Pachydermoperiostosis Associated With a Rare SLCO2A1 Mutation: A Case Report and Literature Review
Maen Mohammad, Yousef Alnajjar, Enas Jondi, Mohammad Alsheikh, Adeeb Darras, Abdullah Hamamdah, Muaath Itmaizeh

TL;DR
A 26-year-old man with a rare SLCO2A1 mutation was diagnosed with Pachydermoperiostosis, a genetic disorder causing skin thickening and bone changes, highlighting the need for early genetic testing and multidisciplinary care.
Contribution
Reports a rare SLCO2A1 mutation (c.563A>G, p.Gln188Arg) in a Pachydermoperiostosis case and provides insights from a literature review of 246 cases.
Findings
The c.940+1G>A splice variant is the most common SLCO2A1 mutation in PDP cases.
PDP shows male predominance (92.3%) and is most prevalent in Asian populations, particularly Chinese.
Common symptoms include digital clubbing (82.5%), pachydermia (74.4%), and hyperhidrosis (41.1%).
Abstract
Pachydermoperiostosis (PDP), also known as primary hypertrophic osteoarthropathy, is a rare genetic disorder characterized by digital clubbing, periostosis, and pachydermia. It typically presents during adolescence or early adulthood and is commonly associated with mutations in the HPGD or SLCO2A1 genes. Due to its nonspecific clinical features, PDP is often misdiagnosed, resulting in delayed treatment. We report the case of a 26-year-old Arab male with an eight-year history of progressive facial skin thickening, hyperhidrosis, and digital clubbing. Laboratory investigations were unremarkable, while imaging revealed periostosis. Genetic analysis identified a SLCO2A1 mutation (c.563A>G, p.Gln188Arg). Our patient experienced significant physical discomfort and psychological distress, with notable improvement following treatment with nonsteroidal anti-inflammatory drugs and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
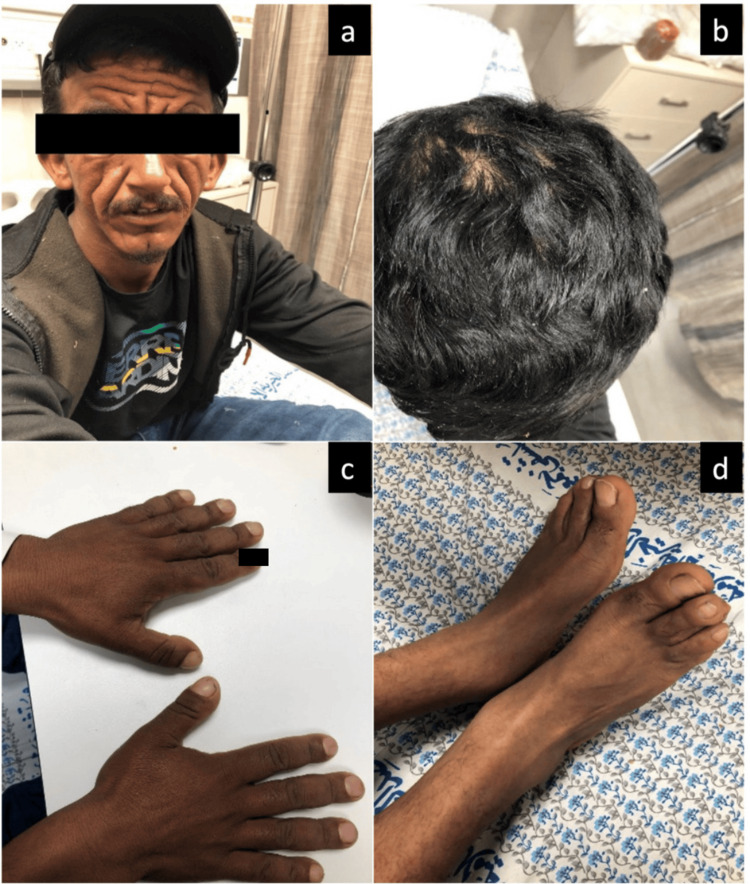 Figure 1
Figure 1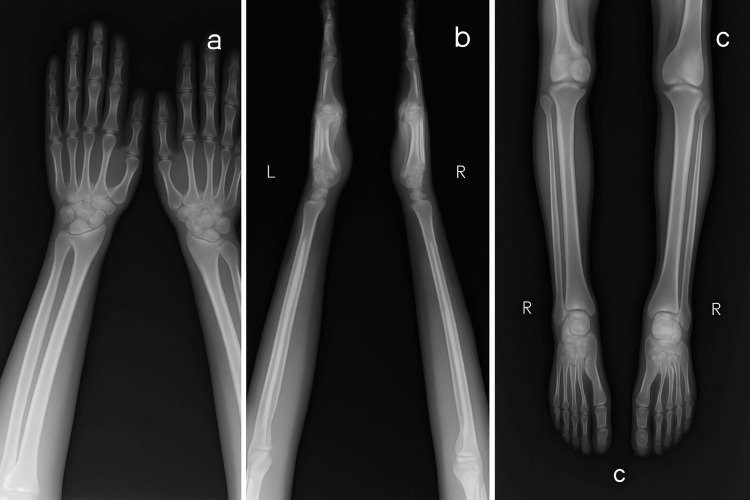 Figure 2
Figure 2| # | First author name | Year of publication | Sex (M/F) | Nationality/ethnicity | Symptoms first started? (age in years) | Age of diagnosis (years) | Excessive sweating | Progressive enlargement of hands and feet | Thickening of the skin of the face and scalp/pachyderma | Digital clubbing | Other manifestations/findings | Radiologic findings | Mutation type | Mutations site | Consanguinity (parents) | Previously suspected diagnosis? | Management |
| 1 | Pang Q [ | 2024 | M | Chinese | - | - | - | - | - | - | - | - | Compound heterozygous | c.1375T>C c.850A>G | No | - | None |
| 2 | M | Chinese | - | - | - | - | - | - | - | - | Compound heterozygous | c.1375T>C c.850A>G | No | - | None | ||
| 3 | M | Chinese | - | - | - | - | - | - | - | - | Homozygous | c.1589G>A | No | - | None | ||
| 4 | M | Chinese | - | - | - | - | - | - | - | - | Compound heterozygous | c.940+1G>A c.1624C>T | No | - | None | ||
| 5 | M | Chinese | - | - | - | - | - | - | - | - | Heterozygous | c.830delT | No | - | None | ||
| 6 | M | Chinese | - | - | - | - | - | - | - | - | Compound heterozygous | c.823T>G c.1681C>T | No | - | None | ||
| 7 | M | Chinese | - | - | - | - | - | - | - | - | Homozygous | c.855delA | No | - | None | ||
| 8 | M | Chinese | - | - | - | - | - | - | - | - | Heterozygous | c.131_134GCCA>CCTGT | No | - | None | ||
| 9 | M | Chinese | - | - | - | - | - | - | - | - | Compound heterozygous | c.1136G>A c.1070A>G | No | - | None | ||
| 10 | M | Chinese | - | - | - | - | - | - | - | - | Compound heterozygous | c.941-1G>A c.1106G>A | No | - | None | ||
| 11 | M | Chinese | - | - | - | - | - | - | - | - | Compound heterozygous | c.611C>T c.1624C>T | No | - | None | ||
| 12 | Dai Y [ | 2024 | M | Chinese | 22 | 32 | No | Yes | Yes | Yes | Recurrent lower abdominal pain, bloody and purulent stools Mild hypoalbuminemia and anemia ESR was elevated at 55 mm/h hsCRP was elevated at 23.41 mg/L Esophagogastroduodenoscopy revealed significant thickening of gastric folds in the cardia, fundus, body, antrum, and the descending duodenum Hematoxylin and eosin (H&E) stained gastric biopsies showed enlarged, densely packed glands Colonoscopy findings included diffuse mucosal edema, erosions, and purulent exudate in the sigmoid colon and rectum Colonic and rectal H&E stains showed inflammation and disrupted crypt architecture, consistent with ulcerative colitis (UC) | Periostosis, cortical thickening and diffuse increased bone density. | Homozygous | c.929A > G | No | - | mesalazine for enteropathy |
| 13 | Shang Q [ | 2024 | M | Chinese | 20 | 32 | - | - | Yes | Yes | Ileus, diarrhea, hematochezia Reflux esophagitis Gastric polyps Ileal multiple strictures with annular ulcer Sigmoid colon isolated stricture with annular ulcer Congenital lymphatic dysplasia | Periostosis | Homozygous nonsense | c.1807C>T | No | - | - |
| 14 | M | Chinese | 29 | 39 | - | - | Yes | Yes | Ileus, diarrhea Gastric polyps Ileal multiple strictures with annular ulcer | Periostosis | Homozygous Frame shift | c.855delA | No | - | - | ||
| 15 | M | Chinese | 25 | 27 | - | - | Yes | Yes | Diarrhea, fever Gastric polyps Hypertrophic gastritis Diffuse mucosal erosions in colon and rectum | Periostosis | Homozygous Missense | c.929G>A | No | - | - | ||
| 16 | M | Chinese | 18 | 26 | - | - | Yes | Yes | Ileus, diarrhea Gastric polyps Ileal multiple strictures with annular ulcer | Periostosis | Compound heterozygous (Missense, Splicing site) | c.1106G>A c.941-1G>A | No | - | - | ||
| 17 | M | Chinese | 5 | 31 | - | - | Yes | Yes | Ileus, melena Gastric anastomotic ulcer Ileal multiple strictures with annular ulcer | Periostosis | Compound heterozygous (Frame shift, Missense) | c.1177delT c.1375T>C | No | - | - | ||
| 18 | M | Chinese | 17 | 47 | - | - | Yes | Yes | Ileus, pyloric obstruction Reflux esophagitis Gastric anastomotic ulcer Ileal multiple strictures with annular ulcer | Periostosis | Heterozygous Missense | c.1660G>A | No | - | - | ||
| 19 | M | Chinese | 24 | 29 | - | - | Yes | Yes | Ileus Hypertrophic gastritis Ileal multiple strictures with annular ulcer | Periostosis | Homozygous Nonsense | c.1771C>T | Yes | - | - | ||
| 20 | Niizeki H [ | 2024 | 43 | Japanese | - | - | - | - | - | - | - | - | - | c.1279_1290del12 | - | - | - |
| 21 | Long B [ | 2024 | M | - | 14 | 21 | - | Yes | Yes | Yes | recurrent diarrhea enlargement of both knees and ankles greasy facial skin gastric pyloric gland adenoma foveolar‐type gastric adenoma | multiple periosteal reactions throughout the body and periarticular soft tissue swelling | homozygous | c.940 + 1G > A | - | - | - |
| 22 | Kimball TN [ | 2024 | M | Mexico | - | - | - | - | - | - | CEAS | - | c.547G > A | - | - | - | |
| 23 | M | Mexico | - | - | - | - | - | - | CEAS | - | c.1768del | - | - | - | |||
| 24 | Nakano Y [ | 2023 | M | Japanese | 14 | 20 | Yes | Yes | Yes | Yes | recurrent knee hydrarthrosis | His knee showed thickening and fraying diaphysis in his lower extremities, without abnormality in the lumbar spine Cortical thickening of the long bones Symmetrical periosteal changes in the diaphysis of the fibula, tibia, metacarpals, metatarsals, and proximal phalanx in both hands and feet | Compound heterozygous (missense, splicing) | c.664G>A c.940+1G>A | No | Acromegaly | - |
| 25 | Zheng C [ | 2023 | M | - | - | 31 | - | - | - | - | CEAS | - | Homozygous | c.290G>A | - | - | - |
| 26 | Bloch A [ | 2023 | M | - | 10 | 40 | Yes | - | Yes | Yes | - | Periostosis | Homozygous | c.664G>A | - | - | - |
| 27 | M | - | 22 | 27 | No | - | Yes | Yes | - | Periostosis | Homozygous | c.861+2dupT | - | - | - | ||
| 28 | M | - | 10 | 28 | No | - | Yes | Yes | - | - | Homozygous | c.1241C>G | - | - | - | ||
| 29 | M | - | 5 | 34 | No | - | Yes | Yes | chronic diarrhea in childhood | - | Homozygous | c.1590C>A | - | - | - | ||
| 30 | M | - | 15 | 28 | Yes | - | Yes | Yes | - | Periostosis | Homozygous | c.1658delT | - | - | - | ||
| 31 | M | - | 20 | 22 | No | - | Yes | Yes | - | - | Homozygous | c.1682G>A | - | - | - | ||
| 32 | M | - | 33 | 36 | No | - | Yes | Yes | - | Periostosis | Heterozygous | c.234+1G>A | - | - | - | ||
| 33 | M | - | 14 | 47 | Yes | - | Yes | Yes | unilateral Deafness | Periostosis | Heterozygous | c.1523_1524del CT | - | - | - | ||
| 34 | M | - | 40 | 41 | No | - | No | Yes | - | Periostosis | Heterozygous | c.1625G>A | - | - | - | ||
| 35 | M | - | 30 | 34 | No | - | Yes | Yes | - | Periostosis | Heterozygous | c.31del | - | - | - | ||
| 36 | Chen B [ | 2023 | M | Chinese | 17 | 31 | No | Yes | Yes | Yes | - | cortical hyperostosis in the distal tibia and fibula periostosis of the diaphysis in the distal left and right radius | Compound heterozygous (nonsense, splice-site) | c.96+4A>C in the exon-intron 2 boundary c.1807 C>T in exon 13 in the proband | No | - | - |
| 37 | Nicolau R [ | 2023 | M | Portuguese | 15 | 20 | Yes | Yes | Yes | Yes | prolonged morning stiffness facial acne CRP: 35.5 mg/L ESR: 27 mm/h | soft tissue swelling, periosteal ossification and cortical thickening of the skull, phalanges, femur and toe acroosteolysis | Homozygous | c.1259G > T | No | - | naproxen 500 mg/day |
| 38 | Umair M [ | 2023 | M | Pakistani | - | 28 | No | No | No | Yes | - | - | Homozygous Missense | c.155T>A | Yes | - | - |
| 39 | M | Pakistani | - | 31 | No | No | No | Yes | - | - | Homozygous Missense | c.155T>A | Yes | - | - | ||
| 40 | Pasumarthi D [ | 2023 | M | South Indian | - | 25 | - | Yes | Yes | Yes | swelling and pain in knee joint heavy eyelids with ptosis, blepharoptosis Seborrhea | Periosteal reaction in long bones | Homozygous missense | c.614C>T | Yes | - | - |
| 41 | M | South Indian | - | 23 | Yes | Yes | Yes | Yes | recurrent intermittent fever pain and swelling of bilateral ankle joints | Periosteal reaction in long bones | Homozygous nonsense | c.529C>T | Yes | - | - | ||
| 42 | M | North Indian | - | 20 | - | Yes | Yes | Yes | bilateral swelling of ankle joints | Periosteal reaction in long bones | Homozygous Frameshift | c.1229_1238delTCCTTTGTGT | No | - | - | ||
| 43 | Dong Z [ | 2022 | M | - | - | 30 | - | - | - | - | gastric cancer | - | - | - | - | - | - |
| 44 | Albawa'neh A [ | 2022 | M | Emarati | - | 22 | - | Yes | Yes | Yes | symmetrical pain in his wrists, hand proximal interphalangeal (PIP) joints, ankles, and feet CRP: 15.44 mg/L | Periostosis MRI of the right ankle and foot showed an ankle effusion with a healing sprain of the posterior inferior tibiofibular ligament. There were effusions noted in the calcaneocuboid, naviculocuneiform, first tarsometatarsal (TMT), first metatarsophalangeal (MTP) joints, and the second–fifth distal interphalangeal (IP) joints and associated non-specific multifocal marrow edema. | Homozygous | c.289C>T | - | seronegative rheumatoid arthritis | etoricoxib 60 mg once daily |
| 45 | Biswas S [ | 2022 | M | - | 12 | - | - | Yes | Yes | Yes | eyelids appeared to be swollen and drooping intermittent episodes of diarrhoea weight loss mild sensorineural hearing loss myelofibrosis | periosteitis upper gastrointestinal endoscopy: hypertrophic gastropathy | - | - | No | - | low dose steroids (prednisolone) etoricoxib retinoids |
| 46 | M | - | 14 | - | - | Yes | Yes | Yes | myelofibrosis | - | - | - | No | - | low dose steroids (prednisolone) etoricoxib retinoids vitamin A | ||
| 47 | Hong HS [ | 2022 | F | Korean | 21 | 39 | - | - | No | Yes | CEAS Abdominal pain loose stool weight loss | periostosis | Homozygous splicing site Wild type | c.940+1G>A c.1807C>T, p.R603X | - | - | - |
| 48 | F | Korean | 32 | 45 | - | - | No | Yes | CEAS Abdominal pain loose stool weight loss | periostosis | Heterozygous Heterozygous | c.940+1G>A c.1807C>T, p.R603X | - | - | - | ||
| 49 | M | Korean | 11 | 54 | - | - | Yes | Yes | CEAS Abdominal pain loose stool GI bleeding | periostosis | Heterozygous Heterozygous | c.940+1G>A c.1807C>T, p.R603X | - | - | - | ||
| 50 | F | Korean | 28 | 52 | - | - | Yes | Yes | CEAS Abdominal pain loose stool | periostosis | Wild type Homozygous | c.940+1G>A c.1807C>T, p.R603X | - | - | - | ||
| 51 | M | Korean | 15 | 29 | - | - | Yes | Yes | CEAS Abdominal pain loose stool | periostosis | Heterozygous Heterozygous | c.940+1G>A c.1807C>T, p.R603X | - | - | - | ||
| 52 | Wang Q [ | 2022 | M | - | 16 | 18 | Yes | No | Yes | Yes | Acne, seborrhea gynecomastia | Brain MRI scan showedscalp hypertrophy, which resembled petals. Radiography of both the legs showed periostitis | Compound heterozygous | - | - | - | 200 mg of celecoxib |
| 53 | Ikeda K [ | 2022 | M | - | 15 | 35 | - | - | Yes | Yes | limited range of motion in knee joints ptosis | periosteal thickening of extremities | - | - | - | - | - |
| 54 | Yousaf M [ | 2022 | M | Pakistan | 14 | 21 | Yes | Yes | Yes | Yes | body aches and joint pains affecting large joints i.e., bilateral wrist and knee joints intermittent low-grade fever lethargy conjunctival pallor transfusion-dependent anemia acne hepatosplenomegaly myelofibrosis | - | Homozygous | c.664G>A | Yes | - | erythropoietin and cyclooxygenase-2 (COX 2) inhibitors |
| 55 | Jeyabaladevan S [ | 2022 | M | Afghanistan | - | 15 | Yes | - | Yes | - | pain and swelling particularly affecting his knees and ankles, with large bilateral knee joint effusions ESR (70 mm/hr) CRP (22 mg l−1) allergic blepharo-conjuctivitis acne iron deficiency anaemia hyperplastic gastric polyps | periostosis was symmetrical and diffuse MRI of the left knee and ankle demonstrated circumferential periostosis, enlargement of the distal femur and distal tibia, synovial hypertrophy, and joint effusions | - | - | Yes | - | Knee aspirations intraarticular injections of 60 mg depomedrone |
| 56 | Kartal Baykan E [ | 2022 | M | Turkey | 13 | 16 | Yes | No | Yes | No | pain in the elbow and knee over three years CRP: 11.4 mg/L | Bilateral knee and hand radiographs were considered normal | Homozygous frameshift | c.86delG (p.G29Afs*48) | - | Acromegaly | hydroxychloroquine was prescribed (200 mg twice daily, PO) |
| 57 | M | Turkey | 12 | 17 | Yes | Yes | Yes | Yes | swelling in knee joints, knee pain, | De novo bone formation and cortical thickening were detected on bilateral knee radiographs Irregular sub-periosteal de novo bone formation and cortical thickening were observed in the tibia, fibula, calcaneum, and talus on bilateral ankle radiographs | Homozygous nonsense | c.31C>T (p.Q11*) | Yes | - | selective Cox-2 inhibitor (oral meloxicam, 15 mg twice daily) steroid (oral methylprednisolone, 5 mg/day) | ||
| 58 | Marques P [ | 2022 | M | - | - | 26 | Yes | Yes | Yes | Yes | prominent jaw and long eyelashes joint pain fatigue periodic episodes of watery diarrhea | - | Homozygous | - | - | Acromegaly | nonsteroid anti-inflammatory drugs zoledronate |
| 59 | Pang Q [ | 2022 | M | Chinese | - | - | Yes | - | Yes | Yes | - | periostosis and acro-osteolysis | - | - | - | - | - |
| 60 | M | Chinese | - | - | Yes | - | Yes | Yes | - | periostosis and acro-osteolysis | - | - | - | - | - | ||
| 61 | M | Chinese | - | - | Yes | - | Yes | Yes | - | periostosis and acro-osteolysis | - | - | - | - | - | ||
| 62 | M | Chinese | - | - | Yes | - | Yes | Yes | - | periostosis and acro-osteolysis | - | - | - | - | - | ||
| 63 | M | Chinese | - | - | Yes | - | Yes | Yes | - | periostosis and acro-osteolysis | - | - | - | - | - | ||
| 64 | M | Chinese | - | - | Yes | - | Yes | Yes | - | periostosis and acro-osteolysis | - | - | - | - | - | ||
| 65 | M | Chinese | - | - | Yes | - | Yes | Yes | - | periostosis and acro-osteolysis | - | - | - | - | - | ||
| 66 | M | Chinese | - | - | Yes | - | Yes | Yes | - | periostosis and acro-osteolysis | - | - | - | - | - | ||
| 67 | M | Chinese | - | - | Yes | - | Yes | Yes | - | periostosis and acro-osteolysis | - | - | - | - | - | ||
| 68 | M | Chinese | - | - | Yes | - | Yes | Yes | - | periostosis and acro-osteolysis | - | - | - | - | - | ||
| 69 | M | Chinese | - | - | Yes | - | Yes | Yes | - | periostosis and acro-osteolysis | - | - | - | - | - | ||
| 70 | M | Chinese | - | - | Yes | - | Yes | Yes | - | periostosis and acro-osteolysis | - | - | - | - | - | ||
| 71 | Xu C [ | 2021 | M | Chinese | 15 | 16 | Yes | Yes | Yes | Yes | seborrhea | soft tissue tumefaction and hyperostosis of metacarpal bones and phalanges irregular periosteal hypertrophy with subperiosteal new bone formation of bilateral tibia and fibula | Compound heterozygous | c.941-1G>A(splicing) c.754C>T(p.R252X) | No | - | Etoricoxib (60 mg per day) |
| 72 | Tran TH [ | 2021 | M | Vietnamese | 16 | 19 | Yes | Yes | Yes | Yes | ESR: 24 mm/h CRP: 30.41 mg/L | Periostosis | Homozygous | c.669C>G | - | Rheumatoid arthritis | NSAIDs Hydroxychloroquine (both not effective) |
| 73 | Sun K [ | 2021 | M | Chinese | - | 33 | - | Yes | Yes | Yes | Anemia intestinal perforation due to segmental coarctation of the intestinal tract splenomegaly portal hypertension splenic vein thickening intestinal ulcers decayed tooth | CT: partial intestinal aggregation and bowel wall thickening in the jejunum and ileum | Homozygous Heterozygous | c.210G>A (Homozygous) c.838C>T (Heterozygous) | No | - | - |
| 74 | Ishizuka T [ | 2021 | M | - | 12 | 41 | - | Yes | Yes | Yes | ileus and gastric ulcer needing partial gastrectomy at 13 years old | hyperrtrophic periosteum at both femur, tibia, fibula | Homozygous splice-site | c.940+1G>A | - | rheumatoid arthritis | baricitinib (2mg/day), |
| 75 | Xu Y [ | 2021 | - | Chinese | - | - | - | - | - | - | - | - | monoallelic | c.1660G>A | - | - | - |
| 76 | - | Chinese | - | - | - | - | - | - | - | - | monoallelic. | c.664G>A | - | - | - | ||
| 77 | - | Chinese | - | - | - | - | - | - | - | - | monoallelic | c.1065dupA | - | - | - | ||
| 78 | - | Chinese | - | - | - | - | - | - | - | - | monoallelic. | c.1293delT | - | - | - | ||
| 79 | - | Chinese | - | - | - | - | - | - | - | - | monoallelic. | c.1106G>A | - | - | - | ||
| 80 | - | Chinese | - | - | - | - | - | - | - | - | monoallelic | c.1807C>T | - | - | - | ||
| 81 | - | Chinese | - | - | - | - | - | - | - | - | monoallelic | c.1807C>T | - | - | - | ||
| 82 | - | Chinese | - | - | - | - | - | - | - | - | biallelic | c.664G>A c.621C>A | - | - | - | ||
| 83 | - | Chinese | - | - | - | - | - | - | - | - | biallelic | c.541G>C c.983T>C | - | - | - | ||
| 84 | - | Chinese | - | - | - | - | - | - | - | - | biallelic | c.1121C>T c.763G>A | - | - | - | ||
| 85 | - | Chinese | - | - | - | - | - | - | - | - | biallelic | c.1660G>A c.1814+1G>A | - | - | - | ||
| 86 | - | Chinese | - | - | - | - | - | - | - | - | biallelic | c.1807C>T c.1807C>T | - | - | - | ||
| 87 | Huang H [ | 2021 | M | Chinese | 12 | 27 | - | - | Yes | Yes | Abdominal pain Anemia Hypoproteinemia intestinal ulcers CRP: 14.14 mg/L ESR: 25 mm/h | - | Homozygous | c.941-1G>A | No | - | - |
| 88 | Ishibashi M [ | 2021 | M | - | - | 18 | - | - | Yes | Yes | - | Periostosis | Homozygous | c.940 þ 1G > A | - | - | - |
| 89 | M | - | - | 25 | - | - | Yes | Yes | - | Periostosis | Homozygous | c.940 þ 1G > A | - | - | - | ||
| 90 | M | - | - | 29 | - | - | Yes | Yes | - | Periostosis | Homozygous | c.940 þ 1G > A | - | - | - | ||
| 91 | M | - | - | 32 | - | - | Yes | Yes | - | Periostosis | c.940 þ 1G > A c.1807C > T | - | - | - | |||
| 92 | M | - | - | 20 | - | - | Yes | Yes | - | Periostosis | Homozygous | c.664G > A | - | - | - | ||
| 93 | M | - | - | 50 | - | - | Yes | Yes | - | Periostosis | Homozygous | c.664G > A | - | - | - | ||
| 94 | M | - | - | 23 | - | - | No | Yes | - | Periostosis | c.940 þ 1G > A c.1279_1290Δ12 | - | - | - | |||
| 95 | M | - | - | 29 | - | - | No | Yes | - | Periostosis | c.940 þ 1G > A c.1279_1290Δ12 | - | - | - | |||
| 96 | M | - | - | 23 | - | - | No | Yes | - | Periostosis | Homozygous | c.1279_1290Δ12 | - | - | - | ||
| 97 | Oiwa T [ | 2021 | M | - | 16 | 20 | No | Yes | Yes | Yes | Acne chronic diarrhea | Periostosis | Homozygous | c.940+1G>A, p.R288Gfs*7 | - | - | Cosmetic surgery was performed on his forehead |
| 98 | M | - | 12 | 25 | No | Yes | Yes | Yes | duodenal ulcer Crohn’s disease | Periostosis | Homozygous | c.940+1G>A/p.R288Gfs*7 | - | - | biweekly injection of adalimumab (80 mg) | ||
| 99 | M | - | 15 | 21 | No | Yes | Yes | Yes | facial acne ADHD | Periostosis | Homozygous | c.664G>A/p.G222R | - | - | atomoxetine for ADHD | ||
| 100 | Pang Q [ | 2020 | M | Chinese | - | - | Yes | - | Yes | Yes | - | Periostosis | Homozygous | c.1589G>A | No | - | - |
| 101 | M | Chinese | - | - | Yes | - | Yes | Yes | - | Periostosis | Homozygous | c.855delA | No | - | - | ||
| 102 | M | Chinese | - | - | Yes | - | Yes | Yes | - | Periostosis | Heterozygous | c.131_134GCCA>CCTGT | No | - | - | ||
| 103 | M | Chinese | - | - | Yes | - | Yes | Yes | - | Periostosis | Compound heterozygous | c.941-1G>A c.1106G>A | No | - | - | ||
| 104 | M | Chinese | - | - | Yes | - | Yes | Yes | - | Periostosis | Compound heterozygous | c.1634delA c.823T>G | No | - | - | ||
| 105 | M | Chinese | - | - | Yes | - | Yes | Yes | - | Periostosis | Homozygous | c.855delA | No | - | - | ||
| 106 | M | Chinese | - | - | Yes | - | Yes | Yes | - | Periostosis | Compound heterozygous | c.823T>G c.1681C>T | No | - | - | ||
| 107 | M | Chinese | - | - | Yes | - | Yes | Yes | - | Periostosis | Compound heterozygous | c.823T>G c.129_130insC | No | - | - | ||
| 108 | M | Chinese | - | - | Yes | - | Yes | Yes | - | Periostosis | Compound heterozygous | c.1136G>A c.1070A>G | No | - | - | ||
| 109 | M | Chinese | - | - | Yes | - | Yes | Yes | - | Periostosis | Heterozygous | c.830delT | No | - | - | ||
| 110 | Tsuzuki Y [ | 2020 | M | - | 46 | 49 | No | Yes | Yes | Yes | palpitation and shortness of breath upon exertion anemia hypoalbuminemia fecal occult blood test was positive intestinal capsule endoscopy demonstrated scattered round ulcers throughout the entire ileum CEAS with ileal ulcers | periostosis of the fingers and long bones in the limb Brain-CT revealed skin hypertrophy | Homozygous | c.1807C>T | - | - | RBC transfusion for severe anemia oral Fe tablets (100 mg/day) was commenced a few weeks later oral mesalazine (3,000 mg/day) |
| 111 | Sonoda A [ | 2020 | M | - | - | 65 | - | - | Yes | Yes | anemia multiple circular and longitudinal ulcers throughout the entire small intestine gastric scarring CEAS | Periostosis | Compound heterozygous | c.940+1 G>A (splice site variant) c.1475 G>A | No | Gitelman syndrome Crohn's disease | - |
| 112 | Li N [ | 2020 | M | Chinese | 16 | 18 | - | Yes | Yes | Yes | Anemia intermittent stomach pain | swelling of the soft tissue in both hands, knee joints, and feet symmetrical thickening of the first phalanx and first metatarsal | Homozygous | c.1807C>T | Yes | - | - |
| 113 | Torgutalp M [ | 2019 | M | - | 12 | 20 | Yes | Yes | Yes | Yes | diffuse joint pain swelling and an hour of morning stiffness seborrheic eczema CRP: 57 mg/L ESR: 36 mm/h | neckchest-abdomen-pelvis computed tomography: normal Joint radiographs were similarly in accordance with inflammatory arthritis (especially erosions in wrists), but also revealed thickening in the mid-diaphyseal parts of the metacarpal and phalangeal bones, and cortical thickening on metaphysis of distal femur and proximal tibia Hypertrophic subperiosteal new bone formation and cortical irregularity with increased periosteal vascularity were determined by MRI of the femur | Homozygous | c.576C>G | - | Juvenile Idiopathic Arthritis: | acemetacin |
| 114 | Wang Q [ | 2019 | M | Chinese | 18 | 28 | - | Yes | Yes | Yes | Diarrhea Hematochezia chronic superficial gastritis and fundic gland polyps scattered ulcers and hemorrhagic spots at the terminal ileum and colon | periostosis | Homozygous | c1807 C > T | - | - | etoricoxib 30 mg~ 60 mg once daily Partial enterectomy |
| 115 | M | Chinese | - | 36 | - | Yes | Yes | Yes | intermittent abdominal colic, diarrhea, and anemia | periostosis | Homozygous | c.855delA | - | - | etoricoxib 60 mg once daily mesalazine (3 g/day) for 3 months prednisone (0.8 g/kg/day) for 1 month Partial enterectomy | ||
| 116 | Xiao J [ | 2019 | M | Chinese | 14 | - | - | Yes | Yes | Yes | - | - | Compound heterozygous | c.310G>A c.861+1G>A | - | - | - |
| 117 | M | Chinese | - | - | - | Yes | No | Yes | - | - | Heterozygous | c.310G>A | - | - | - | ||
| 118 | Li X [ | 2019 | M | Tibetan | 15 | 19 | - | Yes | Yes | Yes | hematemesis seborrhea and acne | X‑ray of the extremities demonstrated enlarged diaphysis, soft tissue swelling and periosteal proliferation Gastroscopy revealed hypertrophic gastric folds with multiple ulcers in gastric antrum | Homozygous nonsense | c.1807C>T | No | - | - |
| 119 | Jiang Y [ | 2019 | M | Chinese | 16 | 33 | Yes | Yes | Yes | Yes | pain and swelling of knees weakness of the extremities diarrhea serum potassium of 3.3 mmol/L | periosteal hyperostosis of tibia and fibula periosteal hyperostosis of phalanges | Compound heterozygous | c.850 A > G c.1375 T > C | No | - | etoricoxib 60 mg qd oral potassium supplements |
| 120 | M | Chinese | 20 | 35 | - | Yes | Yes | Yes | serum potassium was 3.4 mmol/L | periosteal hyperostosis of tibia and fibula periosteal hyperostosis of phalanges | Compound heterozygous | c.850 A > G c.1375 T > C | No | - | - | ||
| 121 | Yuan L [ | 2018 | M | Chinese | - | 43 | Yes | Yes | Yes | Yes | Arthralgia of large joints | Periostosis | Heterozygous frameshift Heterozygous missense | c.122delC c.1781G>A | No | - | - |
| 122 | M | Chinese | - | 37 | Yes | Yes | Yes | Yes | - | Periostosis | Heterozygous frameshift Heterozygous missense | c.122delC c.1781G>A | No | - | - | ||
| 123 | M | Chinese | - | 25 | Yes | Yes | Yes | Yes | Arthralgia of large joints | Periostosis | Homozygous missense | c.1681C>T c.1681C>T | No | - | - | ||
| 124 | M | Chinese | - | 33 | Yes | Yes | Yes | Yes | - | Periostosis | Heterozygous missense Heterozygous | c.440G>A c.940+1G>A | No | - | - | ||
| 125 | M | Chinese | - | 38 | Yes | Yes | Yes | Yes | - | Periostosis | Compound heterozygous | c.724+1G>A c.940+1G>A | No | - | - | ||
| 126 | Umeno J [ | 2018 | M | Japanese | - | 26 | - | - | Yes | Yes | CEAS Two lesions of ulceration with stenosis were observed in the ileum | Periostosis | Compound heterozygous | c.547G > A c.940 + 1G > A | - | - | - |
| 127 | M | Japanese | - | - | - | - | Yes | Yes | CEAS | Periostosis | - | - | - | - | - | ||
| 128 | M | Japanese | - | - | - | - | Yes | Yes | CEAS | Periostosis | - | - | - | - | - | ||
| 129 | M | Japanese | - | - | - | - | Yes | Yes | CEAS | Periostosis | - | - | - | - | - | ||
| 130 | M | Japanese | - | - | - | - | Yes | Yes | CEAS | Periostosis | - | - | - | - | - | ||
| 131 | Alessandrella A [ | 2018 | M | Morrocan | 13 | 17 | Yes | Yes | Yes | Yes | effusion in his knees kyphoscoliosis | metaphysis flaring of the distal femur and proximal tibia swelling of the periarticular soft tissue and cortical thicken- ing of the first metatarsal bilaterally | Homozygous | c.1658delT | No | - | hydroxychloroquine (400 mg per day). |
| 132 | Sun F [ | 2018 | M | Chinese | 17 | 23 | - | Yes | Yes | Yes | intermittent watery diarrhea | Periostosis | Homogenous missense | c.547G>A | Yes | - | Etoricoxib (60 mg/d) |
| 133 | Villarreal-Martínez A [ | 2018 | M | Mexican | 13 | 23 | - | - | Yes | Yes | severe acne and hyperseborrhea | periosteal bone formation circumferentially along the shaft of the tibia and fibula as well as cortical thickening at the distal ends. | Compound heterozygous | c.572G>C c.1186G>A | - | - | - |
| 134 | M | Mexican | 13 | 24 | - | - | Yes | Yes | bilateral knee pain, swelling and reduced range of movement Ota nevus on the left side of the face prognathism | subperiosteal reaction in the lateral condyle of the femur and tibia | Homozygous | c.96+5>A | - | - | - | ||
| 135 | Li SS [ | 2017 | M | Chinese | - | 31.6 | Yes | - | Yes | Yes | Seborrhae Arthralgia Watery diarrhea | Periostosis | Homozygous | c.941-1G>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months |
| 136 | M | Chinese | - | 31.7 | Yes | - | Yes | Yes | Seborrhae Arthralgia Watery diarrhea | Periostosis | - | c.941-2A>G c.1406C>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 137 | M | Chinese | - | 25.6 | Yes | - | Yes | Yes | Seborrhae Watery diarrhea | Periostosis | Homozygous | c.1406C>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 138 | M | Chinese | - | 29.5 | Yes | - | Yes | Yes | Seborrhae | Periostosis | - | c.1069T>C c.1406C>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 139 | M | Chinese | - | 35.9 | No | - | Yes | Yes | - | Periostosis | - | c.440G>A c.1624C>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 140 | M | Chinese | - | 24.8 | Yes | - | Yes | Yes | Seborrhae Watery diarrhea | Periostosis | Homozygous | c.1602C>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 141 | M | Chinese | - | 21.9 | Yes | - | No | Yes | Seborrhae Arthralgia Watery diarrhea | Periostosis | Homozygous | c.1771C>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 142 | M | Chinese | - | 19.3 | Yes | - | Yes | Yes | Seborrhae Arthralgia Watery diarrhea | Periostosis | - | c.178G>A c.547G>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 143 | M | Chinese | - | 29.4 | Yes | - | Yes | Yes | Seborrhae | Periostosis | Homozygous | deletion( | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 144 | M | Chinese | - | 18.4 | Yes | - | Yes | No | Seborrhae | Periostosis | - | c.178G>A c.1660G>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 145 | M | Chinese | - | 24 | Yes | - | Yes | Yes | Seborrhae | Periostosis | - | c.759G>A c.764G>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 146 | M | Chinese | - | 19.6 | Yes | - | Yes | Yes | Arthralgia | Periostosis | - | c.1378G>A c.611C>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 147 | M | Chinese | - | 33.4 | Yes | - | Yes | Yes | Seborrhae | Periostosis | - | c.1406C>T c.1771C>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 148 | M | Chinese | - | 24.9 | Yes | - | No | Yes | Seborrhae Watery diarrhea | Periostosis | - | c.1292dupC c.1456C>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 149 | M | Chinese | - | 21.7 | No | - | Yes | Yes | Seborrhae | Periostosis | Homozygous | c.1807C>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 150 | M | Chinese | - | 27.5 | Yes | - | Yes | Yes | Seborrhae Arthralgia | Periostosis | Homozygous | c.941-1G>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 151 | M | Chinese | - | 21.9 | No | - | Yes | Yes | - | Periostosis | - | c.1624C>T c.1807C>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 152 | M | Chinese | - | 26.8 | Yes | - | Yes | Yes | Seborrhae Watery diarrhea | Periostosis | Homozygous | c.440G>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 153 | M | Chinese | - | 21.2 | Yes | - | Yes | Yes | Seborrhae | Periostosis | - | c.754C>T c.1106G>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 154 | M | Chinese | - | 21.1 | No | - | Yes | Yes | Seborrhae Arthralgia Watery diarrhea | Periostosis | - | c.1287C>A c.1406C>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 155 | M | Chinese | - | 29.5 | Yes | - | Yes | Yes | Seborrhae Watery diarrhea | Periostosis | Homozygous | c.838C>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 156 | M | Chinese | - | 25 | Yes | - | Yes | Yes | Seborrhae Arthralgia Watery diarrhea | Periostosis | Homozygous | c.838C>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 157 | M | Chinese | - | 21 | Yes | - | Yes | Yes | Watery diarrhea | Periostosis | Homozygous | c.838C>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 158 | M | Chinese | - | 24.2 | No | - | Yes | Yes | Seborrhea, watery diarrhea | Periostosis | - | c.178G>A c.310G>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 159 | M | Chinese | - | 24.9 | No | - | Yes | Yes | Seborrhea, arthralgia, watery diarrhea | Periostosis | Heterozygous | c.1293delT | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 160 | M | Chinese | - | 25.2 | Yes | - | Yes | Yes | Seborrhea | Periostosis | Homozygous | c.1372G>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 161 | M | Chinese | - | 19.9 | Yes | - | Yes | Yes | Seborrhea | Periostosis | - | c.289C>T c.1106G>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 162 | M | Chinese | - | 42.4 | Yes | - | Yes | Yes | Seborrhea, watery diarrhea | Periostosis | Heterozygous | c.1660G>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 163 | M | Chinese | - | 24.9 | No | - | Yes | Yes | Seborrhea, arthralgia | Periostosis | - | c.96+4A>C c.565C>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 164 | M | Chinese | - | 35.9 | Yes | - | Yes | Yes | Seborrhea, watery diarrhea | Periostosis | Homozygous | c.941-1G>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 165 | M | Chinese | - | 30.1 | Yes | - | No | Yes | Seborrhea, watery diarrhea | Periostosis | Heterozygous | c.664G>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 166 | M | Chinese | - | 22.2 | Yes | - | Yes | Yes | Seborrhea | Periostosis | - | c.656C>T c.1839C>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 167 | M | Chinese | - | 25 | Yes | - | Yes | Yes | Seborrhea | Periostosis | - | c.1106-1G>A c.1807C>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 168 | M | Chinese | - | 24 | Yes | - | Yes | Yes | Seborrhea | Periostosis | - | c.861+2T>C c.1095C>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 169 | M | Chinese | - | 51 | No | - | Yes | Yes | Seborrhea, arthralgia, watery diarrhea | Periostosis | - | c.621C>A c.664G>A | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 170 | M | Chinese | - | 22.7 | Yes | - | Yes | Yes | Seborrhea, watery diarrhea | Periostosis | - | c.440G>A c.1370C>T | - | - | etoricoxib (Arcoxia, 60 mg/day; Merck & Co) for 6 months | ||
| 171 | Ma W [ | 2017 | M | - | - | 25 | Yes | Yes | Yes | Yes | Cystic acne folliculitis | Periostosis | Homozygous missense | c.101T > C | - | Acromegaly | - |
| 172 | Guo T [ | 2017 | M | Chinese | 18 | 20 | - | - | Yes | Yes | - | Periostosis | Compound heterozygous | c.349 delC (frameshift deletion) c.1286A>G (missence mutation) | No | - | - |
| 173 | Karimova MM [ | 2017 | M | Uzbek | - | 24 | - | Yes | Yes | Yes | Excessive perspiration, generalized fatigue, scattered cafe-au-lait patches on abdomen | - | Homozygous | c.764G.A | No | Acromegaly | - |
| 174 | Mangupli R [ | 2017 | M | Venezuelan | 12 | 20 | - | Yes | Yes | Yes | Knee pain (extensive swelling and effusions bilaterally) | subperiostial bone formation with bone density and cortical thickening | Homozygous | c.830delT | - | Acromegaly | - |
| 175 | Tanese K [ | 2017 | M | Japanese | 14 | 21 | - | - | Yes | Yes | - | Periostosis | c.940+1G>A c.1279_1290del12 | - | - | - | |
| 176 | M | Japanese | 13 | 21 | - | - | Yes | Yes | - | Periostosis | c.940+1G>A c.1279_1290del12 | - | - | - | |||
| 177 | M | Japanese | 13 | 24 | - | - | - | - | - | - | c.940+1G>A c.1279_1290del12 | - | - | - | |||
| 178 | Shah K [ | 2017 | M | Pakistani | No | No | No | Yes | - | - | Homozygous | c.1A>G | - | - | - | ||
| 179 | M | Pakistani | No | No | No | Yes | - | - | Homozygous | c.1A>G | - | - | - | ||||
| 180 | F | Pakistani | No | No | No | Yes | - | - | Homozygous | c.1A>G | - | - | - | ||||
| 181 | Huang H [ | 2017 | M | Chinese | 19 | 32 | Yes | Yes | Yes | Yes | Gastric mucosa hyperplasia | Periostosis | - | c.1106G>A | Yes | - | - |
| 182 | M | Chinese | 18 | 27 | Yes | Yes | Yes | Yes | Gastric mucosa hyperplasia | Periostosis | - | c.1106G>A c.1106G>A | Yes | - | - | ||
| 183 | M | Chinese | 21 | 33 | Yes | Yes | Yes | Yes | Gastric mucosa hyperplasia | Periostosis | - | c.1106G>A c.941-1G>A | No | - | - | ||
| 184 | M | Chinese | 15 | 24 | Yes | Yes | Yes | Yes | Gastric mucosa hyperplasia | Periostosis | - | c.1771C>T c.1406C>T | No | - | - | ||
| 185 | M | Chinese | 19 | 33 | Yes | Yes | Yes | Yes | Gastric mucosa hyperplasia | Periostosis | - | c.1602C>A | No | - | - | ||
| 186 | M | Chinese | 14 | 33 | Yes | Yes | Yes | Yes | Gastric mucosa hyperplasia | Periostosis | - | c.611C>T c.96+4A>C | No | - | - | ||
| 187 | M | Chinese | 16 | 32 | Yes | Yes | Yes | Yes | Gastric mucosa hyperplasia | Periostosis | - | c.1069T>C | No | - | - | ||
| 188 | Lee S [ | 2016 | M | Korean | 19 | 56 | Yes | - | Yes | Yes | Seborrhoea and eczema, acne | Periostosis | - | c.302T>G | |||
| 189 | M | Korean | 17 | 54 | No | - | Yes | Yes | Seborrhoea and eczema, acne, hydrarthrosis | Periostosis | - | c.302T>G | |||||
| 190 | M | Korean | 20 | 52 | No | - | Yes | Yes | Seborrhoea and eczema, acne, hydrarthrosis | Periostosis | - | c.302T>G | |||||
| 191 | M | Korean | 17 | 19 | Yes | - | Yes | Yes | Seborrhoea and eczema, acne, hydrarthrosis PDA | Periostosis | - | c.940+1G>A c.1807C>T | |||||
| 192 | M | Korean | - | 23 | Yes | - | Yes | Yes | Seborrhoea and eczema, acne, hydrarthrosis | Periostosis | - | c.940+1G>A c.940+1G>A | |||||
| 193 | M | Korean | 13 | 19 | Yes | - | Yes | Yes | Seborrhoea and eczema, acne, hydrarthrosis PDA | Periostosis | - | c.940+1G>A c.940+1G>A | |||||
| 194 | Saadeh D [ | 2015 | M | Lebanese | - | 22 | - | Yes | Yes | Yes | Arthralgia | Periostosis | - | c.838C>T c.838C>T | - | - | - |
| 195 | M | Lebanese | - | 24 | - | Yes | Yes | Yes | Arthralgia | - | - | c.838C>T c.838C>T | - | - | - | ||
| 196 | Ayoub N [ | 2015 | M | Saudi | - | 23 | Yes | Yes | Yes | Yes | Arthralgia, seborrhoea, facial acne | Periostosis | Homozygous | c.1016C>T | - | - | - |
| 197 | Giancane G [ | 2015 | M | - | 13 | 21 | Yes | Yes | Yes | Yes | Seborrhoea, aplastic marrow | - | Compound heterozygous | c.754C>T c.794C>G | - | JIA | Ibuprofen 400 mg 3 times per day low dose steroid therapy oxybutynin 2.5 mg 3 times per day |
| 198 | Minakawa S [ | 2015 | M | Japanese | 12 | 15 | Yes | - | Yes | Yes | Seborrhea, arthralgia | Periostosis | Compound heterozygous | c.940+1G>A c.1279_1290del12 | - | - | - |
| 199 | Kim HJ [ | 2015 | M | Korean | 13 | 19 | - | - | Yes | Yes | Severe acne, arthralgia, watery diarrhea | Knee joint radiology revealed periosteal reaction with suspicious diaphyseal widening along the femur and tibia | Homozygous | c.940 + 1G > A | No | - | - |
| 200 | Madruga Dias JA [ | 2014 | M | African | 16 | 26 | - | Yes | Yes | Yes | Arthralgia | Periostosis | Homozygous | c.940+1G>A c.940+1G>A | No | - | etoricoxib 60 mg/day |
| 201 | Niizeki H [ | 2014 | F | Japanese | 43 | 67 | No | No | No | Yes | Myelopathy, arthralgia | Periostosis | Compound heterozygous | c.1279G>A c.1807C>T | - | - | - |
| 202 | Niizeki H [ | 2014 | M | Japanese | 15 | 19 | Yes | Yes | Yes | Yes | Acne, seborrhea, and eczema | Periostosis | Compound heterozygous | c.940+1G>A c.1279_1290del12 | No | - | - |
| 203 | M | Japanese | 16 | 21 | Yes | Yes | Yes | Yes | Acne, seborrhea, and eczema | Periostosis | Compound heterozygous | c.1807C>T c.754C > T | No | - | - | ||
| 204 | M | Japanese | 14 | 20 | Yes | Yes | Yes | Yes | Acne | Periostosis | Compound heterozygous | c.940+1G>A c.421G > T | No | - | - | ||
| 205 | M | Japanese | 14 | 20 | No | Yes | Yes | Yes | Acne, seborrhea, and eczema | Periostosis | Compound heterozygous | c.940+1G>A c.1807C > T | No | - | - | ||
| 206 | Cheng R [ | 2013 | M | Chinese | 20 | 25 | Yes | Yes | Yes | Yes | Arthralgia, seborrhea, gastric polyps, and erosive gastritis | Periostosis | Compound heterozygous | c.547G>A c.1807C>T | No | - | - |
| 207 | M | Chinese | 18 | 37 | - | - | Yes | Yes | Arthralgia Seborrhae | Periostosis | Compound heterozygous | c.940+1G>A c.1602C>A | No | - | - | ||
| 208 | Zhang Z [ | 2013 | M | Chinese | 19 | 22 | Yes | Yes | Yes | Yes | Recurrent blepharitis | periosteal overgrowth of the long bones | Compound heterozygous | c.940 + 1G > A c.1602C > A (missense) | No | - | - |
| 209 | Zhang Z [ | 2013 | M | Chinese | 16 | 36 | No | Yes | Yes | Yes | Stomachache, watery diarrhea, severe anemia, and hypoalbuminemia | periosteal overgrowth of the long bones | Homozygous | c.855delA | No | - | - |
| 210 | F | Chinese | - | 47 | No | - | - | - | Watery diarrhea, anemia, and hypoalbuminemia | - | Homozygous | c.855delA | No | - | - | ||
| 211 | F | Chinese | - | 42 | No | - | - | - | Watery diarrhea, anemia, and hypoalbuminemia | - | Homozygous | c.855delA | No | - | - | ||
| 212 | M | Chinese | - | 23 | Yes | Yes | Yes | Yes | Seborrhea, acne, watery diarrhea | periosteal overgrowth of the long bones | Homozygous | c.1106G>A | Yes | - | - | ||
| 213 | M | Chinese | 10 | 26 | Yes | Yes | Yes | Yes | Stomachache, watery diarrhea, recurrent blepharitis | periosteal overgrowth of the long bones | Homozygous | c.1393G>A | Yes | - | - | ||
| 214 | M | Chinese | 16 | 18 | No | Yes | Yes | Yes | Seborrhea, acne, watery diarrhea | periosteal overgrowth of the long bones | Compound heterozygous | c.493G>T c.1136G>A | No | - | - | ||
| 215 | M | Chinese | 17 | 24 | No | Yes | Yes | Yes | Seborrhea, acne, watery diarrhea | periosteal overgrowth of the long bones | Compound heterozygous | c.664G>A c.1634delA | No | - | - | ||
| 216 | M | Chinese | 19 | 42 | No | Yes | Yes | Yes | Seborrhea, acne, watery diarrhea | periosteal overgrowth of the long bones | Heterozygous | c.861+2T>C | No | - | - | ||
| 217 | M | Chinese | 17 | 17 | Yes | Yes | Yes | Yes | Seborrhea Acne | periosteal overgrowth of the long bones | Heterozygous | c.1065dupA | No | - | - | ||
| 218 | Zhang Z [ | 2013 | M | Chinese | 18 | 27 | Yes | Yes | Yes | Yes | Recurrent blepharitis | periosteal overgrowth of the long bones | Heterozygous Heterozygous missense | c.235-1G>T c.656C>T | No | - | - |
| 219 | Zhang Z [ | 2012 | M | Chinese | - | 24 | - | Yes | Yes | Yes | - | Periostosis | Homozygous | c.97-1G>A | Yes | - | - |
| 220 | M | Chinese | - | 27 | - | Yes | Yes | Yes | Stomach hemorrhage due to a gastric ulcer | Periostosis | - | c.764G>A c.1634delA | No | - | - | ||
| 221 | M | Chinese | - | 21 | - | Yes | Yes | Yes | - | Periostosis | - | c.664G>A c.940+1G>A | No | - | - | ||
| 222 | Busch J [ | 2012 | M | Japanese | 20 | 53 | - | Yes | - | Yes | Arthralgia | Periostosis | Heterozygous | c.940+1G>A c.1668G4C | - | - | - |
| 223 | M | Japanese | - | 21 | - | - | - | Yes | - | - | Homozygous | c.940+1G>A | Yes | - | - | ||
| 224 | M | Japanese | - | 19 | - | - | - | Yes | - | - | Homozygous | c.940+1G>A | Yes | - | - | ||
| 225 | M | Indian | 25 | 27 | - | Yes | Yes | Yes | Seborrhea | - | Homozygous | c.1292delC | Yes | - | - | ||
| 226 | M | Indian | 17 | 26 | Yes | Yes | - | Yes | Pain and swelling in ankle and knee | - | Homozygous | c.763G>A | Yes | - | - | ||
| 227 | M | Indian | 17 | 28 | Yes | Yes | - | Yes | Pain and swelling in ankle and knee | - | Homozygous | c.763G>A | Yes | - | - | ||
| 228 | Seifert W [ | 2012 | M | Turkish | - | 21 | Yes | Yes | Yes | Yes | Arthralgia | Periostosis | Homozygous | c.830_831insT | - | - | - |
| 229 | M | Turkish | - | 19 | Yes | Yes | Yes | Yes | Arthralgia | Periostosis | Homozygous | c.830_831insT | - | - | - | ||
| 230 | M | Turkish | - | 7 | - | - | - | - | - | - | Homozygous | c.830_831insT | - | - | - | ||
| 231 | M | Turkish | - | 40 | - | - | - | Yes | - | - | Hetrozygous | c.830_831insT | - | - | - | ||
| 232 | M | Iraqi | - | 38 | Yes | Yes | Yes | Yes | Arthralgia | Periostosis | Homozygous | c.1670T>C c.1670T>C | - | - | - | ||
| 233 | M | Dutch | - | 28 | - | - | - | Yes | - | - | Hetrozygous | c.754C>T | - | - | - | ||
| 234 | Diggle CP [ | 2012 | M | Hispanic (Colombia) | 19 | 49 | - | Yes | Yes | Yes | Anemia, myelofibrosis | Periostosis | - | c.1259G>T c.1259G>T | Yes | - | - |
| 235 | M | Chinese | 16 | - | - | Yes | Yes | Yes | - | Periostosis | - | c.941-1G>A c.1517C>A | - | - | - | ||
| 236 | M | Turkish | - | 21 | - | Yes | Yes | Yes | Anemia, myelofibrosis | Periostosis | - | c.542G>C c.542G>C | - | - | - | ||
| 237 | M | Dutch | - | - | - | Yes | Yes | Yes | - | Periostosis | - | c.1333C>T | - | - | - | ||
| 238 | M | French | - | - | - | - | - | - | - | - | - | c.290G>A c.940+2T>A | - | - | - | ||
| 239 | M | North African | - | 16 | - | - | - | - | Myelofibrosis | - | - | c.664G>A c.664G>A | - | - | - | ||
| 240 | M | North African | - | 17 | - | - | - | - | Myelofibrosis, hyperplastic gastropathy | - | - | c.253A>T c.253A>T | - | - | - | ||
| 241 | M | Dutch | - | 19 | - | - | - | - | - | - | - | c.1105+4A>G c.1105+4A>G | - | - | - | ||
| 242 | M | Kabardin (Caucasus) | - | 24 | - | - | - | - | - | - | - | c.838C>T c.1693T>G | - | - | - | ||
| 243 | M | Italian | 17 | - | - | - | - | - | - | - | - | c.310G>T c.310G>T | - | - | - | ||
| 244 | M | Algerian | 14 | - | - | - | - | - | - | - | - | c.724+1G>T c.724+1G>T | - | - | - | ||
| 245 | M | Turkish | - | - | - | - | - | - | Profound anemia, pancytopenia, myelofibrosis | - | - | c.542G>A c.542G>A | - | - | - | ||
| 246 | M | Italian | 14 | 15 | - | - | - | - | - | - | - | c.611C>T c.611C>T | - | - | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHypertrophic osteoarthropathy and related conditions · Dermatological and Skeletal Disorders · Dupuytren's Contracture and Treatments
Introduction
Pachydermoperiostosis (PDP) (Touraine-Solente-Gole syndrome) is a rare hereditary cause of hypertrophic osteoarthropathy. Hypertrophic osteoarthropathy can either be primary or secondary to underlying conditions affecting the pulmonary, cardiovascular, gastrointestinal, or other systems, with primary hypertrophic osteoarthropathy (PHO) accounting for less than 5% of all cases of hypertrophic osteoarthropathy [1,2]. PHO is classified based on genotype into three subtypes: PHOAR1 (15-hydroxyprostaglandin dehydrogenase (HPGD), autosomal recessive), PHOAR2 (solute carrier organic anion transporter family member 2A1 (SLCO2A1), autosomal recessive), and PHOAD (monoallelic SLCO2A1, autosomal dominant) [3]. It’s more common in adolescent males, with a male-female ratio of 7:1 [4].
PDP was first described in 1868 by Friedreich [5]. The precise pathophysiology of the disease remains poorly understood; however, current evidence shows that mutations in HPGD and SLCO2A1 lead to elevated prostaglandin E2 (PGE2) levels, through impaired degradation or transport, which underlie many features of PHO and provide the rationale for NSAID or COX-2 inhibitor therapy [6,7].
Herein, we report a rare case of a 26-year-old male patient whose presentation was highly suggestive of PDP and was diagnosed after a genetic study. A literature review providing data on SLCO2A1 mutations causing PDP is provided.
Case presentation
A 26-year-old male Arab patient, previously in his usual state of health, presented to our clinic with complaints of progressive changes in his facial features and extremities over the past eight years. The initial symptoms began with thickening and folding of the forehead, which gradually extended to involve both cheeks and the entire face. Over time, the facial changes became more pronounced, with deeper skin folds and increased coarseness, as assessed during serial clinical examinations. Sweating was evaluated based on the patient’s subjective reports compared with their baseline sweating prior to symptom onset, which indicated a progressive increase.
Concurrently, the patient noticed a gradual enlargement of his fingers, initially affecting the proximal interphalangeal joints within the first one to two years, followed by involvement of the distal interphalangeal joints over the next two years, and later affecting the metacarpophalangeal joints and wrists during the subsequent three to four years. Additionally, the size of his toes, ankles, and knees gradually increased over the same eight-year period. However, no changes were noted in his elbows, shoulders, hips, or spine, and he denied experiencing any pain or erythema in the involved joints.
The patient did not report symptoms such as shortness of breath, orthopnea, palpitations, or tremors. He also reported no history of headaches, visual disturbances, or abnormal height increase. Additionally, a comprehensive review of cardiovascular, gastrointestinal, and neurological systems was also unremarkable. The patient’s past medical, surgical, and family histories were unremarkable. The patient was not taking any chronic medications. The patient finished high school. He is not married, does not smoke or drink alcohol, and does not take illicit drugs.
On physical examination, the patient appeared hemodynamically stable, alert, conscious, and oriented. Examination of the head and neck revealed marked skin folds in the forehead and cheeks, giving the patient a "leonine" appearance (Figure 1a). Notably, there was scalp dandruff, but no other dermatologic abnormalities were observed (Figure 1b). On musculoskeletal examination, there was grade 4 nail clubbing and swelling of the distal interphalangeal, proximal interphalangeal, metacarpophalangeal joints, and wrists (Figure 1c). Examination of the lower limbs revealed swelling of the bilateral knees, ankles, and toes (Figure 1d). Cardiovascular, respiratory, neurological, and thyroid physical examinations were otherwise unremarkable.
(a) Pronounced forehead skin folds with prominent nasolabial folds; (b) Presence of scalp dandruff; (c) Nail clubbing; (d) Swelling of both legs.Written informed consent has been provided by the patient to have the case details and any accompanying images published.
Radiographic imaging revealed bilateral subperiosteal bone formation in the phalanges, metacarpals, radius, and ulna (Figures 2a-2b), as well as increased cortical thickness due to subperiosteal bone formation in the tibias, fibulas, and tarsal bones (Figure 2c). To exclude secondary causes, the patient underwent a comprehensive work-up. Laboratory tests showed a white blood cell count of 9.6 x 10^9^/L, hemoglobin of 14.6 g/dL, and a platelet count of 378 x 10^9^/L. Liver, kidney, and thyroid function tests were normal. Investigations to rule out acromegaly, including an insulin-like growth factor-1 (IGF-1) level, were within normal limits. Rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) antibodies were also negative. A computed tomography (CT) scan of the chest showed no evidence of pulmonary pathology. Echocardiography revealed no structural or functional cardiac abnormalities.
(a, b) Subperiosteal bone formation with enlargement of the phalanges, metacarpals, radius, and ulna. (c) Subperiosteal bone formation involving the bilateral distal tibiae and fibulae.
Over eight years, the patient exhibited progressive changes in facial and extremity features. After excluding secondary causes of hypertrophic osteoarthropathy through laboratory tests, imaging, and cardiovascular evaluation, clinical suspicion for a genetic form of PHO arose. Genomic amplification and direct sequencing of all exons of the HPGD and SLCO2A1 genes were performed on DNA extracted from the patient’s peripheral blood sample. The results revealed a homozygous c.563A>G (p.Gln188Arg) mutation in exon 4 of the SLCO2A1 gene, while no mutations were detected in the HPGD gene.
Over the past eight years, the patient’s social life has been significantly impacted by the progressive changes in his facial features and extremities. These physical changes led to considerable anxiety and a depressed mood, causing him to spend most of his time indoors. He consulted multiple doctors from different specialties before presenting to our hospital, and was distressed by not knowing his diagnosis. Although we advised the patient to seek psychiatric evaluation, he did not undergo a formal assessment. Upon receiving a diagnosis at our hospital, he experienced significant relief. The patient was treated with etoricoxib 90 mg orally once daily for six months to control pain and inflammation. Short-term corticosteroid therapy with prednisone 10 mg orally once daily for two weeks was administered during acute exacerbations. At his first follow-up visit one month after starting treatment, the patient reported a marked reduction in joint pain and facial discomfort. Examination revealed decreased joint tenderness and soft tissue swelling, with partial improvement in digital clubbing and pachydermia. Inflammatory markers (C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR)) also showed a modest decline during follow-up. This case highlights the importance of expert medical care and the need for supportive, multidisciplinary management, including dermatology, rheumatology, and psychiatry, to address the emotional, psychological, and social challenges that patients with rare and complex conditions often face.
Discussion
PDP, also known as PHO, is a rare genetic disorder with variable modes of inheritance described in the literature, the most commonly reported being the autosomal recessive mode in SLCO2A1 gene mutations [3,8]. Clinically, PDP is characterized by a combination of digital clubbing, pachyderma (skin thickening), excessive sweating, periostosis (inflammation of the periosteum), and enlargement of the hands and feet [9]. PDP can manifest in three clinical forms: the complete form, which includes both periostitis and pachydermia; the incomplete form, where bone changes are present without pachydermal features; and the forme fruste, which is characterized by pachydermal changes with little to no bone involvement.
PDP’s pathophysiology has not been completely understood. Literature suggests PDP results from elevated levels of prostaglandins, particularly PGE2. At the genetic level, mutations in either the HPGD gene, located on chromosome 4q34-q35, or the SLCO2A1 gene, which encodes a prostaglandin transporter, have been implicated in the pathogenesis of PDP [10-13]. The HPGD gene mutation leads to deficient activity of HPGD, the enzyme responsible for prostaglandin degradation, resulting in increased PGE2 levels. Similarly, mutations in the SLCO2A1 gene disrupt prostaglandin transport, contributing to elevated PGE2 concentrations and the subsequent clinical manifestations of the disease.
The definite pathophysiology explaining how increased levels of PGE2 lead to the clinical manifestations is not yet fully understood. In addition, many mutations have been reported in recent years, indicating that aspects of the disease are yet to be fully characterized. Our SLCO2A1 c.563A>G (p.Gln188Arg) variant, previously reported in a PDP cohort by Arcanjo et al., was identified in a homozygous proband with classic PDP [3]. This variant is absent from population databases. Our case provides additional clinical and imaging documentation that complements the existing cohort, illustrating the phenotypic spectrum associated with this rare, previously reported variant.
Being a rare condition, the exact number of reported cases of PDP remains undetermined, prompting us to conduct a thorough literature review. We searched PubMed for studies published since 2005, using the following keywords: "primary hypertrophic osteoarthropathy, pachydermoperiostosis, Touraine-Solente-Gole syndrome, and SLCO2A1." Our inclusion criteria were (1) studies published in English, (2) patients genetically diagnosed with a mutation in the SLCO2A1 gene causing PDP, and (3) studies that were fully accessible and provided relevant data. Exclusion criteria included (1) studies published in languages other than English, (2) studies published before 2005, (3) studies that were inaccessible or lacked necessary data, and (4) studies that identified SLCO2A1 mutations in the context of chronic enteropathy associated with SLCO2A1 (CEAS) only, without PDP. The collected data are presented in Table 1.
Upon reviewing the collected data, we documented 246 patients diagnosed with PDP due to mutations in the SLCO2A1 gene [6,8,12-80]. Our patient’s c.563A>G variant has not been previously reported as a pathogenic mutation associated with PDP, making it a novel mutation. The most frequently observed variant was c.940+1G>A. The male-to-female ratio was approximately 32:1 (with 92.3% of patients being male), which is higher than the commonly reported 7:1 ratio in PDP cases.
The ethnic breakdown of the reported cases revealed the following distribution: Chinese (53.3%) (n=131), Japanese (7.3%) (n=18), Korean (4.9%) (n=12), Turkish (3.2%) (n=8), Indian (2.4%) (n=6), and Pakistani (2.4%) (n=6). This supports previous findings indicating that PDP is most commonly prevalent in Asian populations.
Interestingly, the age of diagnosis for SLCO2A1 mutations causing PDP was relatively consistent between two age groups: ≤25 years (37%) (n=91) and 25-45 years (30%) (n=74), with 7% (n=17) of patients diagnosed at ≥45 years of age. Regarding the age of symptom onset, the majority of patients (33%) (n=82) experienced symptoms before the age of 20. In a previously published review, the onset of symptoms typically occurs between the ages of 12 and 18 years [5]. However, hypothetically, this can vary based on factors such as the homozygosity and location of genetic mutations, as well as the underreporting of cases that may change this range. Due to the rarity of the disease and the overlap of its manifestations with those of other conditions, PDP may frequently be misdiagnosed as secondary hypertrophic osteoarthropathy, acromegaly, thyroid acropachy, or other rheumatologic diseases.
The clinical presentation of PDP among the patients in our review showed the following distribution: hyperhidrosis (41.1%) (n=101), pachyderma/thickening of the skin on the face and scalp (74.4%) (n=183), and digital clubbing (82.5%) (n=203). Interestingly, consanguinity was present in 29.7% (n=73) of patients, which is notably higher than the 8.5% (n=21) with consanguinity. The most common mutation type observed in the SLCO2A1 gene was homozygous (39%) (n=97), followed by compound heterozygous (15%) (n=38) and heterozygous (13%) (n=32).
In our review, several observations and limitations were noted. A large number of studies were excluded because they were published in Chinese and Japanese, with the most commonly reported ethnicities in our table being Chinese and Japanese. This means that the percentage of these ethnicities would likely be even higher if the excluded studies had been included. Additionally, many studies diagnosed PDP solely based on clinical presentation, excluding other potential causes without performing genetic testing, and these studies were excluded from our review. This shows that mutations in the SLCO2A1 gene may be underreported, indicating the need for further research. A significant number of patients in our search were found to have mutations in the HPGD gene, which is likely more prevalent than SLCO2A1 mutations and has been more extensively researched. Lastly, many patients diagnosed with CEAS mutation did not exhibit the clinical features of PDP, underscoring the need for further research and better documentation to enhance our understanding of the disorder and its associations.
The management of PDP is primarily symptomatic, focusing on improving the patient's quality of life. Treatment options include non-steroidal anti-inflammatory drugs (NSAIDs) and corticosteroids [81]. In a systematic review published in 2017, 70% of patients treated with NSAIDs showed improvement in arthritis and arthalgia symptoms [82]. A study published in 2018 explored the use of hydroxychloroquine in a patient with PDP, resulting in a decrease in pain and improvement in the patient’s skin condition [16]. Additionally, bisphosphonates have been studied in both primary and secondary hypertrophic osteoarthropathy, with a recent meta-analysis suggesting their safety and efficacy. A total of 88.3% of patients with hypertrophic osteoarthropathy (primary and secondary) showed improvement in pain or arthritis [83]. Recently, a somatostatin analogue, lanreotide autogel (60 mg intramuscularly, administered once monthly for 12 months), was used for the first time in a patient with PDP. Notable improvements were observed, particularly with regard to excessive sweating and arthralgia [81]. Further research is warranted to evaluate the efficacy of somatostatin analogues in PHO. Biologic agents such as infliximab have also been trialed in refractory cases of PDP, though outcomes have been variable [84]. In severe, refractory cases of PDP that do not respond to medical therapy, surgical interventions may be considered [81].
Conclusions
PDP is a rare genetic disorder that is prevalent in the Asian population. Patients commonly present with digital clubbing, pachydermia, and periostitis. Genetic testing of the HPGD and/or SLCO2A1 genes is used for a definitive diagnosis. While the primary treatment involves the use of NSAIDs, other therapeutic options have been explored, and further research is necessary to evaluate their effectiveness.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pachydermoperiostosis: an update Clin Genet Castori M Sinibaldi L Mingarelli R Lachman RS Rimoin DL Dallapiccola B 4774866820051628387410.1111/j.1399-0004.2005.00533.x · doi ↗ · pubmed ↗
- 2Complete form of pachydermoperiostosis An Bras Dermatol Honório MLP Bezerra GH Costa VLDC 981019520203188959410.1016/j.abd.2019.04.009PMC 7058884 · doi ↗ · pubmed ↗
- 3Primary hypertrophic osteoarthropathy: phenotypic variability and penetrance rate in heterozygotes for SLCO 2A 1 variants JBMR Plus Arcanjo AM de Souza AF de Souza Quedas EP de Menezes Correia-Deur JE Ferreira DL de Almeida Toledo SP Lourenço DM Jr 09202510.1093/jbmrpl/ziaf 026PMC 1193782240144454 · doi ↗ · pubmed ↗
- 4Pachydermoperiostosis: a rare mimicker of acromegaly Endocrinol Diabetes Metab Case Rep Abdullah NR Jason WL Nasruddin AB 17292017201710.1530/EDM-17-0029 PMC 544542828567291 · doi ↗ · pubmed ↗
- 5Familial idiopathic hypertrophic osteoarthropathy and cranial suture defects in children Skeletal Radiol Reginato AJ Schiapachasse V Guerrero R 10510981982710093710.1007/BF 00349574 · doi ↗ · pubmed ↗
- 6Genotype and phenotype characterization of primary hypertrophic osteoarthropathy type 2 and chronic enteropathy associated with SLCO 2A 1: report of two cases and literature review Am J Med Genet A Kimball TN Rivero-García P Barrera-Godínez A Domínguez-Cherit J 0194202410.1002/ajmg.a.6344637915296 · doi ↗ · pubmed ↗
- 7Hyperostosis of the entire skeleton [Article in German]Archiv F Pathol Anat Friedreich N 8387431868
- 8Primary hypertrophic osteoarthropathy due to a novel SLCO 2A 1 mutation masquerading as acromegaly Endocrinol Diabetes Metab Case Rep Mangupli R Daly AF Cuauro E Camperos P Krivoy J Beckers A 17132017201710.1530/EDM-17-0013 PMC 540993828469926 · doi ↗ · pubmed ↗