Improvement in Protein-Losing Gastroenteropathy Due to Gastric Polyposis by Laparoscopic Total Gastrectomy: A Case Report
Manatsu Mizuno, Takuro Saito, Shigeto Nakai, Takaomi Hagi, Kota Momose, Kotaro Yamashita, Koji Tanaka, Tomoki Makino, Tsuyoshi Takahashi, Yukinori Kurokawa, Hidetoshi Eguchi, Yuichiro Doki

TL;DR
A man with a rare genetic condition had successful treatment for severe stomach and intestinal issues through a minimally invasive stomach removal surgery.
Contribution
Laparoscopic total gastrectomy is shown to effectively treat protein-losing gastroenteropathy in gastric juvenile polyposis syndrome.
Findings
The patient's symptoms resolved after laparoscopic total gastrectomy.
The patient remained healthy for 4 years post-surgery without symptom recurrence.
The procedure eliminated the risk of malignant transformation of gastric polyps.
Abstract
Juvenile polyposis syndrome (JPS) is a rare disease characterized by multiple hamartomatous polyps in the gastrointestinal tract that may cause protein-losing gastroenteropathy. In such cases, symptoms such as hypoalbuminemia and anemia are often difficult to manage. Although clinical guidelines provide recommendations for diagnosis and management, standardized treatment strategies remain to be fully established. A 40-year-old man underwent laparoscopic total gastrectomy for protein-losing gastroenteropathy secondary to gastric polyposis. He had a history of colorectal polyposis associated with an SMAD4 mutation and had previously undergone subtotal colectomy. The patient developed worsening anemia and hypoproteinemia. Upper gastrointestinal endoscopy revealed an increase in both the size and number of gastric polyps. Protein-losing gastroenteropathy was diagnosed using technetium-99m…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
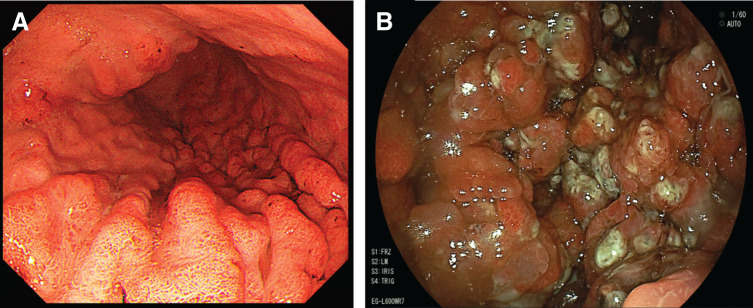 Fig. 1
Fig. 1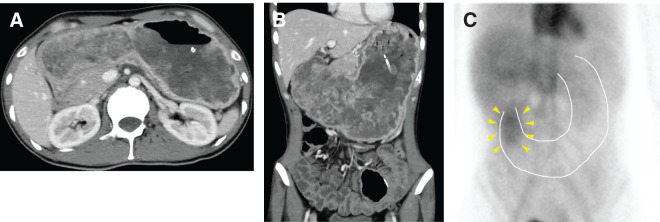 Fig. 2
Fig. 2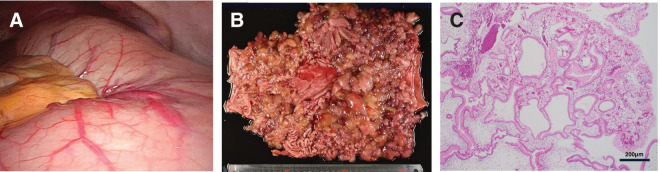 Fig. 3
Fig. 3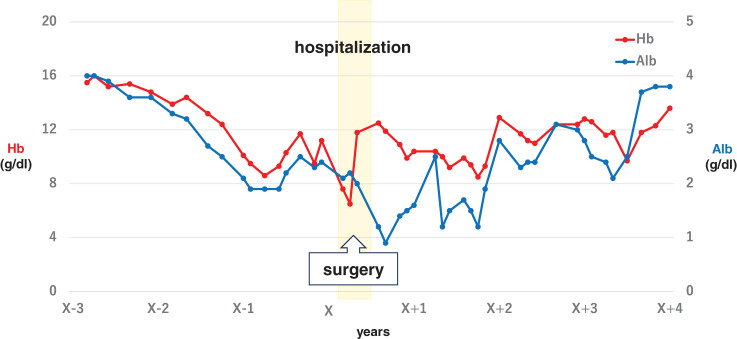 Fig. 4
Fig. 4| No. | Author | Year | Sex | Age | Polyp location | Anemia/low protein | 99mTc-HAS scintigraphy | Cancer | Cancer location | Lap/open | Number of ports | Improvement in anemia/low protein | Postoperative follow-up period (months) | Treatment for colorectal polyposis |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Hamamoto | 1994 | F | 36 | Fundus–body | −/− | – | + | Fundus | Open | nd/nd | nd | – | |
| 2 | Hirata | 2000 | F | 63 | Whole | +/+ | – | – | Open | nd/nd | nd | – | ||
| 3 | Furukawa | 2000 | M | 57 | Whole | +/+ | – | + | Antrum | Open | nd/nd | nd | – | |
| 4 | Harada | 2001 | M | 49 | Whole | +/+ | – | – | Open | +/+ | nd | – | ||
| 5 | Komatsu | 2004 | M | 60 | Whole | +/+ | – | – | Open | +/+ | 6 | – | ||
| 6 | Yamaguchi | 2004 | M | 48 | Whole | +/+ | – | – | Open | +/+ | 24 | – | ||
| 7 | Yamanaka | 2008 | M | 44 | Upper–lower body | −/− | – | + | Middle body | Open | nd/nd | 12 | – | |
| 8 | Yagi | 2009 | F | 60 | Whole | +/+ | – | + | Antrum | Open | +/+ | nd | – | |
| 9 | Takashima | 2009 | F | 50 | Middle body–antrum | −/+ | – | + | Antrum | Open | +/+ | 30 | – | |
| 10 | Yamashita | 2009 | M | 28 | Whole | +/+ | + | – | Open | +/+ | nd | Colorectal polypectomy | ||
| 11 | Ozawa | 2010 | F | 48 | Whole | +/+ | – | + | Antrum | Open | nd/nd | 24 | – | |
| 12 | Matsui | 2010 | M | 39 | Whole | +/+ | – | – | Open | +/+ | nd | – | ||
| 13 | Mizuuchi | 2011 | F | 47 | Upper body–antrum | +/+ | – | – | Lap | 5 ports | +/+ | 2 | – | |
| 14 | Okubo | 2013 | F | 42 | Whole | +/+ | – | – | Open | +/+ | 4 | – | ||
| 15 | Nagasue | 2013 | F | 42 | Whole | +/+ | – | – | Lap | nd | +/+ | nd | – | |
| 16 | Honda | 2013 | F | 29 | Body–antrum | +/+ | – | – | Lap | nd | nd/nd | nd | No treatment | |
| 17 | Sato | 2014 | F | 28 | Middle body–pylorus | +/+ | – | – | Lap | 5 ports | +/+ | 1 | – | |
| 18 | Suzuki | 2015 | F | 49 | Whole | +/+ | – | – | Lap | 5 ports | +/+ | 12 | – | |
| 19 | Matsuo | 2015 | F | 37 | Whole | +/+ | – | + | Antrum | Lap | nd | nd/nd | nd | – |
| 20 | Ochi | 2016 | F | 50 | Whole | +/+ | – | + | Antrum | Open | nd/nd | nd | – | |
| 21 | Yube | 2018 | F | 48 | Whole | +/+ | – | + | Whole | Lap | nd | nd/nd | 7 | – |
| 22 | Jogo | 2018 | M | 63 | Whole | +/+ | – | + | Lower body | Lap | nd | nd/nd | 16 | – |
| 23 | Nakagawa | 2019 | M | 48 | Whole | +/+ | – | – | Open | +/+ | 9 | – | ||
| 24 | Ito | 2022 | F | 43 | Whole | +/+ | – | + | Antrum | Lap | nd | nd/nd | nd | – |
| 25 | Sakai | 2022 | F | 57 | Whole | +/+ | – | + | Middle body | Lap | 5 ports | nd/nd | 12 | – |
| 26 | Takahashi | 2023 | F | 53 | Whole | +/+ | – | – | Lap | 5 ports | nd/nd | nd | – | |
| 27 | Niya | 2023 | F | 42 | Whole | +/+ | – | + | Antrum | Open | nd/nd | 14 | – | |
| 28 | Utsunomiya | 2023 | F | 70 | Upper–middle body | +/+ | – | + | Body | Lap | nd | +/+ | nd | – |
| 29 | Nakamura | 2024 | M | 33 | Stomach–duodenum | +/+ | – | – | Open (TG + PD) | nd/nd | 18 | – | ||
| 30 | Our case | – | M | 40 | Whole | +/+ | + | – | Lap | 5 ports | +/+ | 48 | Subtotal colectomy |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic factors in colorectal cancer · Gastrointestinal Tumor Research and Treatment · Helicobacter pylori-related gastroenterology studies
Abbreviations
99mTc-HSA technetium-99m human serum albumin JPS juvenile polyposis syndrome
INTRODUCTION
Juvenile polyposis syndrome (JPS) is a rare disorder characterized by multiple hamartomatous polyps in the gastrointestinal tract. It is an autosomal dominant hereditary disease, with pathogenic variants in the tumor suppressor genes, SMAD4 or BMPR1A, identified in approximately 60% of cases.^1,2)^ Polyps most frequently occur in the colon (98%), followed by the stomach (14%).^3)^ In cases of gastric JPS, symptoms such as anemia due to bleeding, hypoalbuminemia, hypoproteinemia, and edema caused by protein-losing enteropathy are commonly observed. Several reports have described symptomatic improvement with surgical intervention.^4)^ Furthermore, patients with gastric JPS harboring SMAD4 mutations have a 30% risk of developing gastric cancer.^5,6)^
Herein, we report a case of gastric polyposis with protein-losing gastroenteropathy that was refractory to medical treatment. Given the risk of malignant transformation, laparoscopic total gastrectomy was performed. The patient maintained a stable nutritional status and serum protein levels for 4 years postoperatively.
CASE PRESENTATION
A 40-year-old male visited our hospital with a 2-week history of persistent vomiting and was admitted urgently. Twenty years ago, he underwent subtotal colectomy for isolated JPS due to an SMAD4 mutation and had been under regular follow-up in the Department of Gastroenterology. Three years before admission, he experienced melena, followed by progressive anemia and hypoalbuminemia. Upper gastrointestinal endoscopy revealed a polyp surrounding the gastric cardia; however, biopsy showed no evidence of malignancy. During annual surveillance endoscopies, no significant changes were observed, and no polyps were detected in the gastric body (Fig. 1A); however, at the time of the current hospitalization, endoscopy revealed markedly enlarged polyps (Fig. 1B). Capsule endoscopy was also performed as a screening examination for small intestinal lesions 1 year ago, which revealed no apparent polyps in the small intestine. Blood tests at admission showed anemia (hemoglobin: 10.8 g/dL) and hypoalbuminemia (albumin: 2.2 g/dL), while tumor marker levels were within normal limits. Contrast-enhanced CT demonstrated multiple gastric polyps and significant gastric dilation (Fig. 2A and 2B).
Endoscopic findings. (A) Three years prior to admission, no polyps were observed in the gastric body. (B) At the time of admission, a marked increase in both the size and number of polyps in the gastric body was observed.
CT findings in axial (A) and coronal (B) views. The stomach is significantly enlarged, and numerous polyps are observed inside. (C) Technetium-99m human serum albumin scintigraphy demonstrated increased tracer accumulation in the gastric antrum 6 h after injection. White dotted lines: gastric outline; yellow arrowheads, tracer accumulation.
Initial management involved gastric decompression using a nasogastric tube, but drainage remained high (1.5–2.0 L/day), and the patient continued to experience persistent diarrhea (15–20 episodes per day). Technetium-99m human serum albumin (99mTc-HSA) scintigraphy demonstrated increased tracer accumulation in the antrum 6 h after injection (Fig. 2C), indicating protein-losing gastroenteropathy originating from the gastric antrum due to juvenile polyposis. Blood transfusions and albumin infusion were administered, but these symptoms proved refractory to treatment. Therefore, surgical resection was deemed necessary due to refractory anemia, hypoalbuminemia, gastric outlet obstruction, and the potential risk of malignant transformation.
Laparoscopic total gastrectomy with Roux-en-Y reconstruction was subsequently performed, with an operative time of 229 min and blood loss of 100 mL. Intraoperative findings revealed a markedly distended stomach with limited visualization, which made standard laparoscopic port placement and exploration mildly difficult (Fig. 3A). Nevertheless, the procedure was completed without complications. Postoperatively, an umbilical surgical site infection was observed, which was likely related to preexisting hypoproteinemia. Diarrhea improved to 5–10 times per day, and oral intake was successfully resumed. The patient was discharged 26 days postoperatively.
Surgical and pathological findings. (A) Intraoperative findings revealed a markedly distended stomach with limited visualization. (B) Multiple polyps were observed throughout the gastric mucosa in the resected specimen. (C) Histopathological examination revealed hyperplasia of the glandular epithelium accompanied by stromal edema. No evidence of malignancy was identified in any of the polyps or lymph nodes.
Histopathological examination revealed foveolar epithelial hyperplasia and stromal edema (Fig. 3B and 3C). No evidence of malignancy was identified in any of the polyps or resected lymph nodes.
Following surgery, both anemia and hypoproteinemia gradually improved, and the patient was able to maintain adequate oral intake. He remains in good health and has continued a normal daily life without symptom recurrence for 4 years postoperatively (Fig. 4).
Pre- and postoperative changes in serum Alb and Hb levels.Alb, albumin; HB, hemoglobin
DISCUSSION
JPS is characterized by hamartomatous polyps in the gastrointestinal tract. Approximately 75% of cases exhibit an autosomal dominant inheritance pattern.^7)^ As most JPS cases are caused by genetic mutations, no curative pharmacological treatments have been established even in the clinical guidelines, as the effectiveness of molecular targeted therapies or prophylactic medications has not been demonstrated.^8)^ Endoscopic polypectomy is recommended for symptomatic lesions, while surgical resection is indicated in cases with invasive carcinoma, intussusception, or when anemia and hypoproteinemia are difficult to control.^3)^ Pharmacological management is generally supportive and symptomatic, including iron supplementation or blood transfusions for anemia, albumin replacement for hypoalbuminemia, and oral nutritional supplements or total parenteral nutrition for malnutrition. In the present case, gastric decompression using a nasogastric tube, blood transfusions, and albumin infusion were performed as part of the preoperative management. In addition, JPS is associated with malignant potential, and in patients with gastric involvement harboring SMAD4 mutations, the risk of developing gastric cancer has been estimated to be as high as 30%.^5,6)^ Therefore, surgical intervention should be considered at the time of diagnosis in appropriate cases. Given the increased risk of postoperative complications, including anastomotic leakage, owing to the poor general condition associated with concurrent anemia and hypoproteinemia, careful perioperative management is essential to ensure patient safety.
We encountered a case of JPS with an SMAD4 mutation that presented with protein-losing gastroenteropathy. As the anemia and hypoproteinemia were refractory to medical treatment and the gastric polyps had increased in size, surgical intervention was considered necessary because of the associated risk of malignant transformation. Surgical options for gastric JPS include both total gastrectomy and partial gastrectomy, depending on the distribution of polyps. In our case, numerous polyps were widely distributed from the cardia to the gastric body, necessitating total gastrectomy. In surgical approaches for gastric JPS, obtaining an adequate surgical field is often challenging because of the difficulty in decompressing a stomach distended with numerous polyps.^9)^ A review of 30 reported cases in Ichushi (Igaku Chuo Zasshi: a Japanese medical literature database) of patients who underwent total gastrectomy for JPS revealed that 13 involved laparoscopic surgery using a 5-port technique^4,9–36)^ (Table 1). Laparoscopic surgery is considered to facilitate access to the entire abdominal cavity with minimal disruption of the abdominal wall compared to open surgery. In cases such as JPS, where the stomach is highly dilated, the advantages of laparoscopic surgery may be particularly significant. In the present case, although the procedure was performed laparoscopically, the stomach was markedly distended and edematous, making visualization challenging. However, by carefully manipulating the thickened gastric wall to secure the operative field, surgery was completed safely without injury or significant bleeding. No established guidelines currently exist for lymph node dissection in cases where gastric cancer is not confirmed preoperatively. However, considering the potential for carcinoma on histopathological examination, D1 lymphadenectomy was performed.
Several reports have described improvements in anemia and hypoproteinemia following surgical intervention, as well as favorable recurrence-free postoperative outcomes in cases of gastric cancer associated with JPS. Previous reports of total gastrectomy for JPS showed that the course of the symptoms was described in 13 among 30 patients, all of whom experienced improvement in postoperative anemia and hypoalbuminemia. However, the follow-up periods ranged from 2 to 24 months, which is shorter than in our patient who had a 48-month follow-up^4,9–36)^ (Table 1). Moreover, previous studies have reported that approximately 27.4% of JPS cases exhibit polyps in both the stomach and intestine.^37)^ Although there are documented cases in which patients underwent gastrectomy with colorectal polypectomy^4)^ or colectomy with gastric endoscopic mucosal resection,^38)^ there have been no reports in Japan of patients undergoing both gastrectomy and colectomy. Regarding gastric cancer, there are case reports documenting recurrence-free survival at 15 months postoperatively.^13)^ In the present case, the patient was followed up for 4 years postoperatively, maintaining stable hemoglobin and serum albumin levels, without symptom exacerbation and with adequate oral intake. Our report represents the longest follow-up demonstrating sustained symptomatic and biochemical improvement among reported cases in Japan. Given that JPS patients remain at risk of developing new polyps and potential malignancies in other parts of the gastrointestinal tract over time, long-term surveillance is therefore essential to monitor for recurrence and to manage nutritional complications such as anemia and hypoalbuminemia, thereby ensuring timely intervention and improved patient outcomes.
CONCLUSIONS
We encountered a case of JPS with an SMAD4 mutation who presented with protein-losing gastroenteropathy and medically refractory anemia and hypoproteinemia, for which laparoscopic total gastrectomy was performed. The patient maintained good nutritional status throughout the long-term postoperative course. Therefore, total gastrectomy may be an effective therapeutic option for symptom control in patients with gastric JPS associated with protein-losing gastroenteropathy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sayed MG, Ahmed AF, Ringold JR, et al. Germline SMAD 4 or BMPR 1A mutations and phenotype of juvenile polyposis. Ann Surg Oncol 2002; 9: 901–6.12417513 10.1007/BF 02557528 · doi ↗ · pubmed ↗
- 2Friedl W, Uhlhaas S, Schulmann K, et al. Juvenile polyposis: massive gastric polyposis is more common in MADH 4 mutation carriers than in BMPR 1A mutation carriers. Hum Genet 2002; 111: 108–11.12136244 10.1007/s 00439-002-0748-9 · doi ↗ · pubmed ↗
- 3Howe JR, Bair JL, Sayed MG, et al. Germline mutations of the gene encoding bone morphogenetic protein receptor 1A in juvenile polyposis. Nat Genet 2001; 28: 184–7.11381269 10.1038/88919 · doi ↗ · pubmed ↗
- 4Yamaguchi Y, Shibata S, Ishiguro M, et al. A case of generalized juvenile gastrointestinal polyposis with protein losing gastropathy. Nihon Rinsho Geka Gakkai Zasshi 2004; 65: 656–60. (in Japanese)
- 5Howe JR, Roth S, Ringold JC, et al. Mutations in the SMAD 4/DPC 4 gene in juvenile polyposis. Science 1998; 280: 1086–8.9582123 10.1126/science.280.5366.1086 · doi ↗ · pubmed ↗
- 6Latchford AR, Neale K, Phillips RK, et al. Juvenile polyposis syndrome: a study of genotype, phenotype, and long-term outcome. Dis Colon Rectum 2012; 55: 1038–43.22965402 10.1097/DCR.0b 013e 31826278 b 3 · doi ↗ · pubmed ↗
- 7Schreibman IR, Baker M, Amos C, et al. The hamartomatous polyposis syndromes: a clinical and molecular review. Am J Gastroenterol 2005; 100: 476–90.15667510 10.1111/j.1572-0241.2005.40237.x · doi ↗ · pubmed ↗
- 8Matsumoto M, Arai M, Iwama T, et al. Japanese Clinical Guidelines 2020 for Diagnosis and Treatment of Juvenile polyposis syndrome in Children and Adults. Journal of Hereditary Tumors 20: 79–92. (in Japanese)