
Contribution
Highlights the need for early genomic profiling in inconclusive lung cancer cases to enable timely targeted therapy.
Findings
Genomic profiling identified a MET exon 14 skipping mutation in a suspected NSCLC case.
The patient's death before treatment underscores the aggressive nature of pulmonary pleomorphic carcinoma.
Autopsy confirmed the diagnosis, emphasizing the importance of early molecular testing.
Abstract
Pulmonary pleomorphic carcinoma (PPC) is a rare, aggressive non-small cell lung cancer (NSCLC) subtype characterized by rapid progression and challenging diagnosis from a limited biopsy. These challenges delay treatment initiation. Comprehensive genomic panel profiling helps identify actionable driver mutations, such as mesenchymal-epithelial transition factor (MET) exon 14 skipping mutations, enabling molecular targeted therapy planning. We present a case of an older female patient with suspected NSCLC and rapid clinical deterioration, where biopsy did not confirm the specific subtype. Genotype testing identified a MET exon 14 skipping mutation. A MET inhibitor treatment was planned; however, the patient died before treatment began. Postmortem autopsy confirmed the diagnosis of PPC. This case highlights the importance of early comprehensive genomic profiling in suspected NSCLC with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
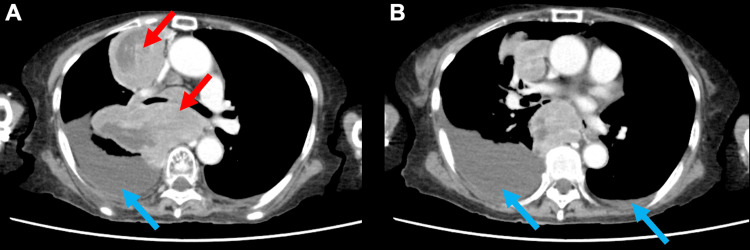 Figure 1
Figure 1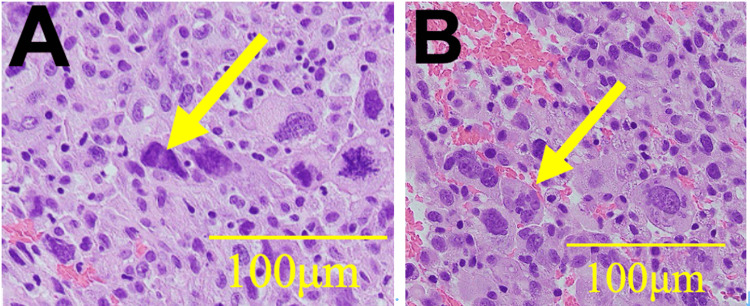 Figure 2
Figure 2| Tumor marker | Measured value | Normal range |
| ProGRP | 48.8 pg/mL | <81 pg/mL |
| NSE | 37 ng/mL | <16.3 ng/mL |
| SLX | 52.1 U/mL | <38 U/mL |
| CYFRA | 7.1 ng/mL | <3.5 ng/mL |
| IL-2R | 3,532 U/mL | 122-613 U/mL |
| Hospital day | Key clinical events and interventions |
| Day 1 | Admitted to the hospital. Contrast-enhanced CT reveals a large mediastinal tumor. EUS-FNB is performed to obtain a specimen. |
| Day 4 | Initial histopathology report of the EUS-FNB specimen suggests a malignant tumor. |
| Day 11 | Comprehensive genomic profiling identifies a MET exon 14 skipping mutation. |
| Day 20 | A large right pleural effusion and a collapsed IVC. |
| Day 21 | Quetiapine is initiated for terminal delirium. |
| Day 22 | The planned MET inhibitor (gumarontinib) arrives, but oral administration is not feasible due to the patient’s deteriorating condition. Dexamethasone is initiated. |
| Day 23 | Dexamethasone is discontinued, and a 0.5 mg fentanyl patch is applied for pain management. |
| Day 24 | The fentanyl patch is replaced with intravenous morphine. The decision is made to transition to CMO. |
| Day 25 | The patient died. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMetastasis and carcinoma case studies · Tracheal and airway disorders · Cancer Diagnosis and Treatment
Introduction
Lung cancer is the most common cancer type and the leading cause of cancer-related mortality worldwide [1]. Non-small cell lung cancer (NSCLC) is the most common lung cancer subtype, with 60%-70% diagnosed at advanced stage Ⅳ. Although various chemotherapy regimens exist for patients with advanced NSLC, prognosis remains poor, with a median survival of approximately 1.5 years [2]. However, a paradigm shift in NSCLC treatment occurred with the identification and targeted treatment of genomic oncogenic drivers such as epidermal growth factor receptor (EGFR), anaplastic lymphoma kinase (ALK), and mesenchymal-epithelial transition factor (MET) exon 14 skipping. Patients with NSCLC with driver gene mutations have better prognoses than those without [2]. Presently, targetable driver genes are identified in approximately 60% of lung adenocarcinoma cases in Western populations and up to 80% in Asian populations [3].
Adenocarcinoma is the most common NSCLC histological subtype, followed by squamous cell carcinoma [4]. Pulmonary pleomorphic carcinoma (PPC) is a rare NSCLC subtype, defined as a malignancy that contains at least 10% spindle or giant cell components, accounting for approximately 0.1% of all NSCLC cases [5]. PPC progresses rapidly and can deteriorate the patient’s condition before treatment can begin [6,7]. Treatable driver mutations such as EGFR, ALK, and MET exon 14 skipping have been detected in patients with PPC [6,8]. Therefore, patients with PPC have a poor prognosis; however, their prognosis may improve depending on the results of driver gene testing.
PPC can harbor actionable oncogenic driver gene mutations such as EGFR, ALK, B-Raf proto-oncogene, serine/threonine kinase (BRAF), Kirsten rat sarcoma viral oncogene homolog (KRAS), and MET exon 14 skipping. In this context, “driver mutations” are key genetic changes that fuel a tumor’s growth. The process of searching for these alterations is called “comprehensive genomic testing,” a laboratory analysis of a tumor’s DNA. This testing is essential because finding a specific driver mutation can guide treatment decisions, enabling the use of targeted therapies that are designed to selectively block the effects of that particular mutation.
Among these actionable mutations, MET exon 14 skipping is a key oncogenic driver found in approximately 3%-4% of NSCLC cases [9]. The MET proto-oncogene encodes a receptor tyrosine kinase, and aberrant activation via this exon 14 skipping mutation leads to downstream signaling that promotes tumor cell proliferation, survival, and invasion [10]. Potent MET tyrosine kinase inhibitors have been developed to counter this alteration. Gumarontinib, a selective MET inhibitor used in this case, was approved in Japan in 2024 for the treatment of advanced or recurrent NSCLC with MET exon 14 skipping, based on its demonstrated clinical efficacy [11]. The identification of such therapeutic targets is facilitated by comprehensive genomic panels such as the Oncomine™ Dx Target Test. This next-generation sequencing (NGS)-based companion diagnostic simultaneously analyzes both DNA and RNA from a single tumor sample to detect multiple biomarkers. For NSCLC, its panel is designed to identify critical mutations in genes such as EGFR, BRAF, and KRAS; fusions in ALK, proto-oncogene 1, receptor tyrosine kinase (ROS1), and rearranged during transfection (RET); and alterations such as MET exon 14 skipping, thereby enabling the selection of appropriate molecular targeted therapies [12].
This case report describes a patient whose PPC was confirmed postmortem, and the process of diagnosis and management particularities will be discussed.
Case presentation
An older female patient in her early 80s presented with fatigue and loss of appetite persisting for several months and was subsequently admitted to our hospital. She had no history of smoking and a medical history of poliomyelitis and cataracts. Prior to symptom onset, her Eastern Cooperative Oncology Group (ECOG) Performance Status (PS) deteriorated from 1 (fully ambulatory and able to carry on light work) to 4 (completely disabled and confined to bed) before admission [13]. Computed tomography (CT) revealed a large anterior mediastinal mass compressing the esophagus and bilateral pleural effusions (Figure 1). However, CT did not show significant metastases to the bone, adrenal glands, or liver. Furthermore, a brain magnetic resonance imaging (MRI) revealed no evidence of metastases. Tumor markers were elevated: pro-gastrin-releasing peptide (ProGRP), 48.8 pg/mL; neuron-specific enolase (NSE), 37 ng/mL; Sialyl-Lewis X (SLX), 52.1 U/mL; cytokeratin 19 fragment (CYFRA), 7.1 ng/mL; and interleukin-2 receptor (IL-2R), 3,532 U/mL (Table 1). Based on findings from the CT scan and tumor markers, small cell lung cancer, NSCLC, and malignant lymphoma were considered as differential diagnoses. Subsequently, an endoscopic ultrasound-guided fine-needle biopsy (EUS-FNB) of the mediastinal lesion was performed, using a 19-gauge needle to obtain adequate tissue for both histological and genomic analysis (Figure 2). Histopathological examination of the tumor biopsy sample indicated NSCLC, although the specific histological subtype could not be determined. Furthermore, an immunohistochemical panel was performed, but the results were non-contributory for definitive subtyping.
Initial chest CT image showing a bulky mediastinal tumor and bilateral pleural effusionsFigure 1A shows a bulky mediastinal tumor (red arrows) compressing the esophagus. Figure 1A and Figure 1B demonstrate bilateral pleural effusions, which are more predominant on the right side (blue arrows).CT: computed tomography
Histopathology of the tumor specimen obtained via endoscopic ultrasound-guided fine-needle biopsy of the mediastinal massFigure 2A and Figure 2B show different sites from the same tumor specimen. Histopathological examination revealed large nuclei (yellow arrows in Figure 2A) and multinucleated cells (yellow arrow in Figure 2B). A subset of tumor cells exhibited increased nuclear chromatin, irregular cytoplasmic morphology resembling squamous cell features, and eccentric nuclei. However, a definitive histological subtype could not be determined, and the findings were suggestive of non-small cell carcinoma.
Given the patient’s advanced stage and exceptionally rapid clinical decline, the immediate clinical priority was to identify a potential molecular target for therapy, rather than to pursue a more definitive histological classification via further invasive procedures. To identify potentially actionable genetic alterations, next-generation sequencing (Oncomine™ Dx Target Test) was performed and revealed a MET exon 14 skipping mutation. Based on the evidence of invasion into the esophagus (T4) and the presence of pleural effusion, the disease was classified as stage IV. Consequently, the initiation of treatment with the MET inhibitor gumarontinib was planned [8]. However, due to a severe loss of appetite and the onset of terminal delirium, oral administration of gumarontinib was not feasible. Thus, she succumbed to tumor progression on hospital day 25, before gumarontinib administration (Table 2). A postmortem pathological autopsy was subsequently performed, revealing an approximately 10 cm tumor in the right upper lung lobe. This postmortem histopathological evaluation revealed that the tumor predominantly consisted of spindle and giant cells, with poorly differentiated adenocarcinoma components in part. Based on these findings, the tumor was eventually diagnosed as PPC.
Discussion
This case of a large mediastinal tumor provided key insights into the diagnostic and therapeutic process. First, in a suspected case of NSCLC with an indeterminate histological subtype based on biopsy pathology, submission of a comprehensive cancer gene panel, while considering the possibility of rare malignancies such as PPC, enabled the successful identification of a MET exon 14 skipping mutation. Second, even without a definitive pathological diagnosis, the gene panel allowed the construction of a treatment plan, incorporating the potential use of a molecular targeted therapy.
PPC is typically diagnosed at a median age of approximately 66, and it demonstrates a higher prevalence in men (58%-76%), with a strong correlation to a history of smoking [14,15]. In addition, the lesions most frequently affect the upper lobes, with a predilection for the right lung [14]. In this case, the patient was an older female non-smoker, deviating from established epidemiological trends. The tumor progressed rapidly and was located in the right upper lobe, aligning with known clinical PPC features. In addition, histologically, PPC is defined by the presence of both epithelial and sarcomatoid components, including spindle and giant cells. The epithelial component of PPC may include adenocarcinoma, squamous cell carcinoma, or large cell carcinoma elements [16]. The sarcomatoid component consists of undifferentiated elements and is associated with a high degree of biological aggressiveness [17]. A definitive diagnosis typically requires comprehensive histopathological examination of resected specimens, as biopsy samples alone are generally insufficient for diagnosis, making early detection challenging [18]. In this case, histopathology revealed undifferentiated NSCLC characterized by prominent spindle and giant cell components. The strong presence of sarcomatoid features likely indicated a high tumor grade and contributed to the tumor’s aggressive clinical behavior.
PPC may harbor various oncogenic driver mutations, allowing for early development of molecular targeted treatment strategies, even before definitive histopathological diagnosis. PPC harbors various actionable oncogenic driver gene mutations, including KRAS (27%), EGFR (8%), and PIK3CA (7%). Among these, MET exon 14 skipping mutations are present in approximately 8% of PPC cases [8]. Although evidence remains limited to individual case reports, several have described marked clinical responses to MET inhibitors in patients with PPC harboring MET exon 14 skipping mutation [17]. Ongoing investigations are evaluating the therapeutic efficacy of MET-targeted agents in this molecular subset [19,20]. PPC is a rare and aggressive malignancy where definitive diagnosis from small biopsy samples is often challenging. However, since PPC can harbor actionable driver mutations, early comprehensive genomic profiling is critical. In this clinical context, identifying a targetable mutation by genomic profiling can be of immediate therapeutic importance as it directly guides the use of molecular targeted therapies. In this case, MET exon 14 skipping was identified via comprehensive genomic profiling before a definitive diagnosis was made. This early gene mutation identification enabled the planning of MET-targeted therapy. Notably, several case reports have described therapeutic responses, commonly referred to as the “Lazarus effect,” in patients with MET exon 14 skipping-positive NSCLC and poor PS following MET inhibitor treatment [21-23]. Although MET inhibitor therapy with gumarontinib was not initiated prior to the patient’s death in this case, previous reports support its potential for therapeutic benefit.
Finally, we acknowledge some limitations in this report. Our report focused solely on the identified MET exon 14 skipping mutation as the primary therapeutic target. The full data from the comprehensive genomic panel, including the status of potential co-mutations, which could influence prognosis or therapeutic response, were not available for this case report.
Conclusions
In conclusion, PPC is a rare, rapidly progressing malignancy with a poor prognosis, primarily owing to the challenges in achieving a definitive diagnosis. When a mediastinal mass demonstrates heterogeneous histological features on biopsy, making classification and diagnosis challenging, comprehensive genomic profiling should be considered. Early identification of actionable driver mutations through such profiling may enable the timely initiation of personalized therapy, including molecular targeted therapies, which is essential for improving patient outcomes. This case, therefore, underscores the need to consider advocating for standardized protocols that incorporate early comprehensive genomic profiling in patients with suspected high-grade or rapidly progressing NSCLC, even when histology is inconclusive. As recent studies have suggested, the timing of genomic profiling matters, and earlier testing in patients with lung cancer is associated with improved survival outcomes. Establishing such protocols could be a critical step in optimizing treatment pathways and ensuring that patients have the best possible chance to benefit from precision medicine.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J Clin Bray F Laversanne M Sung H Ferlay J Siegel RL Soerjomataram I Jemal A 2292637420243857275110.3322/caac.21834 · doi ↗ · pubmed ↗
- 2Evolving treatments and prognosis in stage IV non-small cell lung cancer: 20 years of progress of novel therapies Lung Cancer Satoh H Okuma Y Shinno Y 10845320220254002046610.1016/j.lungcan.2025.108453 · doi ↗ · pubmed ↗
- 3Targeted therapies for lung cancer patients with oncogenic driver molecular alterations J Clin Oncol Tan AC Tan DS 6116254020223498591610.1200/JCO.21.01626 · doi ↗ · pubmed ↗
- 4The 2015 World Health Organization classification of lung tumors: impact of genetic, clinical and radiologic advances since the 2004 classification J Thorac Oncol Travis WD Brambilla E Nicholson AG 124312601020152629100810.1097/JTO.0000000000000630 · doi ↗ · pubmed ↗
- 5Clinicopathological characteristics and prognosis of pulmonary pleomorphic carcinoma: a population-based retrospective study using SEER data J Thorac Dis Yin J Yang Y Ma K 426242731020183017487210.21037/jtd.2018.06.71PMC 6106015 · doi ↗ · pubmed ↗
- 6Pulmonary pleomorphic carcinoma: a clinicopathological study including EGFR mutation analysis J Thorac Oncol Kaira K Horie Y Ayabe E 460465520102010742110.1097/JTO.0b 013e 3181 ce 3e 3c · doi ↗ · pubmed ↗
- 7Pleomorphic carcinoma of the lung: a surgical outcome J Thorac Cardiovasc Surg Yuki T Sakuma T Ohbayashi C Yoshimura M Tsubota N Okita Y Okada M 39940413420071766277910.1016/j.jtcvs.2007.04.018 · doi ↗ · pubmed ↗
- 8Comprehensive molecular profiling of pulmonary pleomorphic carcinoma NPJ Precis Oncol Nagano M Kohsaka S Hayashi T 57520213415860110.1038/s 41698-021-00201-3PMC 8219709 · doi ↗ · pubmed ↗