Prognostic value of neutrophil to lymphocyte ratio in patients with esophagus cancer receiving neoadjuvant therapy: a systematic review and meta-analysis
Longwei Ma, Jiaxing He, Ping Li, Long Ma, He Wang, Yanchao Deng

TL;DR
This study finds that a higher neutrophil to lymphocyte ratio is linked to worse outcomes in esophageal cancer patients receiving neoadjuvant therapy.
Contribution
The study provides a meta-analysis confirming NLR as a prognostic biomarker for esophageal cancer patients undergoing neoadjuvant therapy.
Findings
Higher NLR is associated with worse overall and recurrence-free survival in esophageal cancer patients.
Elevated NLR is linked to lower rates of pathological complete response in these patients.
Subgroup analyses confirm the robustness of NLR as a prognostic marker across different treatment types.
Abstract
Growing research reveals a relation of the neutrophil-to-lymphocyte ratio (NLR) to clinical outcomes of the esophageal cancer (EC) population undergoing neoadjuvant therapy. However, current findings remain inconclusive and somewhat controversial. PubMed, Embase, Web of Science, and the Cochrane Library were thoroughly retrieved until April 22, 2025 to collect studies on the link of NLR to prognosis among the EC population following neoadjuvant therapy. Eligible studies were selected as per predefined eligibility criteria. The primary outcomes encompassed overall survival (OS), recurrence-free survival (RFS), and pathological complete response (pCR). Hazard ratios (HRs) and corresponding 95% confidence intervals (CIs) were pooled for prognostic significance assessment along with subgroup analyses. The evidence was graded via the GRADE method. 11 cohort studies involving 2,220 patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
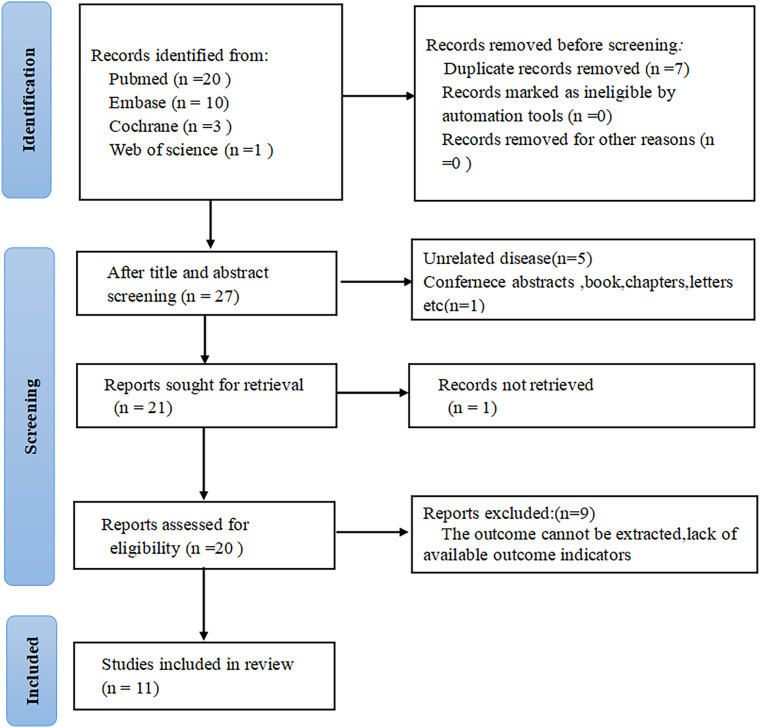 Figure 1
Figure 1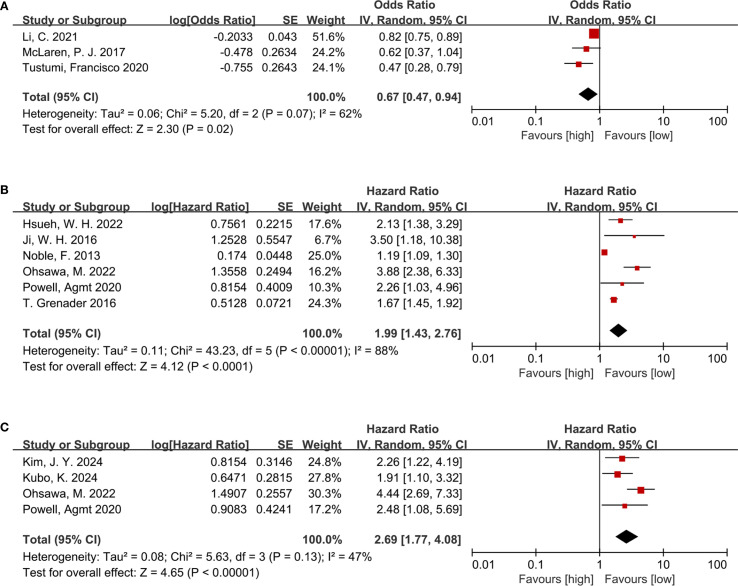 Figure 2
Figure 2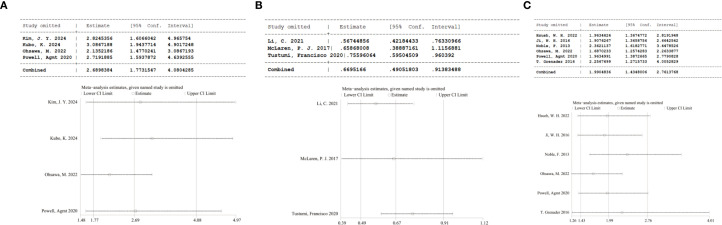 Figure 3
Figure 3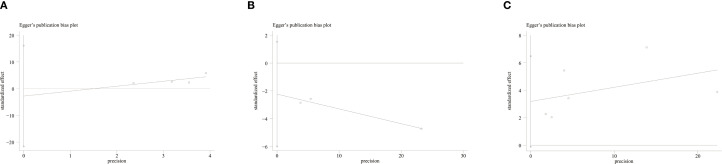 Figure 4
Figure 4| Author | Year | Source of patients | Study type | Population | Age | Duration | Sample size | Treatments | TNM stage | NLR cut-off | Timing of detection |
|---|---|---|---|---|---|---|---|---|---|---|---|
| T. Grenader ( | 2016 | UK and Australia | Prospective cohort | Esophageal gastric cancer | NA | 2000-2005 | 908 | NCT | NA | 3 | baseline |
| Hsueh, W. H ( | 2022 | China | Prospective cohort | squamous cell carcinoma | 56 | 2016-2017 | 123 | NCRT | II-IV | 3.1 | baseline |
| Ji, W. H ( | 2016 | China | Retrospective cohort | squamous cell carcinoma | 56.6 | 2009-2012 | 41 | NCT | NA | 5 | baseline |
| Li, C ( | 2021 | China | Retrospective cohort | squamous cell carcinoma | 54.77 | 2007-2016 | 127 | NCRT | II-III | 5.4 | baseline |
| McLaren, P. J ( | 2017 | US | Retrospective cohort | squamous cell carcinoma and adenocarcinoma of esophagus | NA | 2005-2015 | 60 | NCRT | NA | NA | baseline |
| Ohsawa, M ( | 2022 | Japan | Retrospective cohort | squamous cell carcinoma | NA | 2003-2018 | 163 | NCRT | NA | 4.5 | baseline |
| Powell, Agmt ( | 2020 | UK | Retrospective cohort | adenocarcinoma of esophagus | 68 | 2010-2018 | 136 | NCT | I-III | 2.25 | baseline |
| Tustumi, Francisco ( | 2020 | NA | Retrospective cohort | squamous cell carcinoma and adenocarcinoma of esophagus | 60.9 | 2009-2019 | 149 | NCRT | NA | NA | baseline |
| Noble, F ( | 2013 | UK | Retrospective cohort | Esophageal gastric cancer | 67 | 2005-2010 | 246 | NCT | II-III | 2.5 | baseline |
| Kim, J. Y ( | 2024 | South Korea | Retrospective cohort | squamous cell carcinoma | 63 | 2007-2017 | 123 | NCRT | II-III | 2.5 | baseline |
| Kubo, K ( | 2024 | Japan | Retrospective cohort | squamous cell carcinoma | 64.1 | 2015-2020 | 144 | NCT | I-IV | 3 | NA |
| Subgroup | OS | RFS | ||||||
|---|---|---|---|---|---|---|---|---|
| Study | HR [95%CI] | P value | I2 | Study | HR [95%CI] | P value | I2 | |
| Total | 6 | 1.99 [1.43, 2.76] | P<0.00001 | 88% | 4 | 2.69 [1.77, 4.08] | P<0.00001 | 47% |
| Sample size | ||||||||
| ≤130 | 2 | 2.28 [1.52, 3.41] | P<0.0001 | 0% | 1 | 2.26 [1.22, 4.19] | P=0.01 | NA |
| >130 | 4 | 1.86 [1.28, 2.70] | P=0.001 | 92% | 3 | 2.82 [1.61,4.97] | P=0.0003 | 61% |
| Follow-up | ||||||||
| ≤36mouths | 3 | 1.84 [1.43, 2.35] | P<0.00001 | 27% | 1 | 1.91 [1.10,3.32] | P=0.02 | NA |
| >36mouths | 3 | 2.13 [0.90, 5.04] | P=0.09 | 92% | 3 | 3.09 [1.94, 4.90] | P<0.00001 | 47% |
| Age | ||||||||
| <60years old | 3 | 1.84 [1.43, 2.35] | P<0.00001 | 27% | 0 | NA | NA | NA |
| >60years old | 3 | 2.13 [0.90, 5.04] | P=0.09 | 92% | 4 | 2.69 [1.77, 4.08] | P<0.00001 | 47% |
| Line of therapy | ||||||||
| NCRT | 2 | 2.84 [1.58,5.12] | P=0.0005 | 69% | 2 | 3.25 [1.68,6.28] | P=0.0005 | 64% |
| NCT | 4 | 1.58 [1.15,2.18] | P=0.004 | 86% | 2 | 2.07 [1.31,3.28] | P=0.002 | 0% |
| NLR cut-off | ||||||||
| NLR cut-off ≤ 3 | 3 | 1.49 [1.09, 2.03] | P=0.01 | 89% | 3 | 2.14 [1.48,3.09] | P<0.0001 | 0% |
| NLR cut-off>3 | 3 | 2.91 [1.87, 4.52] | P<0.00001 | 41% | 1 | 4.44 [3.69, 7.33] | P<0.00001 | NA |
| Outcomes | No. of studies | HR or OR | 95%CI |
| Risk of bias | Inconsistency | Indirectness | Imprecision P<0.001 | Publication bias | Plausible confounding | Magnitude of effect | Dose-response gradient | GRADE |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OS | 6 | 1.99 | 1.43, 2.76 | 88%; P<0.0001 | Serious risk | Serious inconsistency | No serious | No Serious | Undetected | Would not | No | No | Very Low |
| RFS | 4 | 2.69 | 1.77,4.08 | 47%;P<0.00001 | Serious risk | No Serious inconsistency | No serious | No Serious | Undetected | Would not | Yes | No | Very Low |
| pCR(OR) | 3 | 0.67 | 0.47, 0.94 | 62%;P=0.02 | Serious risk | serious | No serious | Serious | Undetected | Would not | No | No | Very Low |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal Cancer Research and Treatment · Inflammatory Biomarkers in Disease Prognosis · Pancreatic and Hepatic Oncology Research
Introduction
1
Esophageal cancer (EC), one of the most lethal malignancies worldwide, represents the seventh predominant cause of global mortality related to cancer (1). Though there have been notable advancements in therapeutic approaches and critical care in recent decades, the EC population demonstrates one of the least favorable five-year survival outcomes in contrast to other cancers (2). The GLOBOCAN 2020 global cancer statistics showed approximately 604,000 new and 544,000 dead cases attributable to EC, ranking seventh and sixth in incidence and mortality, among all malignancies (3). Notably, nearly half of all new cases and deaths occurred in East Asia (4). Its treatment presents unique challenges owing to the anatomical proximity of the esophagus to the airway and main blood vessels, no serosal layer, and its rich surrounding lymphatic network. Furthermore, patients are commonly diagnosed at a late stage and frequently malnourished, further complicating treatment (5). We accurately determined the stage of esophageal cancer according to the international esophageal cancer diagnostic guidelines, which is important for us to choose the appropriate treatment, so that we can provide individualized treatment pathways for patients with different stages of esophageal cancer (6).In the early stage, surgical resection is still the mainstay and most effective approach. However, due to the insidious onset and aggressive nature of EC, many cases are detected at advanced stages, thereby missing the best opportunity for curative surgery (7). With a better understanding of the disease, various treatment strategies have been developed for the locally advanced EC population, like neoadjuvant chemoradiotherapy (NCRT), neoadjuvant chemotherapy (NCT), as well as immunotherapy with surgery (8). Evidence suggests that NCRT significantly improves overall survival (OS) in locally advanced EC, with clinical benefits observed across different histological subtypes (9); Similarly, several studies have reported a survival advantage with NCT in this patient population (10). In terms of recurrence-free survival (RFS), Zhang et al. demonstrated that neoadjuvant treatment - whether NCRT or NCT - contributes positively to improved outcomes (11); Furthermore, Lewis et al. found that neoadjuvant therapy increases the pathological complete response (pCR) rate compared to surgery alone (12). Hence, early and accurate prognostic assessment is critical for guiding individualized treatment decisions in clinical practice.
Tumor progression is influenced by both tumor-specific factors and the host immune response (13, 14). Therefore, systemic inflammatory markers are prospective prognostic indicators. A low neutrophil-to-lymphocyte ratio (NLR) influences favorable outcomes in various malignancies, including non-small cell lung cancer, gastric cancer, colorectal cancer, and hepatocellular carcinoma (15, 16). Systemic inflammation can be assessed via alterations in peripheral blood cell counts of lymphocytes, monocytes, neutrophils, and platelets. Composite hematological indices, like the NLR and platelet-to-lymphocyte ratio (PLR), have been proposed as accessible prognostication biomarkers. In 2021, Li et al.’s study, which included 127 patients, NLR was a dependable indicator of prognosis for EC sufferers undergoing neoadjuvant therapy (17). Conversely, a contemporaneous study by Anand et al. reported limited predictive value of NLR in this context (18). These conflicting findings underscore the need for further investigation into the prognosis utility of NLR among the EC population after neoadjuvant therapy.
To date, a substantial number of both retrospective and prospective investigations have examined the predictive value of NLR in this context, yet a comprehensive meta-analysis to consolidate the available research findings remains lacking. Therefore, our study unveiled the prognosis relevance of NLR among EC individuals taking neoadjuvant therapy via a systematic review and meta-analysis. GRADE methodology and subgroup analyses were employed to assess the evidence quality and identify possible sources of heterogeneity. Ultimately, this study seeks to present evidence-based recommendations for the clinical adoption of NLR as a readily available hematological biomarker to facilitate prognostic stratification and guide therapeutic decision-making, ameliorating outcomes for the EC population.
Materials and methods
2
Literature search
2.1
Our study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines (19). Our study protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; Registration No.: CRD42024610088). LWM and JXH developed the search strategy and independently have searched terms and keywords comprehensively across PubMed, Embase, Web of Science, and the Cochrane Library up to April 22, 2025. A broad range of search terms was employed, such as “EC,” “neoadjuvant therapy,” “neutrophils,” “lymphocytes,” “NCRT,” “NCT,” and “NLR.” The strategy is provided in Supplementary Table 1.
Study selection
2.2
The inclusion criteria were: (1) EC diagnosis based on endoscopic evaluation and histopathological biopsy; (2) patients received preoperative neoadjuvant therapy, including NCRT or NCT, with commonly used regimens comprising epirubicin and cisplatin with fluorouracil or capecitabine, or epirubicin and oxaliplatin with fluorouracil or capecitabine; (3) evaluating the prognostic utility of NLR on OS, RFS, and pCR; (4) hazard ratio (HR) data with corresponding 95% confidence intervals (CIs) were offered or could be computed; (5) patients were divided into high- and low-NLR cohorts based on a defined cutoff value; (6) only fully published studies were considered. The exclusion criteria were: (1) reviews, commentaries, conference abstracts, and case reports, as well as letters; (2) insufficient information for HRs and 95% CIs computation; (3) no survival outcome data; and (4) duplicate or overlapping data.
Two reviewers (LWM and JXH) independently checked the titles and abstracts, accessed the full texts, and assessed eligibility. Any dissents in the selection process were addressed via discussion and consensus. 34studies published in English were identified through the search strategy applied across the four databases. These studies were initially translated utilizing the professional translation software “ZhiYun,” followed by independent data extraction conducted by two English-proficient investigators (LWM and JXH). Any terminological inconsistencies encountered during translation were resolved in consultation with a third English-language expert (Dr. YCD) to reach a consensus. Data extraction strictly adhered to the PICOS framework, and key prognostic indicators were systematically recorded utilizing standardized data collection forms.
Data extraction
2.3
LWM and JXH independently gathered information. Dissents were addressed after consensus. Gathered data comprised the first author, publication year, country (study location), design, sample size, age, duration, pathological stage, treatment, timing of NLR assessment, cutoff value, follow-up length, as well as HRs with 95% CIs for OS, RFS, and pCR.
Quality assessment
2.4
The study quality was rated via the Newcastle-Ottawa Scale (NOS) assessing selection, comparability, as well as outcome. The maximum score for each study was 9 points (20). 7–9 denoted high quality (21). Agreement statistics between two authors (LWM and JXH) regarding study selection were performed using Cohen’s kappa statistics and associated 95% CI. Magnitude of agreement was interpreted following guidelines reported by Landis and Koch: slight (0.00-0.20), fair (0.21-0.40), moderate (0.41-0.60), substantial (0.61-0.80), and almost perfect agreement (0.81-1.00) (22).
Statistical analysis
2.5
Pooled HRs with corresponding 95% CIs were derived for assessing NLR’s prognosis utility among the EC population who received neoadjuvant therapy. Heterogeneity was examined utilizing Cochran’s Q test and Higgins’ I² statistic (23). Each statistical analysis adopted a random-effects model. To examine the stability of our OS、RFS and pCR findings, subgroup and sensitivity analyses were carried out. Funnel plots and Egger’s test assessed possible publication bias. Two-tailed P<0.05 suggested statistical significance. Every analysis was enabled by STATA 15.0 and Review Manager 5.4.
GRADE classification
2.6
Moreover, the evidence quality was rated utilizing the GRADE approach as “high,” “moderate,” “low,” or “very low” (24). Due to serious concerns regarding heterogeneity and imprecision, the quality of evidence for the relationships of NLR with OS, RFS, and pCR was rated as “very low.”
Results
3
Study characteristics
3.1
34 articles were initially identified through database searches. After removing seven duplicate publications, seven additional studies were excluded after title and abstract review. The full texts of the rest were checked, with nine excluded primarily due to partial or insufficient data relevant to the present analysis. Ultimately, eleven studies comprising 2,220 patients were encompassed (Figure 1).
Flow chart of literature screening.
Among the eleven eligible studies (25–33), six were conducted in Asian countries, while four originated from Western countries like the United Kingdom and the United States. Notably, all eleven studies were cohort studies, with nine being retrospective in design (5, 17, 27–33) and two being prospective (25, 26). All studies were published in English between 2016 and 2025. Each included study investigated EC sufferers who received neoadjuvant therapy, and participants were split into high and low NLR cohorts. Regarding NLR assessment, eight studies measured NLR before the initiation of neoadjuvant therapy, one study assessed preoperative NLR and two studies evaluated both pre-neoadjuvant and preoperative NLR levels. Based on these assessments, six studies examined the prognostic impact of NLR on OS, four studies focused on recurrence-free survival (RFS), and three studies investigated its association with pathologic complete response (pCR). The characteristics are presented in Table 1.
Study quality
3.2
11 eligible studies scored 7–9 on the NOS, indicating high methodological quality (Supplementary Table 2).Agreement between the two reviewers (LWM and JXH) for study selection was almost perfect (κ = 0.906, 95% CI 0.859 to 0.953, P < 0.001).
Meta-analysis results
3.3
NLR and pCR
3.3.1
Three studies including 336 participants were analyzed to investigate the link of NLR to pathological complete response(pCR). Among EC patients receiving neoadjuvant therapy, a lower NLR was evidently linked to a risen pCR rate (OR = 0.67, 95% CI = 0.47–0.94, P = 0.02; I² = 62%) (Figure 2A), indicating an inverse relationship between NLR and treatment response.
(A) Forest plots for the association between NLR and pCR; (B) Forest plots for the association between NLR and OS; (C) Forest plots for the association between NLR and RFS.
NLR and OS
3.3.2
The relationship between NLR and OS was examined across six cohort studies involving 1,617 participants. Due to substantial heterogeneity (I² = 88%, P < 0.00001), a random-effects model was leveraged (Figure 2B). A higher NLR was notably related to poorer OS among the EC population following neoadjuvant therapy (HR = 1.99, 95% CI = 1.43–2.76, P < 0.0001; I² = 88%) (Figure 2B).
NLR and RFS
3.3.3
Four studies involving 566 participants provided data on the link of NLR to RFS. Consistent with the findings for OS, elevated NLR was markedly linked to shortened RFS (HR = 2.69, 95% CI = 1.77–4.08, P < 0.00001; I² = 47%) (Figure 2C) among patients treated with neoadjuvant therapy.
Subgroup analysis
3.4
To detect probable sources of heterogeneity, subgroup analyses regarding NLR were executed. Elevated NLR independently predicted poorer OS and RFS, regardless of age, follow-up duration, sample size, treatment modality and NLR cut-off value.
Firstly, subgroup analyses by sample size and treatment modality consistently showed a marked link of increased NLR to shortened OS (P < 0.05). Notably, the subgroup receiving NCRT showed a stronger association (HR = 2.84, 95% CI: 1.58–5.12, P = 0.0005) in contrast to the subgroup receiving NCT alone (HR = 1.58, 95% CI: 1.15–2.18, P = 0.004). Secondly, subgroup analysis by follow-up length indicated that among patients with follow-up less than 36 months, higher NLR was markedly linked to shorter OS (HR = 1.84, 95% CI: 1.43–2.35, P < 0.00001), while notable relation was not found in those with follow-up longer than 36 months (P = 0.09). Thirdly, age-based subgroup analysis showed that in patients younger than 60, elevated NLR evidently predicted less favorable OS (HR = 1.84, 95% CI: 1.43–2.35, P < 0.00001), whereas marked prognostic influence was not observed among those aged 60 or older (P = 0.09).Finally, based on the subgroup analysis of NLR cut-off values, both the subgroup with NLR cut-off value ≤ 3 and the subgroup with NLR cut-off value > 3 showed that higher NLR often indicated poor OS was statistically significant(P<0.05). Notably, the subgroup with NLR cut-off value>3 (HR = 2.91,95% CI = 1.87-4.52; P< 0.00001) showed a stronger correlation than the subgroup with NLR cut-off value ≤ 3 (HR = 1.49,95% CI = 1.09-2.03; P = 0.01).
Subgroup analyses for RFS based on the same parameters (sample size, follow-up time, age, treatment modality, and NLR cut-off value) all demonstrated a statistically significant relation of elevated NLR to shorter RFS (P < 0.05), indicating the robustness of NLR as a prognostic marker for RFS. Notably, a stronger link of risen NLR to reduced RFS was observed in patients with follow-up lasting over 36 months (HR = 3.09, 95% CI: 1.94–4.90, P < 0.00001) in contrast to those with shortened follow-up. Similarly, the NCRT subgroup showed a stronger correlation between elevated NLR and shortened RFS (HR = 3.25, 95% CI: 1.68–6.28, P = 0.0005) than the NCT subgroup. These findings are consistent with the OS results and warrant further investigation (Table 2).Otherwise, Subgroup analysis based on NLR cut-off values showed that there was a significant statistical difference between higher NLR and shorter RFS (P<0.05).NLR cut-off value > 3 subgroup had better predictive performance for RFS than NLR cut-off value ≤ 3 subgroup.
Sensitivity analysis
3.5
Sensitivity analyses assessed the influence of separate studies on the overall effect size and evaluated the resulting robustness concerning NLR’s clinical relevance. For NLR and RFS (P = 0.13, I² = 47%), sequential exclusion of each study yielded consistent results within the original effect range, suggesting that no individual study disproportionately influenced our pooled estimate for RFS and confirming the reliability of the RFS findings (Figure 3A). For NLR and pCR, the exclusion of the study by McLaren P. J (2017) (29).altered the pooled result from statistically significant to insignificant (HR = 0.66, 95% CI: 0.39–1.12), indicating considerable effects of this study on the overall effect (Figure 3B). For NLR and OS (P < 0.00001, I² = 88%), sequential exclusion of individual studies also yielded consistent results within the original effect range, confirming that OS results were not disproportionately affected by any study and validating the reliability of the link of NLR to OS (Figure 3C).
(A) Sensitivity analysis of RFS; (B) Sensitivity analysis of pCR; (C) Sensitivity analysis of OS.
Publication bias
3.6
Publication bias was detected via funnel plots and Egger’s test. The funnel plots for RFS (Figure 4A), pCR (Figure 4B), and OS (Figure 4C) did not show significant asymmetry, suggesting no obvious publication bias. Additionally, Egger’s test presented insignificant results regarding OS (P = 0.055), RFS (P = 0.591), and pCR (P = 0.084), further showing no publication bias.
(A) Funnel plot for the evaluation of publication bias for RFS; (B) Funnel plot for the evaluation of publication bias for pCR; (C) Funnel plot for the evaluation of publication bias for OS.
GRADE classification
3.7
Through the GRADE approach, the evidence quality was classified as “high,” “moderate,” “low,” or “very low” as per standard criteria. This classification was used to assess the strength of recommendations for applying NLR as a prognostic indicator in EC sufferers receiving neoadjuvant therapy, thereby informing clinical decision-making (22). Due to substantial heterogeneity and imprecision, the quality of evidence for OS, RFS, and pCR was rated as very low (Table 3).
Discussion
4
Inflammation, a key feature of the tumor microenvironment, is crucial in cancer initiation, cell proliferation, angiogenesis, as well as metastasis during tumor progression (34, 35). Several studies have demonstrated that inflammatory markers hold prognostic value in cancer treatment and outcome prediction (36). Among them, NLR has been a proven prognostic indicator. In non-small cell lung, colorectal, gastric, ovarian cancers, hepatocellular and renal cell carcinomas (37–42), NLR is related to patient prognosis. Zhang CL et al. identified that NLR notably predicts survival and treatment response among the ovarian cancer population (43). Similarly, Mi HL et al.’s retrospective research on NLR in lung cancer proved that higher NLR can independently be adopted for forecasting reduced RFS (44). These findings suggest that NLR, a non-invasive, easily accessible, and cost-effective hematologic marker, may provide valuable prognostic information across various types of cancer.
This meta-analysis, which included 2,220 patients, demonstrated that NLR evidently correlates with OS, RFS, and pCR among the EC population. These findings have been validated by other studies. For instance, a 2021 study reported that among EC patients who received NCRT, those who achieved pCR exhibited evidently lower NLR levels (HR = 1.218, 95% CI = 1.050–1.414, P = 0.009) (45). Another meta-analysis published in 2024 unveiling NLR’s prognostic relevance in EC also proved that elevated NLR is markedly linked to worse OS (HR = 1.47, 95% CI = 1.29–1.67, P < 0.00001) (46). These consistent results reinforce our conclusion that NLR is a qualified and reliable prognostic indicator. As a cost-effective and easily obtainable hematological marker, NLR can facilitate the rapid construction of prognostic models and serve as a feasible component in the development of comprehensive prognostic prediction tools. Our subgroup analysis showed that NCRT offers greater prognostic benefits than NCT among the EC population. Furthermore, the subgroup analyses for RFS across various parameters demonstrated robust statistical power. Prognostic models constructed through this approach can assist clinicians in accurately assessing patient outcomes and adjusting treatment strategies in a timely manner, thereby potentially improving prognosis in high-risk individuals.
Our study elucidated the link of NLR to OS and RFS in EC sufferers and included subgroup analyses by sample size, follow-up duration, age, and treatment regimen. For OS, NLR showed a significant association among patients with a follow-up length of ≤36 months, while no marked link was observed in those with a follow-up lasting over 36 months. This may be due to increased loss to follow-up over longer durations, which can bias statistical analyses in retrospective studies and reduce the significance of subgroup findings with extended follow-up. Among patients aged <60, higher NLR was linked to shorter OS, whereas no significant association was found in patients aged >60. Rui et al. (47) demonstrated that the mortality risk of EC increases with age. Aging is accompanied by a gradual decline in immune function and cumulative exposure to risk factors, both of which contribute to higher mortality. This could account for the lack of statistical significance in NLR’s prediction value for OS among patients aged above 60. Notably, in the NCRT cohort, the prognostic effect of NLR (HR = 2.84, 95% CI = 1.58–5.12, P = 0.0005) was stronger than the NCT receivers(HR = 1.58, 95% CI = 1.15–2.18, P = 0.004). Similarly, for RFS, the link of NLR to prognosis was stronger in the NCRT group (HR = 3.25, 95% CI = 1.68–6.28, P = 0.0005) than in the NCT subgroup (HR = 2.07, 95% CI = 1.37–3.28, P = 0.002). Multiple studies have shown that perioperative NCRT, compared to NCT alone, offers superior benefits in terms of prognosis and postoperative complications among the EC population (48, 49). In our RFS subgroup analyses, all predefined subgroups demonstrated a significant link between NLR and patient outcomes. This consistent cross-subgroup finding further supports the reliability of NLR as a prognosis biomarker in EC, suggesting that its predictive value is largely independent of these clinical variables. Of note, our subgroup analysis also demonstrated that the subgroup with an NLR cut-off value > 3 exhibited better predictive performance for RFS compared to the subgroup with an NLR cut-off value ≤ 3. The superior predictive ability of an NLR cut-off > 3 may be attributed to the fact that a higher threshold more effectively identifies patients with severe systemic inflammation, which is closely associated with tumor recurrence.
This study explored the link of NLR to the prognosis of EC and conducted a comprehensive sensitivity analysis to ensure result robustness and reliability. All sensitivity analyses were performed utilizing a random-effects model. The stability of our pooled estimates was examined utilizing a leave-one-out approach. For NLR and RFS (I² = 47%, P = 0.13), heterogeneity was relatively low, and the effect sizes remained the same within the original range upon sequential exclusion of individual studies, indicating good stability in the RFS-related findings. In contrast, for NLR and pCR (I² = 62%, P = 0.07) and NLR and OS (I² = 88%, P < 0.00001), significant heterogeneity persisted even after stepwise study ostracization. This possibly arises from variations in study populations from various countries and regions, variability in study periods, and the relatively small sample sizes, which introduce both temporal and geographic heterogeneity. Taken together, the sensitivity analysis suggests that, despite differences in patient characteristics and study design, the prognostic value of NLR remains robust. Probable publication bias was examined utilizing Egger’s test. No publication bias existed in the analyses of OS, RFS, and pCR in relation to NLR. Furthermore, GRADE assessments were executed and evidence was rated as “very low” for each outcome. This was mainly due to the observational nature of eligible studies, which are inherently prone to methodological limitations. Therefore, Additional high-quality prospective research is necessitated for verifying and strengthening the evidence base for the prognostic utility of NLR in this setting. Ultimately, the goal is to provide clinicians with better tools for making informed decisions on the post-neoadjuvant treatment of EC sufferers. From the perspective of outcome stability, our findings further confirm that elevated NLR is significantly associated with worse OS and RFS, while its association with lower pCR rates is less stable due to the influence of individual studies; this is consistent with the sensitivity analysis result that excluding the McLaren P. J (2017). study altered the statistical significance of the pCR-related association.
Neutrophils exhibit an intricate role in the tumor microenvironment. Once recruited by tumor cells into the tumor milieu, neutrophils become tumor-associated neutrophils (TANs): N1 and N2 phenotypes. TANs support tumor growth primarily by releasing proliferative factors, suppressing T-cell activity, and promoting tumor angiogenesis (50). In contrast, lymphocytes are central to antitumor immunity. CD8^+^ T cells are cytotoxic against tumor cells via the secretion of IFN-γ and TNF-α, while CD4^+^ T cells activate antigen-presenting cells and enhance the cytotoxic effects of both CD8^+^ T cells and NK cells, thereby inhibiting tumor growth and metastasis (51, 52). Lymphocyte count decrease is often connected with poor prognosis among the EC population (53). A risen NLR usually reflects a relative elevation in neutrophils and/or a drop in lymphocytes. Neutrophils suppress the activity of lymphocytes and NK cells, diminishing antitumor immune responses, while also contributing to systemic inflammation through the release of pro-inflammatory mediators. Conversely, lymphopenia weakens the ability of the immune system to target and eliminate tumor cells, thereby facilitating tumor invasion and metastasis (54). Lymphocytes play crucial roles in restraining tumor cell proliferation, and metastasis, and promoting cytotoxicity and apoptosis, whereas neutrophils facilitate tumor progression by producing growth factors, chemokines, and proteases (55). When elevated neutrophil counts and reduced lymphocyte counts co-occur, the predictive value for tumor progression may be further enhanced. Thus, NLR is regarded as a potential prognostic biomarker for EC sufferers following neoadjuvant therapy. Despite presenting valuable insights, this meta-analysis has limitations. Most incorporated studies were retrospective, with only two being prospective. The retrospective design may introduce uncontrolled confounding factors that could bias the conclusions. Moreover, most were conducted in Asia and Europe, suggesting potential geographic limitations. Therefore, broad generalizations to non-studied populations should be approached with caution. Further research is required to validate NLR’s prognostic relevance among the EC population undergoing neoadjuvant therapy in other geographic settings. Additionally, variability in the cutoff values and timing of NLR measurement may introduce heterogeneity and confounding effects that are difficult to control. Differences in treatment regimens across studies may also contribute to the inconsistency in results. Therefore, subsequent researchers should focus on standardizing when NLR is measured, selecting consistent treatment approaches, and determining clear, measurable NLR thresholds.
Conclusion
5
In conclusion, following neoadjuvant therapy, elevated NLR is markedly linked to poor prognosis among the EC population, including reduced OS and RFS and lower pCR. Therefore, NLR is a low-cost, non-invasive, and easily accessible biomarker for forecasting the prognosis of EC sufferers. It can aid clinicians in timely developing optimal treatment plans based on the potential risk of poor outcomes. Notably, this hematological biomarker may be valuable for forecasting the prognosis of EC in underdeveloped or resource-limited regions, especially in clinical settings where genomic monitoring is not feasible. However, due to some inevitable limitations and confounding factors in the included studies, it is recommended to carry out a multi-center prospective study to standardize the NLR measurement time, such as baseline and cutoff values before treatment, in order to confirm the conclusions of this study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yang X Tang Z Li J Jiang J . Esophagus cancer and essential trace elements. Front Public Health. (2022) 10:1038153. doi: 10.3389/fpubh.2022.1038153, PMID: 36466456 PMC 9709130 · doi ↗ · pubmed ↗
- 2Bray F Laversanne M Sung H Ferlay J Siegel RL Soerjomataram I . Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834, PMID: 38572751 · doi ↗ · pubmed ↗
- 3Sung H Ferlay J Siegel RL Laversanne M Soerjomataram I Jemal A . Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660, PMID: 33538338 · doi ↗ · pubmed ↗
- 4Arnold M Abnet CC Neale RE Vignat J Giovannucci EL Mc Glynn KA . Global burden of 5 major types of gastrointestinal cancer. Gastroenterology. (2020) 159:335–49.e 15. doi: 10.1053/j.gastro.2020.02.068, PMID: 32247694 PMC 8630546 · doi ↗ · pubmed ↗
- 5Kim JY Yun JK Kim YH Park SI Lee JH Jung HY . Prognostic impact of inflammation-based factors in patients with esophageal squamous cell carcinoma achieving pathological complete response after neoadjuvant chemoradiotherapy followed by surgery. Ann Surg Oncol. (2024) 31:6662–72. doi: 10.1245/s 10434-024-15678-y, PMID: 38954089 · doi ↗ · pubmed ↗
- 6Yuan Y Chen LQ . Interpretation of update on the AJCC esophageal cancer staging system, eighth edition. Zhonghua Waike Zazhi. (2017) 55:109–13. doi: 10.3760/cma.j.issn.0529-5815.2017.02.007, PMID: 28162209 · doi ↗ · pubmed ↗
- 7Shi X Zhao H Yu J Cai P Zhou S Yang N . Changes in PD-1 expression on T lymphocyte subsets and related immune indicators before and after definitive chemoradiotherapy for esophageal squamous cell carcinoma. Ann Med. (2025) 57:2445190. doi: 10.1080/07853890.2024.2445190, PMID: 39713872 PMC 11703528 · doi ↗ · pubmed ↗
- 8Kato K Machida R Ito Y Daiko H Ozawa S Ogata T . Doublet chemotherapy, triplet chemotherapy, or doublet chemotherapy combined with radiotherapy as neoadjuvant treatment for locally advanced oesophageal cancer (JCOG 1109 N Ex T): a randomised, controlled, open-label, phase 3 trial. Lancet. (2024) 404:55–66. doi: 10.1016/S 0140-6736(24)00745-1, PMID: 38876133 · doi ↗ · pubmed ↗