Invasive Sphenoid Sinus Aspergillosis in a Patient With Chronic Neutropenia: A Case Report
Hafiz Fadl, Nicolas Bakinde, Teddy Ikhuoriah

TL;DR
A 75-year-old woman with chronic neutropenia developed invasive sphenoid sinus aspergillosis and was successfully treated with antifungal therapy.
Contribution
Highlights the occurrence of invasive fungal sinusitis in patients with transient or borderline immunosuppression.
Findings
Invasive sphenoid sinus aspergillosis can occur in patients with chronic neutropenia.
Successful treatment with liposomal amphotericin B followed by oral voriconazole led to full recovery.
Fungal sinusitis should be considered in patients without classical immunosuppression.
Abstract
Invasive sinus aspergillosis is an uncommon but potentially life-threatening infection typically observed in immunocompromised individuals. However, increasing reports highlight its occurrence in patients with transient or borderline immunosuppression. We present a case of a 75-year-old female with treated mantle cell lymphoma and chronic neutropenia who developed invasive sphenoid sinus aspergillosis. Diagnosis was confirmed via imaging and histopathology following surgical intervention. She was treated with liposomal amphotericin B, followed by a successful transition to oral voriconazole, with full clinical recovery. This case underscores the importance of considering fungal sinusitis in patients without classical or sustained immunosuppression and supports a multidisciplinary, stepwise approach to management.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1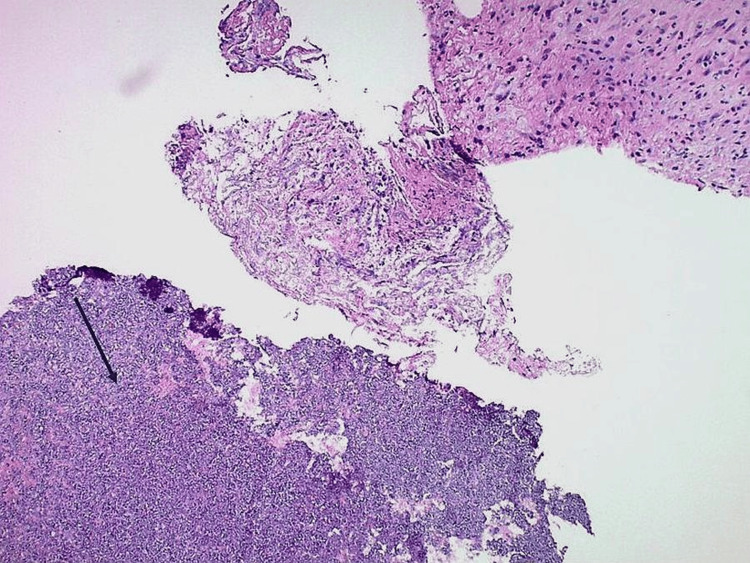 Figure 2
Figure 2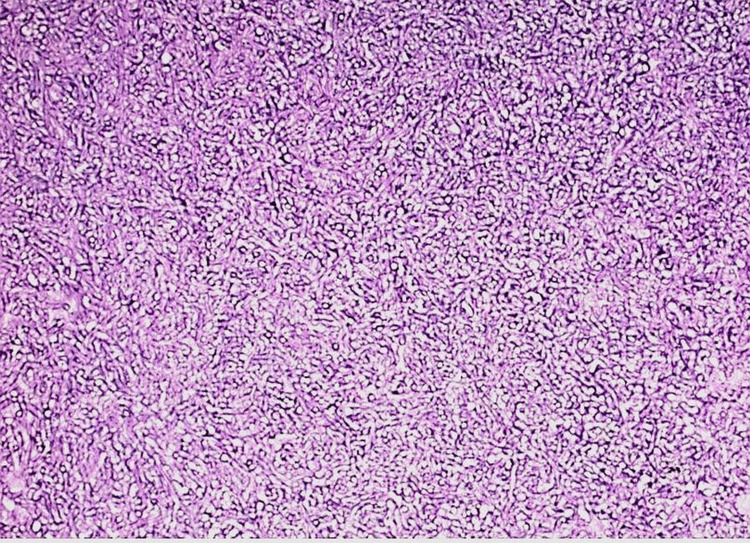 Figure 3
Figure 3| Author (Year) | Immune Status | Location Involved | Treatment | Outcome |
|---|---|---|---|---|
| Pushker et al. (2011) [ | Immunocompetent | Orbit + paranasal sinuses | Surgery + amphotericin | Recovered |
| Vazquez et al. (2016) [ | Borderline (ICU/critical illness) | Paranasal sinuses | Voriconazole monotherapy; combination therapy | Recovered |
| Apostolopoulou et al. (2020) [ | COVID-associated | Pulmonary + paranasal sinuses | Voriconazole | Recovered |
| Current Case (2025) | Borderline (chronic neutropenia) | Isolated sphenoid sinus | Surgery + amphotericin B + voriconazole | Recovered |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Sinusitis and nasal conditions · Myasthenia Gravis and Thymoma
Introduction
Invasive fungal sinusitis (IFS) is a rare but potentially lethal condition most commonly caused by *Aspergillus *spp. Although it traditionally affects severely immunocompromised patients, such as those with prolonged neutropenia or uncontrolled diabetes, it is increasingly recognized in individuals with partial or transient immune deficits, including those recovering from chemotherapy or receiving corticosteroids [1,2]. Clinical manifestations often mimic bacterial sinusitis, and delayed diagnosis may lead to serious complications, including bony erosion or intracranial invasion. This report presents an unusual case of isolated sphenoid sinus aspergillosis with bony erosion in a patient with chronic neutropenia and emphasizes the need for heightened clinical suspicion in borderline immunocompromised hosts [3-5].
Case presentation
A 75-year-old female with a history of hypertension, migraines, gastric cancer (status post-gastrectomy and chemotherapy in 2009), and mantle cell lymphoma (treated from September 2022 to January 2024) presented with worsening headaches over three months. She had recently completed a short course of corticosteroids for presumed inflammatory headaches. Her lymphoma treatment had been discontinued due to persistent neutropenia. On presentation, she was afebrile with stable vitals and a non-focal neurological exam. Head computed tomography (CT) without contrast showed opacification and bony erosion of the bilateral sphenoid sinuses without signs of orbital or intracranial involvement (Figure 1).
Axial CT image showing complete opacification of the bilateral sphenoid sinusesCT head without contrast demonstrates opacification of the sphenoid sinuses with associated osteogenesis and dehiscence of the posterior wall of the sphenoid sinus along the anterior wall of the sella.
The Otolaryngology-Head and Neck Surgery team performed bilateral endoscopic sphenoidotomy. The procedure was conducted using stereotactic, computer-assisted cranial navigation under general anesthesia.
Intraoperative findings showed bilateral sphenoid sinuses filled with purulent drainage and thick fungal mucin, consistent with fungal sinusitis. Diffuse inflammatory changes were noted in the surrounding sinus mucosa. The left sphenoid sinus exhibited bony dehiscence at the skull base; however, there was no evidence of cerebrospinal fluid (CSF) leak. Histopathology revealed septate hyphae with acute-angle branching consistent with non-fumigatus Aspergillus species (Figures 2-3). Concurrent culture grew Streptococcus pneumoniae, indicating a polymicrobial infection.
Hematoxylin and eosin–stained section of sphenoid tissue at 100× magnificationHematoxylin and eosin staining demonstrates necrotic tissue with a mixed inflammatory infiltrate and detached fungal elements (arrow).
Hematoxylin and eosin-stained section of sphenoid tissue at 200× magnificationHematoxylin and eosin staining demonstrates numerous fungal hyphae with characteristic 45-degree branching, forming a compact fungal ball.
The patient was initiated on intravenous liposomal amphotericin B at 3 mg/kg daily for 2 days, after which she was transitioned to oral voriconazole to complete a 12-week antifungal course. For the bacterial component, she received 2 days of intravenous ceftriaxone, followed by oral cefadroxil 500 mg every 12 hours for a total of 10 days. This regimen resulted in complete symptom resolution.
Discussion
This case highlights the evolving epidemiology of invasive fungal sinusitis. Although our patient had completed chemotherapy several months earlier, her chronic neutropenia and recent corticosteroid exposure likely predisposed her to infection. The isolated sphenoid involvement with osseous erosion and polymicrobial infection is particularly rare and underscores the importance of early multidisciplinary evaluation and imaging, involving the Otolaryngology-Head and Neck Surgery, Radiology, Infectious Diseases, and Internal Medicine teams [6,7].
Aspergillus fumigatus is the most frequently isolated species in IFS. Diagnosis typically relies on radiographic features, such as sinus opacification and bony destruction, endoscopic visualization, and histopathological confirmation. Standard treatment involves prompt surgical debridement in combination with systemic antifungal therapy [1,8,9].
The differential diagnosis included bacterial sinusitis and mucormycosis. Bacterial sinusitis is a more common cause of acute sinus infection; however, the invasive features seen on imaging, together with culture results, supported a fungal etiology [10]. Mucormycosis, another invasive fungal sinus infection, can present with overlapping clinical and radiographic findings [11]. In this case, the absence of angioinvasive features, such as tissue necrosis, along with the identification of Aspergillus on microbiological analysis, distinguished it from mucormycosis [12,13]. These distinctions were critical in guiding the antifungal management strategy.
Voriconazole is the preferred agent due to its improved efficacy and safety profile compared with amphotericin B [1,8,14]. In this case, amphotericin was selected initially because of disease severity and diagnostic uncertainty, with a successful transition to voriconazole once the fungal etiology was confirmed. The polymicrobial nature of this infection, involving both Aspergillus and Streptococcus pneumoniae, did not alter the antifungal strategy, as *Aspergillus *was considered the primary pathogen. The bacterial component was managed with a short course of antibiotics, which resolved the secondary infection without influencing the antifungal regimen or overall clinical outcome. Table 1 shows a comparison of the present case with selected reports in the literature.
This case also highlights the value of a multidisciplinary approach involving Internal Medicine, Otolaryngology-Head and Neck Surgery, Infectious Diseases, and Pharmacy [16]. Timely evaluation by the Otolaryngology-Head and Neck Surgery team enabled prompt surgical debridement, while Pharmacy support ensured appropriate antifungal dosing and monitoring, both of which contributed to a favorable outcome.
Conclusions
Sinus aspergillosis should be considered in elderly patients with chronic or treatment-resistant sinusitis, even when overt immunosuppression is not apparent. Patients with a history of chemotherapy, persistent neutropenia, or immunomodulatory treatment may be at elevated risk despite appearing immunocompetent. A high index of suspicion, timely imaging, surgical intervention, and appropriate antifungal therapy are essential for favorable outcomes. Increased clinician awareness of this underrecognized presentation may improve diagnostic and therapeutic timelines.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis N Engl J Med Herbrecht R Denning DW Patterson TF 40841534720021216768310.1056/NEJ Moa 020191 · doi ↗ · pubmed ↗
- 2Invasive pulmonary aspergillosis in patients with SARS-Co V-2 infection: a systematic review of the literature Diagnostics (Basel) Apostolopoulou A Esquer Garrigos Z Vijayvargiya P Lerner AH Farmakiotis D 8071020203305049910.3390/diagnostics 10100807 PMC 7600775 · doi ↗ · pubmed ↗
- 3Is neutropenia still the main risk factor for invasive aspergillosis? A contemporary university hospital retrospective cohort of invasive aspergillosis in neutropenic and non-neutropenic patients Ann Clin Microbiol Antimicrob Gutiérrez-Villanueva A Diego-Yagüe I Gutiérrez-Martín I 282420254028156910.1186/s 12941-025-00794-8PMC 12032692 · doi ↗ · pubmed ↗
- 4Sphenoid sinus aspergilloma in an immunocompetent and an immunocompromised patient: a case report Cureus Singh M Zaita BM Singh D Singh A Kaur G 015202310.7759/cureus.34517 PMC 998428136879700 · doi ↗ · pubmed ↗
- 5Aspergillosis of maxillary sinus's diagnosis, management, and association with COVID-19: a case report Cureus Rai D Shukla D Bhola ND 014202210.7759/cureus.30191 PMC 964890836397916 · doi ↗ · pubmed ↗
- 6The changing epidemiology of invasive aspergillosis in the non-traditional host Pulm Crit Care Med Vazquez JV Tovar-Torres MP Hingwe A Cheema F Welch VL Ford KD 12016
- 7Isolated invasive fungal sphenoid sinusitis-induced extensive bone erosion and severe meningoencephalitis: diagnosis and multidisciplinary management BMJ Case Rep Hallak B Teiga P Hedjoudje A Alvarez V 016202310.1136/bcr-2022-253788 PMC 1012421437085281 · doi ↗ · pubmed ↗
- 8Comparison of antifungal drugs in the treatment of invasive pulmonary aspergillosis: a systematic review and network meta-analysis Front Microbiol Cheng J Han H Kang W Cai Z Zhan P Lv T 15048261520243968787210.3389/fmicb.2024.1504826 PMC 11648418 · doi ↗ · pubmed ↗