Laparoscopic Management of Long-Standing Gallbladder Hydrops: A Case Report and Literature Review
Ahmed R Zubi, Imran M Adam, Ibrahim S Abdulla, Hawwa Nuha, Abdulla Ubaid

TL;DR
This case report describes a long-standing gallbladder hydrops managed successfully with laparoscopic surgery and highlights the importance of intraoperative decompression.
Contribution
The paper presents a rare case of prolonged gallbladder hydrops and emphasizes the technical aspects of its laparoscopic management.
Findings
Laparoscopic cholecystectomy with intraoperative decompression was effective for long-standing gallbladder hydrops.
Preoperative recognition and decompression are crucial to avoid complications during surgery.
Histopathology confirmed chronic cholecystitis as the underlying condition.
Abstract
Gallbladder hydrops, a condition characterized by distension of the gallbladder with clear serous fluid due to chronic outflow obstruction, is an uncommon clinical entity most often associated with cholelithiasis. It poses a diagnostic and therapeutic challenge, as it can present with a wide spectrum of symptoms, from being an incidental finding to mimicking other abdominal pathologies. This case report illustrates the clinical course of a patient with long-standing, intermittently symptomatic gallbladder hydrops. A 63-year-old woman presented with a four-year history of intermittent right upper quadrant pain. Imaging three years prior (ultrasound and CT) had confirmed the diagnosis of gallbladder hydrops with an impacted stone in the cystic duct. She deferred surgery at that time. Upon re-presentation, imaging revealed a persistently distended gallbladder. She successfully underwent a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1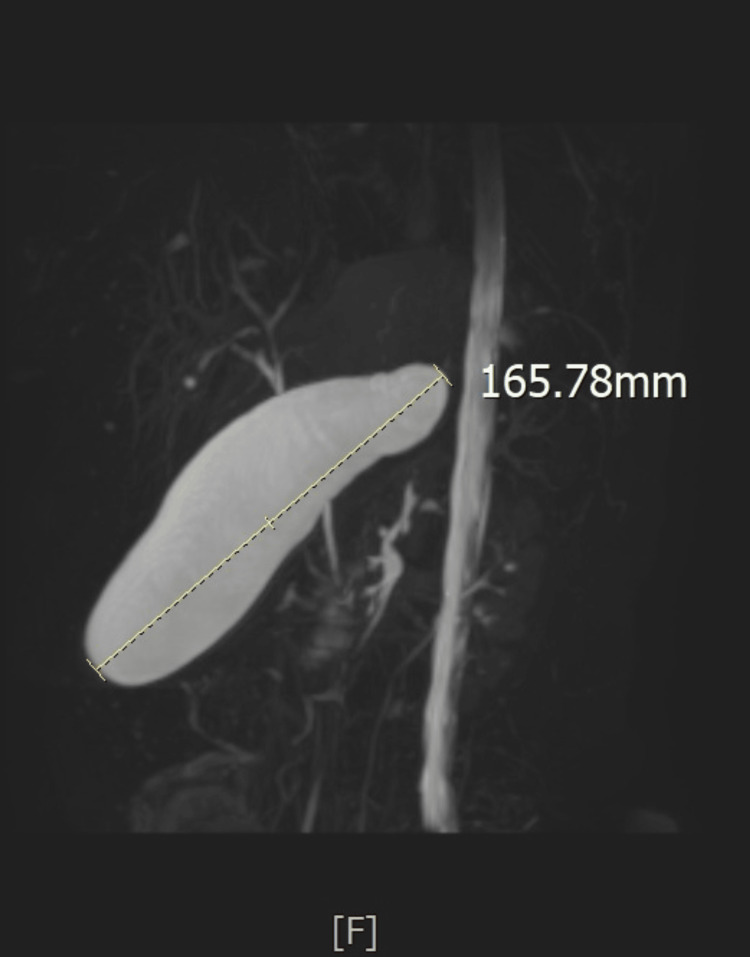 Figure 2
Figure 2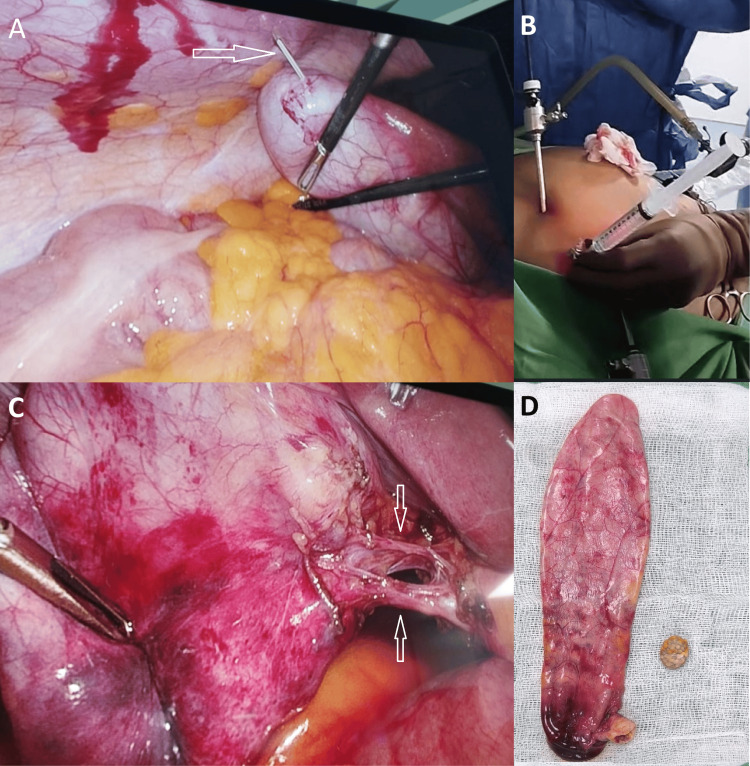 Figure 3
Figure 3| Parameter | Three years prior to surgery | 15 days prior to surgery | Reference Value |
| Hemoglobin | 13.6 g/dL | 12.9 g/dL | 10.6 - 13.5 g/dL |
| White cell count | 8.14 109/L | 9.47 109/L | 4.37 - 9.68 109/L |
| Platelet | 237 109/L | 257 109/L | 186 - 353 109/L |
| Urea | 23.54 mg/dL | 25.68 mg/dL | 15 - 40 mg/dL |
| Creatinine | 0.82mg/dL | 0.81 mg/dL | 0.57 - 1.11 mg/dL |
| Serum sodium | 142 mmol/L | 140 mmol/L | 136 - 145 mmol/L |
| Serum potassium | 4.4 mmol/L | 4.3 mmol/L | 3.5 - 5.1 mmol/L |
| Total bilirubin | 0.8 mg/dL | 0.4 mg/dL | 0.2 - 1.2 mg/dL |
| Albumin | 5 g/dL | 4.5 g/dL | 3.5 - 5.2 g/dL |
| Alkaline phosphatase | 49 U/L | 95 U/L | 40 - 150 U/L |
| aspartate aminotransferase | 33 U/L | 51 U/L | 5.0 - 34 U/L |
| alanine aminotransferase | 62 U/L | 62 U/L | 0 - 55 U/L |
| Gamma-glutamyl transferase | 23 U/L | 36 U/L | 9.0 - 36 U/L |
| Fasting Blood Glucose | 98 mg/dL | 111 mg/dL | 60 - 139 mg/dL |
| Lipase | - | 42.78 U/L | 8 - 78 U/L |
| Case report (Author, Year) | Age/Gender | Presenting symptoms | Duration of symptoms | First diagnostic image | Stone size | Gallbladder length | Fluid description | Treatment received |
| Tan et al., 2025 [ | 18/Female | Acute cholecystitis | 2 days | CT | Not mentioned | 145 mm | Not mentioned | Laparoscopic cholecystectomy |
| Haji et al., 2023 [ | 28/Male | Gastric outlet obstruction | 2 years | Ultrasound | No stone | 149 mm | Purulent mucoid bile | Open subtotal cholecystectomy |
| Sharma et al., 2021 [ | 50/Female | Right hypochondrial pain | 3 days | CT | Not mentioned | Not mentioned | - | Not mentioned |
| Le et al., 2023 [ | 56/Female | Abdominal discomfort and nausea | 4 days | Ultrasound | Not mentioned | 217 mm | Clear mucous-like fluid | Laparoscopic cholecystectomy |
| Viswanathan and Cheng, 2012 [ | 84/Female | Abdominal discomfort, weight loss, and jaundice | No mentioned | Ultrasound | No stones | 120 mm | - | Conservative |
| Viswanathan et al., 2012 [ | 83/Male | Asymptomatic | - | MRCP | Not mentioned | Not mentioned | - | Conservative |
| Loh et al. 2019 [ | 63/Male | Gastric outlet obstruction | 6 months | CT | 10 mm | 98 mm | White mucoid bile | Open cholecystectomy |
| Adhikari et al., 2024 [ | 79/Male | Dark urine and pale stool | 1 week | CT | No stone | 102 mm | Not mentioned | Laparoscopic cholecystectomy |
| Amarnath et al., 2019 [ | 78/Male | Epigastric pain | 1 day | CT | No stone | 110 mm | Not mentioned | Laparoscopic subtotal cholecystectomy |
| Reyes et al., 2017 [ | 39/Female | Acute cholecystitis | 4 days | Ultrasound | 6.9 mm | 139 mm | Not mentioned | Laparoscopic cholecystectomy |
| Yadav and Kankaria, 2017 [ | 46/Female | Right hypochondrial pain | Not mentioned | Ultrasound | 10.6 mm | 300 mm | Not mentioned | Laparoscopic cholecystectomy |
| Poget et al., 2024 [ | 51/Female | Right hypochondrial pain | 6 months | Ultrasound | 6 mm | 110 mm | Whitish mucus | Laparoscopic cholecystectomy |
| Ganta et al., 2022 [ | 67/Female | Acute cholecystitis | 4 days | Ultrasound | Not mentioned | 170 mm | Not mentioned | Laparoscopic cholecystectomy |
| Mvoula et al., 2023 [ | 42/Female | Acute cholecystitis | 7 days | Ultrasound | 15 mm | 155 mm | Not mentioned | Laparoscopic cholecystectomy |
| Ercihan et al., 2022 [ | 26/Female | Upper abdominal pain and indigestion | 2 years | Ultrasound | 14 mm | 75 mm | Mucoid material | Laparoscopic cholecystectomy |
| Ercihan et al., 2022 [ | 34/Female | Upper abdominal pain and nausea | 1 months | Not done | No stones | 70 mm | Mucus | Laparoscopic cholecystectomy |
| Valecha et al., 2019 [ | 27/Female | Abdominal pain, vomiting | 3 days | Ultrasound | Not mentioned | 85 mm | Whitish material | Laparoscopic cholecystectomy |
| Our case | 63/Female | Intermittent right hypochondrial pain | 4 years | Ultrasound | 13 mm | 145 mm | Clear serous fluid | Laparoscopic cholecystectomy |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments · Cholangiocarcinoma and Gallbladder Cancer Studies
Introduction
Gallbladder hydrops is a benign condition resulting from a prolonged blockage of the gallbladder outflow, which leads to its filling with clear serous fluid. It most commonly occurs due to an impacted stone in the gallbladder neck or cystic duct [1]. Other possible causes include cystic duct fibrosis, tumors (of the gallbladder or cystic duct), certain parasitic infections, external compression, and motility disorder [2]. With prolonged obstruction, the bile salts are absorbed, and the bile is replaced with a clear serous fluid. The gallbladder distends to various degrees, and volumes of up to 1500 ml have been reported [3].
As gallbladder hydrops is primarily a complication of cholelithiasis, it occurs most commonly in middle-aged women [3]. It usually follows an episode of acute cholecystitis, which may resolve, but the blockage of the cystic duct persists, resulting in chronic intermittent pain and bloating [4]. In some instances, it may be discovered incidentally [5]. It can also present with unusual symptoms such as lower abdominal pain, urinary frequency, gastric outlet obstruction, or Mirizzi’s syndrome [1,4,6,7]. More serious complications, such as empyema or perforation, may also occur [8].
Laboratory results are often within the reference range for uncomplicated cases. Abdominal ultrasound, computed tomography (CT), or magnetic resonance cholangiopancreatography (MRCP) typically reveal a distended gallbladder, commonly with associated cholelithiasis [9]. Laparoscopic cholecystectomy is the standard treatment for gallbladder hydrops. However, the procedure becomes more technically challenging with an increasing risk of perforation [10]. Percutaneous drainage serves as an alternative for acutely ill patients, acting as a bridge to definitive surgery [6].
We present the case of a middle-aged woman with long-standing gallbladder hydrops who had intermittent symptoms and was treated with laparoscopic cholecystectomy. A comparative review of the literature on its characteristics, clinical features, diagnostic imaging, and treatment is also provided.
Case presentation
A 63-year-old woman presented to the surgical OPD as a known case of gallbladder hydrops, diagnosed three years prior. For four years, she had occasional episodes of right upper abdominal pain, characterized as mild, dull, radiating to the upper back and suprapubic area. The pain was precipitated by heavy meals or prolonged fasting and was relieved spontaneously or with simple analgesics.
Three years prior to her presentation, she sought medical advice for urinary symptoms. An abdominal ultrasound revealed a distended gallbladder with multiple stones, including one impacted stone at the neck, with high suspicion of a hydropic gallbladder. This was followed by an abdominal CT, which confirmed the diagnosis (Figure 1). The laboratory investigations were within the reference range (Table 1). She was offered laparoscopic cholecystectomy but deferred the surgery due to social reasons.
Abdominal CT at the first presentationAbdominal CT from the first presentation (three years before the cholecystectomy detailed in this case report) showing a distended gallbladder.
During this three-year period, she experienced mild episodes of pain that resolved spontaneously or with basic analgesics without requiring medical consultation. However, one year prior to presentation, the pain became more frequent and was associated with nausea and anorexia. A systematic review was positive only for chronic constipation. She denied fever, vomiting, dark urine, pale stools, fatigue, or weight loss. She is a known case of diabetes mellitus and dyslipidemia, diagnosed during her initial presentation three years ago, and was started on oral medication. Apart from a cesarean section performed over 20 years ago, she has no history of other surgical interventions and no significant family history.
Physical examination revealed an overweight woman who was hemodynamically stable. Her abdomen was flabby, soft, and non-tender, with no palpable gallbladder. Laboratory findings were within normal limits (Table 1). Abdominal ultrasound demonstrated a 13-mm stone impacted in the cystic duct, causing gallbladder dilatation. Magnetic resonance cholangiopancreatography (MRCP) confirmed these findings and showed a normal biliary tree and pancreas (Figure 2).
MRCP at second presentationMagnetic resonance cholangiopancreatography (MRCP) from the second presentation (two weeks before the cholecystectomy detailed in this case report) showing a distended gallbladder.
The patient underwent a laparoscopic cholecystectomy, which revealed a distended, elongated gallbladder that was difficult to grasp and was assigned a Parkland Grading Scale grade of 3 (Figure 3A). We therefore performed percutaneous decompression using a 16-gauge cannula, aspirating approximately 125 mL of clear fluid (Figure 3A, 3B). The remainder of the procedure was uneventful. The patient was discharged on postoperative day 1 and remained asymptomatic at her two-week follow-up appointment. Histopathology came back as chronic cholecystitis. The gallbladder was 145 mm long, and the wall thickness was 2 mm.
Intraoperative finding during cholecystectomyA: Percutaneous aspiration of distended gallbladder (white arrow), B: Aspirated clear fluid in syringe, C: Cystic duct (lower arrow) and cystic artery (upper arrow), D: the gallbladder and the impacted stone.
Discussion
Gallbladder hydrops in humans is underreported in the literature and lacks large-scale studies to deeply analyze its risk factors and potential complications. Most of the available information comes from animal studies [11,12]. Murtaza Khomusi et al. reported one case (0.4%) among the cases they collected over two years. Khan et al., in their 26-year experience, encountered 216 mucoceles, constituting 4.2% of the total number of cholecystectomies performed. Similarly, Shirah et al. reported 57 cases (5.8%) over 10 years [12-14]. Gallbladder hydrops is a condition that most surgeons will encounter in their careers. That said, its definition is loosely applied. In this literature review, seven of the 14 case reports involving gallbladder removal did not describe the filling fluid and focused only on size (Table 2) [1,7-10,15,16]. The remaining reports described the fluid as clear, white, or purulent mucus or mucoid material (Table 2).
The majority of case reports use "gallbladder hydrops" and "gallbladder mucocele" interchangeably. However, a more nuanced distinction is highlighted in several reports. They posit that a hydropic gallbladder results from chronic cystic duct obstruction, leading to the accumulation of a watery, serous fluid. A mucocele, in contrast, is defined by mucinous hyperplasia of the gallbladder epithelium and an overproduction of mucus, which is also accompanied by obstruction [11]. Furthermore, some cases involve mucinous metaplasia without physical obstruction, while hydrops can develop in the absence of stones, potentially due to a functional obstruction of the gallbladder outlet [2,7,8,11]. All these factors should be considered when describing gallbladder hydrops.
Our case involves a 63-year-old woman with a long-standing hydropic gallbladder, which was intermittently symptomatic, radiologically confirmed, and ultimately treated with laparoscopic cholecystectomy and intraoperative decompression. The gallbladder was distended with clear watery fluid due to a stone impacted in the neck. The absence of mucinous hyperplasia on histopathology confirms the diagnosis of hydrops rather than mucocele. The chronic presentation, diagnostic definition, and successful surgical outcome provide several reference points for comparison with similar cases in the literature.
The most common cause of gallbladder hydrops is cholelithiasis, as seen in this case. Other possible causes of gallbladder outflow obstruction include benign or malignant polyps, cystic duct fibrosis, external compression from either liver parenchyma or perihilar lymphadenopathy, intraluminal parasites, or functional disorders [2,7].
Hydropic gallbladder has been reported in all age groups (though the pediatric population was not included in this literature review) and is more common in females (Table 2). Its presentation ranges from an incidental finding to chronic pain to acute conditions such as acute cholecystitis [5,7,11,17]. Our patient presented with chronic intermittent pain but no systemic inflammatory symptoms and had normal liver function tests. Older patients tend to present with chronic symptoms or may even remain asymptomatic, and may have had the condition for many years before diagnosis [4]. Interestingly, some patients develop atypical manifestations such as right lower quadrant pain or urinary symptoms, resulting from mechanical compression of nearby structures by the hydropic gallbladder [1,4]. Our patient also initially presented with urinary symptoms, similar to the case reported by Le et al. [4].
Although some cases of gallbladder hydrops may remain asymptomatic for long periods, particularly in elderly patients, most cases present with symptoms, and some may even develop complications. In our patient, the gallbladder size did not increase significantly despite three years of observation, though she experienced intermittent pain or discomfort. Potential complications primarily arise from the compression of adjacent structures, leading to Mirizzi syndrome or gastric outlet obstruction. Additionally, empyema may develop, and in rare cases, perforation can occur [2,6-8]. Although these complications are considered uncommon - as evidenced by Shirah et al.'s series of 57 cases, over 10 years, without any - our review of 17 case reports revealed two instances of gastric outlet obstruction, one of Mirizzi syndrome, and one perforation [12].
This higher rate is likely skewed, as case reports have an inherent bias toward publishing complicated presentations. Another potential complication is malignant transformation. This is more likely with a mucocele due to the associated epithelial hyperplasia and metaplasia, which carry a risk of dysplasia and can lead to carcinoma. The incidence of gallbladder cancer in cholecystectomy specimens has been reported to be around 1.5%. Additionally, the presence of the mucocele or the gallbladder hydrops can be secondary to gallbladder neoplasm [11].
The longest reported gallbladder measured 300 mm [10]. In our literature review, gallbladder size ranged from 70 to 300 mm, with a median of 115 mm (Table 2). White mucus was observed even in gallbladders of normal size (70-100 mm) [2,17]. Only six case reports specified the size of the impacted stone, which ranged from 6 mm to 15 mm [6,9-11,16,17], while five case reports documented no stones [2,5,7,8,17].
Most cases of gallbladder hydrops can be diagnosed via abdominal ultrasound. However, a CT scan or MRCP is often performed to better characterize the condition, rule out other pathologies, or when ultrasound findings are limited (e.g., due to obesity or bowel gas) [9]. In five cases, CT scans were the initial imaging study because the diagnosis was unclear, and the hydropic gallbladder was not suspected and discovered after imaging (Table 2). In our patient, gallbladder hydrops was initially detected on ultrasound. Nevertheless, an abdominal CT was obtained during the first presentation, while an MRCP was obtained during the second presentation. These additional imaging modalities allowed for further assessment of gallbladder size and confirmed the absence of bile duct stones or anatomical abnormalities.
The standard treatment for gallbladder hydrops is cholecystectomy. This approach is justified by the frequent presence of symptoms, the risk of complications (including gallbladder rupture), and the potential for malignant transformation in longstanding mucoceles due to epithelial metaplasia [11]. Conservative management may be considered in asymptomatic elderly patients when the risks of surgery outweigh the potential complications, but the long-term outcome has not been studied, and the possible complications should be discussed carefully with the patient [5]. In the reported cases (Table 2), cholecystectomy was performed in all but three instances: one patient was referred for surgery, while the other two were elderly with minimal symptoms and were managed conservatively [3,5].
Although gallbladder hydrops can complicate laparoscopic cholecystectomy, the procedure was successfully completed in most cases (Table 2). Two cases required conversion to open cholecystectomy - one due to encapsulated peritonitis and the other due to dense adhesions [2,6]. Laparoscopic cholecystectomy was successfully performed by Shirah et al. in all 57 of their reported cases [12]. Percutaneous cholecystostomy serves as a temporary measure to decompress the gallbladder, alleviate symptoms, and stabilize patients, either as a bridge to surgery or in high-risk individuals. Endoscopic ultrasound-guided drainage is an alternative minimally invasive option [12].
One of the challenges in operating on gallbladder hydrops is the distended gallbladder, which is difficult to manipulate and carries a risk of rupture; therefore, Intraoperative decompression - via laparoscopic needle aspiration or percutaneous cannula - is often needed but risks bile spillage. To mitigate this, some surgeons place a figure-of-eight suture around the puncture site for immediate closure after aspiration. Notably, only four reported cases mention gallbladder decompression, none of which specify the technique used [2,4,6,15]. However, Shirah et al. performed percutaneous drainage for all reported cases without complications and recommended it to ensure safe laparoscopic cholecystectomy in gallbladder hydrops [12]. We aspirated the gallbladder contents via a 16-gauge cannula introduced through the abdominal wall into the fundus of the gallbladder under laparoscopic guidance. After decompression, the puncture site was secured with a gallbladder grasper to minimize spillage.
Conclusions
Gallbladder hydrops, primarily caused by cystic duct obstruction from an impacted stone, leads to the absorption of bile and accumulation of sterile "white bile." While well-documented in animals, it is underreported in humans and presents a diagnostic challenge due to its highly variable presentation, from being asymptomatic to causing chronic pain or atypical compressive symptoms. Abdominal ultrasound is the key initial diagnostic tool, though CT or MRCP are often essential for confirmation, detailed anatomical mapping, and excluding other pathologies or malignancies before surgical intervention.
Laparoscopic cholecystectomy remains the definitive treatment for symptomatic cases. However, the surgery is technically challenging due to the large, tense gallbladder, which increases the risk of intraoperative perforation. Therefore, strategic intraoperative decompression is a crucial and often necessary step to safely collapse the organ and facilitate dissection. A successful outcome hinges on preoperative recognition of this condition and meticulous surgical planning.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A case report of hydropic gallbladder presenting as right lower quadrant abdominal pain J Educ Teach Emerg Med Tan S Adams Z Rudkin S Matonis D 0610202510.21980/J 8DD 26PMC 1205407440336690 · doi ↗ · pubmed ↗
- 2A rare case of ‘gastric outlet obstruction secondary to hydrops of gallbladder’ caused by recurrent acalculous cholecystitis: a variant of Bouveret’s syndrome - a rare case and review of literature Surg Gastroenterol Oncol Haji AG John AR Elhassan A Zohdy M Haider SI Lourdusamy S Piramanayagam B 243247282023
- 3Gallbladder hydrops Cureus Sharma R Stead TS Aleksandrovskiy I Amatea J Ganti L 013202110.7759/cureus.18159 PMC 853050234703693 · doi ↗ · pubmed ↗
- 4A rare case of calculous gallbladder hydrops presenting with atypical abdominal and urinary symptoms Cureus Le ZH Dowling L Ranasinghe SM 015202310.7759/cureus.40016 PMC 1032315237425591 · doi ↗ · pubmed ↗
- 5Management of hydrops gallbladder in the elderly: 806Off J Am Coll Gastroenterol ACG Viswanathan P Cheng E 01072012 https://journals.lww.com/ajg/fulltext/2012/10001/management_of_hydrops_gallbladder_in_the_elderly_.806.aspx
- 6Rare case of gallbladder mucocele causing gastric outlet obstruction treated with cholecystectomy Int J Surg Case Rep Loh WL Ng NZ Kabir T Chan CY 84875720193092544910.1016/j.ijscr.2019.03.013PMC 6439269 · doi ↗ · pubmed ↗
- 7Hydrops gallbladder caused by cystic duct fibrosis leading to Mirizzi syndrome: a case report Cureus Adhikari B Nieto LM Adhikari B Dhital A Attar C 016202410.7759/cureus.68328 PMC 1144204039350813 · doi ↗ · pubmed ↗
- 8Spontaneous perforation of an acalculous hydropic gallbladder in a diabetic patient with neuropathy: an underdiagnosed entity Gastroenterology Res Amarnath S Polavarapu AD Gumaste V 3153191220193180331210.14740/gr 1226 PMC 6879033 · doi ↗ · pubmed ↗