A Decade With Sheehan's Syndrome: A Case Report and Personal Experience
Kayalvizhi D., Adedeji Yusuf Moradeyo, Bhuvaneswari G.

TL;DR
This case report describes a woman's long-term experience with Sheehan's syndrome, a rare pituitary disorder following childbirth, highlighting diagnostic delays and management challenges.
Contribution
The paper contributes a detailed case report emphasizing the importance of early diagnosis and multidisciplinary management of Sheehan's syndrome.
Findings
Delayed diagnosis of Sheehan's syndrome led to prolonged hormonal deficiencies and persistent symptoms.
Lifelong hormone replacement therapy and frequent dose adjustments are necessary for managing endocrine dysfunction.
Multidisciplinary collaboration improves outcomes and reduces diagnostic delays in postpartum patients with SS.
Abstract
Sheehan's syndrome (SS) is a rare endocrine disorder caused by ischemic necrosis of the anterior pituitary gland secondary to massive postpartum hemorrhage (PPH) and shock. It commonly leads to multiple hormonal deficiencies, such as adrenal insufficiency, hypothyroidism, and hypopituitarism. Affected individuals may present with signs and symptoms including weight gain or loss, cold intolerance, hair loss, menstrual irregularities, and hypotension. Diagnosis is often delayed due to its nonspecific presentation and overlap with conditions like postpartum depression and chronic fatigue syndrome. This case report highlights the clinical presentation, management challenges, and complications associated with the delayed diagnosis of SS. A 35-year-old female was diagnosed with SS in 2016, at the age of 26, following severe PPH and hemorrhagic shock after a vaginal delivery in 2013.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
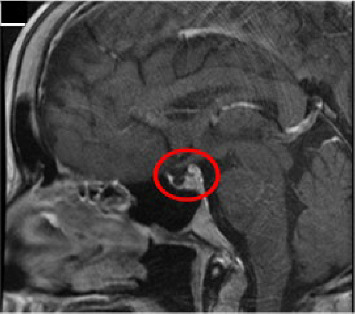 Figure 1
Figure 1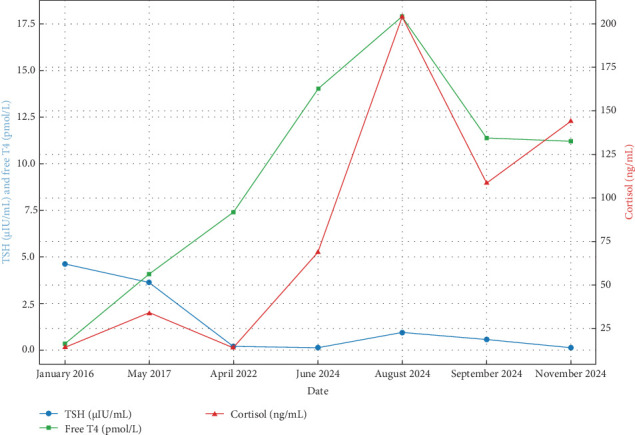 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological diseases and metabolism
1. Introduction
Sheehan's syndrome (SS) results from ischemic necrosis of the anterior pituitary gland secondary to severe postpartum hemorrhage (PPH). The anterior pituitary is supplied by a low-capacity portal venous system, making it more susceptible to vascular compromise. Following hemorrhage, reduced perfusion of oxygen and nutrients leads to ischemia, cellular necrosis, and subsequent deficiency of anterior pituitary hormones. The typical sequence of hormonal loss, reflecting the differential vulnerability of cell types, is: growth hormone → prolactin → TSH → ACTH → LH/FSH [1].
In contrast, the posterior pituitary gland is rarely affected, as it receives a direct arterial blood supply, making it more resistant to ischemic damage. However, in uncommon cases, diabetes insipidus may occur due to antidiuretic hormone (ADH) deficiency, which may be suggested by the presence of polyuria in this patient.
SS is often underdiagnosed, as its clinical features can mimic postpartum depression, chronic fatigue, or psychological stress [2]. This case underscores the diagnostic challenges of late recognition [3] and highlights the lifelong hormonal deficiencies, fertility issues [4], and the complexity of managing multiple endocrine deficits.
2. Case Presentation
A 35-year-old female was diagnosed with Sheehan's Syndrome three years after experiencing severe PPH and hemorrhagic shock following a vaginal delivery in 2013. Initially, she presented with nonlactation and profound fatigue, followed by amenorrhea, hair loss, weight changes, hypotension, mood swings, and frequent urination (Table 1). These symptoms were attributed to postpartum depression for several years, which delayed the correct diagnosis and management. Over time, her symptoms worsened, prompting consultations with multiple specialists, including urologists, gynecologists, and endocrinologists (Table 2).
In 2016, at the age of 26, she was diagnosed with SS after an extensive endocrine work-up. This included serial measurements of cortisol, thyroid function tests, sodium levels, and vitamin D status, providing insights into her hormonal profile. Magnetic resonance imaging (MRI) of the brain (sella protocol) revealed a partial empty sella, with residual pituitary tissue and loss of the posterior pituitary bright spot, confirming the diagnosis (Figure 1).
She was initiated on lifelong hormone replacement therapy (HRT) for adrenal insufficiency (hydrocortisone 30 mg/day), hypothyroidism (thyroxine 100 mcg/day), and hypogonadism (estrogen [Progynova 10 mg/day] and progesterone [Naturogest 200 mg/day]). Ovulation was induced using human chorionic gonadotropin (HCG) and human menopausal gonadotropin (HMG) injections, resulting in a successful conception.
During pregnancy, she developed an adrenal crisis, presenting with multiple episodes of severe vomiting, which required intravenous hydrocortisone administration—a known complication of adrenal insufficiency during pregnancy in SS. Although the postpartum period remained stable, lifelong endocrine surveillance remains essential.
The patient is highly sensitive to fluctuations in hydrocortisone and thyroxine doses as reflected in hormonal variability (Figure 2), often experiencing fatigue, hair loss, low libido, mood disturbances (e.g., irritability, anxiety, and sadness), palpitations, and excessive sweating. She also reports bone pain, osteoporosis, and gastrointestinal side effects such as chronic gastritis, likely due to long-term hydrocortisone therapy (Table 1).
Despite partial improvement, regular hormonal monitoring and medication adjustments have been necessary over a 9-year follow-up period to maintain physiologic hormone levels. She currently undergoes blood tests every 3 months, adjusting doses as needed to limit adverse effects (Table 3). Persistent symptoms such as fatigue, hair thinning, low libido, and intermittent palpitations continue to require attention. These ongoing effects significantly impact her quality of life, underscoring the importance of early diagnosis, timely treatment, and long-term endocrine follow-up.
3. Discussion
Postpartum hypopituitarism can result from several conditions, including SS, a rare but serious disorder caused by ischemic necrosis of the pituitary gland [5] following poorly managed severe PPH. The incidence of SS has significantly decreased in developed countries [6] due to improved obstetric care. However, delayed diagnosis remains a major challenge, often due to nonspecific symptoms, late presentation, and misattribution to alternative conditions. Unless patients present early with lactation failure after PPH, symptoms may evolve slowly over months to as long as 10 years, leading to long-term endocrine complications. In many cases, SS is misdiagnosed as postpartum depression, which can significantly delay appropriate management [7]. This delay was evident in the present case, where the diagnosis was made 3 years after delivery.
Although rare in high-resource countries, SS remains a diagnostic challenge in low- and middle-income regions. Studies from India, Africa, and Latin America report diagnostic delays of 5–10 years due to overlapping symptoms with other postpartum disorders, limited endocrine follow-up, and low awareness among healthcare providers [1, 7]. In developed countries, better MRI availability has reduced delays, yet subtle or partial cases may still be overlooked, highlighting the importance of early screening protocols. There are minimal regional data from island nations like Seychelles, making this report an important contribution to the limited literature. The longitudinal follow-up, documentation of treatment responsiveness, and reproductive outcomes in this case provide valuable insight into patient-centered management in underrepresented settings.
SS may present as partial or complete hypopituitarism, with deficiencies in anterior pituitary hormones such as ACTH, thyroid hormones, prolactin, gonadotropins, and growth hormone [8, 9].
The term “SS” refers to pituitary hypofunction arising from ischemic necrosis of the anterior pituitary gland secondary to massive PPH. Risk factors for postpartum hypopituitarism include disseminated intravascular coagulation (DIC), hemophilia, thrombocytopenia, and other bleeding disorders. Clinicians should also be aware of nonobstetric causes such as radiation therapy, empty sella Syndrome, traumatic brain injury, pituitary tumors, neurosurgery, and systemic infections like sepsis. These may mimic SS clinically but differ in etiology and treatment approach.
Characteristic clinical features of SS include failure to lactate, persistent amenorrhea, chronic fatigue, weight changes, and hypotension [10]. Most of these are nonspecific, often leading to misinterpretation as normal postpartum changes or psychiatric conditions [11]. Gradual symptom onset further complicates timely recognition. This case illustrates that even in the presence of severe hemorrhagic shock during delivery, significant hormonal deficiencies may be missed initially, delaying endocrine evaluation (Table 2) [12].
Diagnosis relies on clinical suspicion, laboratory assessment, and imaging studies. Hormonal evaluation should include cortisol, ACTH, TSH, free T4, LH, FSH, and prolactin [13, 14], as deficiencies are common. In this patient, low cortisol and thyroid hormone levels confirmed multiple anterior pituitary hormone deficiencies (Table 3). MRI demonstrated partial empty sella, supporting ischemic pituitary damage [13, 15, 16].
A recent case report detailed a rare and severe presentation of SS diagnosed 6 years after childbirth, in which the patient developed an adrenal crisis, profound hypothyroidism, and massive pericardial effusion as a result of longstanding anterior pituitary insufficiency [17]. This case underscores the potentially life-threatening consequences of delayed recognition and highlights the critical importance of maintaining a high index of suspicion for SS in postpartum women presenting with nonspecific or evolving symptoms. Timely diagnosis and appropriate hormone replacement therapy (HRT) are essential to prevent such serious complications and improve long-term outcomes.
Management of SS requires lifelong HRT. Glucocorticoid replacement with hydrocortisone is essential not only to treat adrenal insufficiency but also to prevent adrenal crisis, especially during stress, illness, or pregnancy. Levothyroxine is used for hypothyroidism [18, 19], and estrogen/progesterone therapy for gonadal failure helps prevent long-term complications such as osteoporosis [20–22] and cardiovascular disease [23]. In this case, frequent dose adjustments were required due to persistent symptoms, illustrating the variability in individual hormone dose responses and the importance of personalized care.
Long-term complications of SS and its treatment include decreased bone mineral density, cardiovascular risks, metabolic disturbances, and psychiatric symptoms [24]. Chronic glucocorticoid therapy increases osteoporosis risk, warranting bone density monitoring and calcium/vitamin D supplementation [21, 22]. Patients frequently report fatigue, mood swings, night sweats, and reduced libido [25–28]. This patient also experienced chronic gastritis, a gastrointestinal side effect of prolonged corticosteroid use [29].
Fertility depends on the extent of pituitary damage. Partial SS may allow near-normal fertility, whereas complete SS significantly impairs reproductive capacity. Amenorrhea and menstrual irregularities are early signs of gonadotropin deficiency. With appropriate HRT, patients can regain reproductive potential and pursue pregnancy. Individualized reproductive counseling is important, taking into account cultural expectations and the emotional impact of infertility.
Women with SS who become pregnant require multidisciplinary monitoring. Pregnancy carries risks, particularly adrenal crisis due to increased hormonal demands. Hydrocortisone dosage should be adjusted during pregnancy and labor to prevent life-threatening complications. With coordinated care involving endocrinologists and obstetricians, favorable maternal and fetal outcomes are possible.
Maternal hormone stability is crucial for fetal growth and neurodevelopment. Poorly controlled maternal hypothyroidism may lead to neurocognitive and developmental delays in the fetus, while prolactin deficiency can result in postpartum lactation failure, depriving the newborn of colostrum, which is vital for neonatal immunity and nutrition.
In some cases, ovulation induction using HCG and HMG injections can restore fertility and lead to successful conception [30]. In this patient, pregnancy was complicated by adrenal crises, necessitating intravenous glucocorticoid therapy, which highlights the importance of adjusting steroid doses during pregnancy to meet increased physiological demands [31].
The integration of emerging technologies, such as wearable hormone monitors and mobile applications, may support real-time hormone tracking and dose optimization, particularly during pregnancy and other vulnerable periods. Existing literature supports a multidisciplinary management approach, involving endocrinologists, obstetricians, and reproductive specialists, to optimize outcomes for both mother and child [32].
Severe PPH, especially when inadequately managed, should raise a high index of suspicion for SS in postpartum women with persistent fatigue, amenorrhea, and lactation failure [32, 33]. This case adds novel patient-specific perspectives, as the patient is also the author, offering a unique narrative medicine dimension. Her case emphasizes diagnostic delays, treatment challenges, psychosocial burdens, and the need for micro-adjustments in hormone dosing. It also highlights the value of longitudinal hormone tracking and the potential of emerging technologies such as wearable and AI-assisted monitoring systems. For instance, the U-RHYTHM system enables continuous cortisol profiling to personalize steroid dosing [34], while wearable nano biosensors now allow noninvasive estradiol monitoring via sweat [35]. Consumer-grade ovulation-tracking wearables are also gaining clinical relevance [36], supporting the integration of mobile apps and AI tools into reproductive care. These advancements, combined with a “Postpartum Endocrine Red Flag Checklist,” may facilitate earlier diagnosis and safer outcomes for high-risk women.
4. Conclusion
This report narrates the challenges and consequences of delayed diagnosis in SS, a rare but significant cause of postpartum hypopituitarism [37, 38]. The delay in diagnosis, despite classic features such as fatigue, amenorrhea, and failure to lactate [39, 40] following severe PPH, emphasizes the critical need for heightened clinical vigilance. These symptoms should not be attributed solely to postpartum changes or psychiatric conditions without a comprehensive endocrine evaluation. This case reinforces that the timely diagnosis of SS can significantly reduce long-term morbidity and improve patient outcomes.
Considering the complexity of lifelong HRT [41–43], this case report underscores the potential benefits of technology-based medical support, such as digital hormone monitoring systems or AI-based decision tools for dose optimization.
This case also brings attention to the reproductive challenges in women with SS. The successful conception following ovulation induction and the management of adrenal crises during pregnancy illustrate the importance of coordinated care involving endocrinologists, obstetricians, and fertility specialists [44, 45]. These insights support the integration of innovative healthcare technologies, such as wearable hormone trackers and mobile alert systems, to enhance patient safety during pregnancy.
Importantly, this report demonstrates the value of incorporating patient perspectives in clinical literature. As both subject and author, the patient offers a unique narrative that enriches clinical insight and humanizes medical understanding. This emphasizes the role of narrative medicine in supporting empathetic, patient-centered care.
Ultimately, this case advocates for a multidisciplinary, proactive, and personalized approach to SS. Routine postpartum endocrine screening in high-risk individuals, continuous provider education, and technology-driven care strategies are critical to reduce diagnostic delays and enhance the quality of life. The lessons from this case aim not only to improve clinical care but also to lay the foundation for future research, innovation, and policy development in the management of postpartum endocrine disorders.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Keleştimur F. Sheehan’s Syndrome Pituitary 20036418118810.1023/B:PITU.0000023425.20854.8e 2-s 2.0-314274372815237929 · doi ↗ · pubmed ↗
- 2Qadri M. I. Mushtaq M. B. Qazi I. Yousuf S. Rashid A. Sheehan’s Syndrome Presenting as Major Depressive Disorder Iranian Journal of Medical Sciences 2015401737625648343 PMC 4300485 · pubmed ↗
- 3Diri H. Karaca Z. Tanriverdi F. Unluhizarci K. Kelestimur F. Sheehan’s Syndrome: New Insights Into an Old Disease Endocrine 2016511223110.1007/s 12020-015-0726-32-s 2.0-8495383588826323346 · doi ↗ · pubmed ↗
- 4Saxena S. Verma V. Samadarshi S. Dorji T. Muthukrishnan J. Delayed Sheehan’s Syndrome Diagnosed During the Evaluation of Secondary Infertility: A Case Report Clinical Case Reports 202412210.1002/ccr 3.8521 e 8521 PMC 1085304938344342 · doi ↗ · pubmed ↗
- 5Shivaprasad C. Sheehan’s Syndrome: Newer Advances Indian Journal of Endocrinology and Metabolism 2011157 S 203S 20710.4103/2230-8210.8486922029025 PMC 3183525 · doi ↗ · pubmed ↗
- 6Karaca Z. C. Laway B. A. Dokmetas H. S. Atmaca H. Kelestimur F. Sheehan Syndrome Nature Reviews Disease Primers 20162111510.1038/nrdp.2016.922-s 2.0-8500697862028004764 · doi ↗ · pubmed ↗
- 7Ramiandrasoa C. Castinetti F. Raingeard I. Delayed Diagnosis of Sheehan’s Syndrome in a Developed Country: A Retrospective Cohort Study European Journal of Endocrinology 2013169443143810.1530/EJE-13-02792-s 2.0-8488488948623864341 · doi ↗ · pubmed ↗
- 8Goswami R. Kochupillai N. Crock P. A. Jaleel A. Gupta N. Pituitary Autoimmunity in Patients With Sheehan’s Syndrome The Journal of Clinical Endocrinology & Metabolism 20028794137414110.1210/jc.2001-0202422-s 2.0-003673849412213861 · doi ↗ · pubmed ↗