Acute Encephalopathy and Severe Hypercalcemia as the Initial Presentation of a Large Parathyroid Hormone-Related Protein (PTHrP)-Secreting Pancreatic Neuroendocrine Tumor: A Case Report
Katherine M Collamore, Parul Jandir, Jennifer Hashem, Alejandro Cruz Ponce, Michael Levitt

TL;DR
A rare pancreatic tumor caused severe hypercalcemia and brain issues, showing how early diagnosis can improve outcomes.
Contribution
Highlights a rare initial presentation of a PTHrP-secreting pNET causing acute encephalopathy and severe hypercalcemia.
Findings
A 15 cm pancreatic tumor was found to secrete PTHrP, leading to severe hypercalcemia.
Neurologic symptoms improved after treating hypercalcemia with hydration, calcitonin, zoledronic acid, and dialysis.
Lanreotide therapy was initiated for managing the neuroendocrine tumor.
Abstract
Pancreatic neuroendocrine tumors (pNETs) are rare neoplasms that present with diverse clinical manifestations depending on their secretory activity. Paraneoplastic hypercalcemia due to parathyroid hormone-related peptide (PTHrP) secretion by pNETs is an uncommon but serious complication. We describe the case of a 67-year-old female with a past medical history of multiple sclerosis and uveitis presenting with acute metabolic encephalopathy due to profound hypercalcemia. Laboratory workup revealed a corrected calcium of 22.4 mg/dL and PTHrP of 327 pg/mL. Imaging demonstrated a new 15 cm pancreatic mass with adrenal nodules suspicious for metastatic disease. Pathology from a percutaneous biopsy confirmed a well-differentiated pNET with a Ki-67 index of ~15%. The patient’s mental status improved following treatment of hypercalcemia with intravenous hydration, calcitonin, zoledronic acid,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1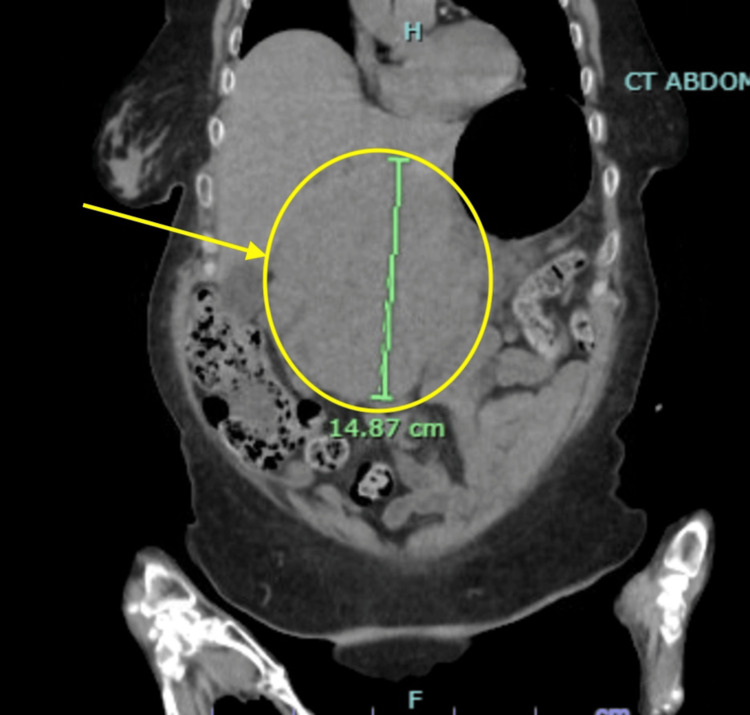 Figure 2
Figure 2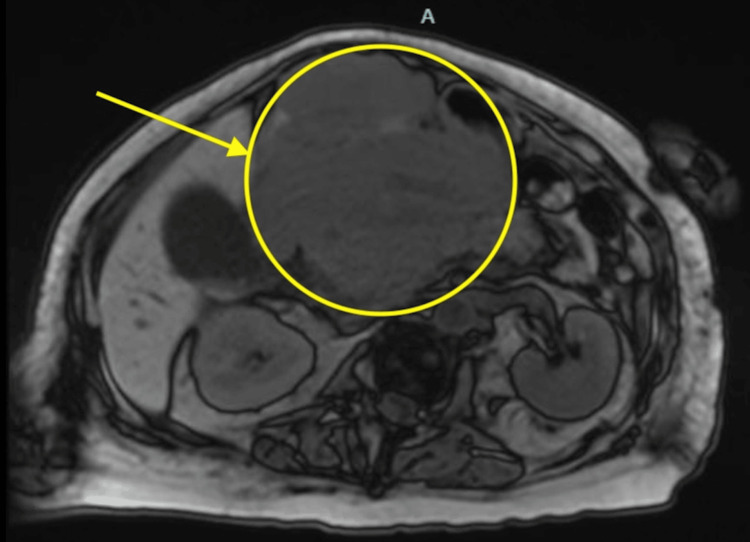 Figure 3
Figure 3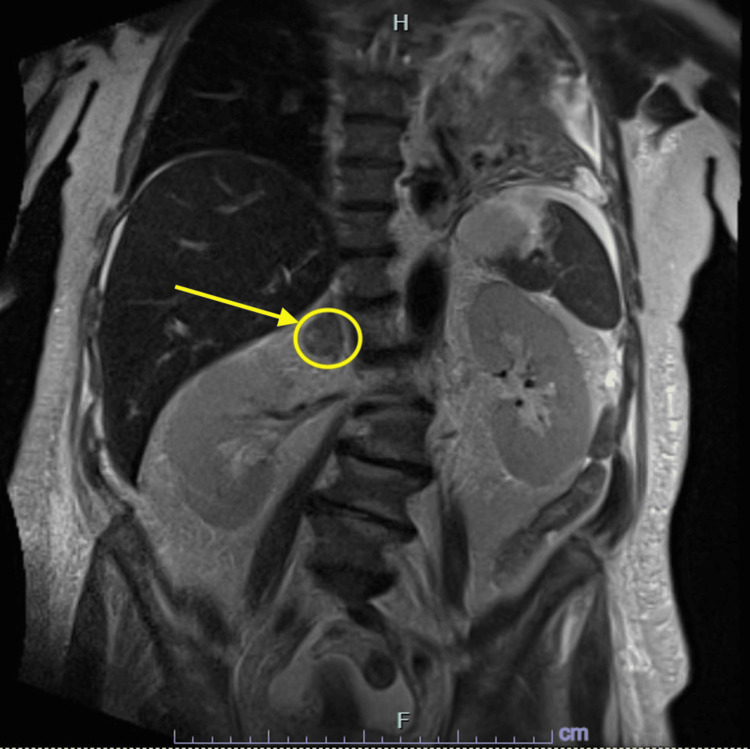 Figure 4
Figure 4| Vital signs | |
| Heart rate | 112 beats/minute |
| Blood pressure | 142/81 mmHg |
| Respiratory rate | 17 breaths/minute |
| Oxygen saturation (SpO2) | 97% |
| Laboratory studies | Patient results | Reference values |
| White blood cells | 21,000/µL | 4,500–11,000/µL |
| Neutrophil | 87% | 50–70% |
| Hemoglobin | 11.8 g/dL | 12–16 g/dL |
| Creatinine | 2.22 mg/dL | 0.55–1.02 mg/dL |
| Calcium | 21.6 mg/dL | 8.7–10.4 mg/dL |
| Corrected calcium | 22.4 mg/dL | 8.7–10.4 mg/dL |
| Magnesium | 2.71 mg/dL | 1.6–2.6 mg/dL |
| Creatinine kinase | 6,016 IU/L | 34–145 IU/L |
| Alkaline phosphatase | 145 U/L | 46–116 U/L |
| Aspartate aminotransferase | 388 U/L | 0–34 U/L |
| Alanine aminotransferase | 226 U/L | 10–49 U/L |
| Ferritin | 1,502.0 ng/mL | 7.3–270.7 ng/mL |
| Laboratory studies | Patient results | Reference values |
| Carcinoembryonic antigen | <2 | Non-smoker: <2.5 ng/mL; smoker: <5.0 ng/mL |
| Carbohydrate antigen 19-9 | <3 | <34 U/mL |
| Lactate dehydrogenase | 630 U/L | 120–246 U/L |
| Uric acid | 12.4 mg/dL | 3.1–7.8 mg/dL |
| Cancer antigen 125 | 155 U/mL | <35 U/mL |
| Chromogranin A | 841 ng/mL, 1,028 ng/mL | <311 ng/mL |
| Intact parathyroid hormone | 10.6 pg/mL | 18.4–88.0 pg/mL |
| Parathyroid hormone-related peptide | 327 pg/mL, 891 pg/mL | 11–20 pg/mL |
| Vitamin D 25 Hydroxy | 27.1 ng/mL | 30.0–100.0 ng/mL |
| Thyroid-stimulating hormone | 5.7 µIU/mL | 0.550–4.780 µIU/mL |
| Free thyroxine | 1.21 ng/dL | 0.89–1.76 ng/dL |
| Epinephrine | 17 pg/mL | Supine: <58 pg/mL; upright: <82 pg/mL |
| Norepinephrine | 337 pg/mL | Supine: 149-564 pg/mL; upright: 199-937 pg/mL |
| Dopamine | 11 pg/mL | Supine: <16 pg/mL; upright: <27 pg/mL |
| Total Catecholamines | 365 pg/mL | Supine: <632 pg/mL; upright: <1046 pg/mL |
| Plasma Renin Activity | 1.88 ng/mL.hour | 0.25–5.82 ng/mL.hour |
| Free metanephrine (plasma) | <25 pg/mL | 57 pg/mL |
| Free Normetanephrine (plasma) | 51 | 148 pg/mL |
| Free total metanephrines (plasma) | 51 | 205 pg/mL |
| Aldosterone | <1 ng/dL | Upright 8:00–10:00 am = 28 ng/dL; upright 4:00–6:00 pm = 21 ng/dL; supine 8:00–10:00 am = 3–16 ng/dL |
| Random urine sodium | 51 mmol/L | |
| Random urine creatinine | 41.08 mg/dL | 20.00–320.00 mg/dL |
| Ammonia | 19 µmol/L | 11–32 µmol/L |
| Vitamin B12 | 912 pg/mL | 211–911 pg/mL |
| Folate | 18.75 ng/mL | >5.38 ng/mL |
|
| ||
| Protein, total | 5.5 g/dL | 6.0–8.0 g/dL |
| Albumin | 2.95 g/dL | 3.2–5.0 g/dL |
| Alpha 1 globulins | 0.68 g/dL | 0.1–0.4 g/dL |
| Alpha 2 globulins | 0.87 g/dL | 0.6–1.0 g/dL |
| Beta globulins | 0.53 g/dL | 0.6–1.30 g/dL |
| Gamma globulins | 0.47 g/dL | 0.70–1.50 g/dL |
| AG ratio | 1.16 | >1.00 |
| Kappa Qt free light chains | 29.40 mg/L | 3.30–19.40 mg/L |
| Lambda Qt free light chains | 13.72 mg/L | 5.71–26.30 mg/L |
| Kappa-lambda free light chains ratio | 2.14 | 0.26–1.65 |
| Date/Time | Reference values | 4/7/25 15:17 | 4/8/25 04:54 | 4/8/25 10:50 | 4/8/25 22:55 | 4/9/25 04:50 | 4/9/25 17:39 | 4/10/25 06:20 | 4/10/25 18:53 | 4/11/25 03:41 | 4/11/25 18:43 | 4/12/25 04:55 | 4/13/25 05:18 | 4/14/25 06:22 | 4/15/25 05:33 | 4/16/25 05:17 |
| Glucose, mg/dL | 70–99 | 75 | 80 | 66 | 68 | 61 | 94 | 116 | 173 | 268 | 125 | 128 | 117 | 96 | 76 | 100 |
| Sodium, mmol/L | 136–145 | 140 | 139 | 139 | 140 | 142 | 139 | 141 | 144 | 142 | 142 | 140 | 141 | 139 | 142 | 143 |
| Potassium, mmol/L | 3.5–5.1 | 3.4 | 3.9 | 4.5 | 3.7 | 3.9 | 3.1 | 3.2 | 3.6 | 3.5 | 3.1 | 3.7 | 3.5 | 3.6 | 3.0 | 3.2 |
| Chloride, mmol/L | 98–107 | 102 | 105 | 107 | 104 | 106 | 103 | 103 | 107 | 106 | 106 | 105 | 105 | 104 | 103 | 108 |
| CO2, mmol/L | 20–31 | 27 | 25 | 17 | 26 | 25 | 28 | 25 | 24 | 23 | 25 | 23 | 26 | 21 | 25 | 25 |
| Blood urea nitrogen, mg/dL | 9–23 | 57 | 60 | 47 | 28 | 30 | 14 | 18 | 24 | 26 | 28 | 30 | 36 | 34 | 29 | 22 |
| Creatinine, mg/dL | 0.55–1.02 | 2.22 | 2.14 | 2.19 | 1.33 | 1.54 | 0.91 | 1.21 | 1.42 | 1.47 | 1.39 | 1.36 | 1.18 | 0.98 | 0.89 | 0.70 |
| Estimated glomerular filtration rate, mL/min/1.73m2 | >/= 60 | 24 | 25 | 24 | 44 | 37 | >/= 60 | 49 | 41 | 39 | 42 | 43 | 51 | >/= 60 | >/= 60 | >/= 60 |
| Anion gap, mmol/L | 5–15 | 11 | 9 | 15 | 10 | 11 | 8 | 13 | 13 | 13 | 11 | 12 | 10 | 14 | 14 | 10 |
| Phosphorus, mg/dL | 2.4–5.1 | 4.3 | 1.7 | 2.9 | 1.5 | |||||||||||
| Magnesium, mg/dL | 1.6–2.6 | 2.71 | 2.62 | 1.87 | 1.58 | 1.51 | 1.55 | 1.43 | 1.31 | 1.40 | 1.28 | |||||
| Calcium, mg/dL | 8.7-10.4 | 21.6 | 19.7, 19.6 | 18.9 | 13.5 | 13.6 | 10.5 | 11.5 | 11.7 | 10.9 | 10.8 | 10.4 | 9.8 | 9.4 | 8.2 | 8.1 |
| Corrected calcium | 22.4 | 20.6 | 19.8 | 14.6 | 14.6 | 11.8 | 12.8 | 13.1 | 12.3 | 12.1 | 11.6 | 11.2 | 10.6 | 9.4 | 9.4 | |
| Albumin, g/dL | 3.4–5.0 | 3.0 | 2.7 | 2.9 | 2.6 | 2.8 | 2.4 | 2.4 | 2.3 | 2.3 | 2.4 | 2.5 | 2.2 | 2.5 | 2.5 | 2.4 |
| AG ratio | >1.0 | 0.9 | 0.9 | 0.8 | 0.8 | 0.8 | 0.8 | 0.7 | 0.7 | 0.7 | 0.7 | 0.7 | 0.6 | 0.7 | 0.6, 0.6 | 0.7 |
| Protein total, g/dL | 6.0–8.0 | 6.5 | 5.8 | 6.4 | 6.0 | 6.2 | 5.5 | 5.7 | 5.5 | 5.7 | 6.0 | 5.9 | 5.6 | 6.1 | 6.6 | 5.9 |
| Bilirubin total, mg/dL | 0.2–1.3 | 0.6 | 0.9 | 0.7 | 0.7 | 0.7 | 1.5 | 1.5 | 0.8 | 0.5 | 0.6 | 0.5 | 0.4 | 0.3 | 0.4 | 0.4 |
| Alkaline phosphatase, U/L | 46–116 | 145 | 137 | 142 | 326 | 388 | 587 | 567 | 615 | 507 | 728 | 621 | 443 | 392 | 428 | 349 |
| Aspartate aminotransferase, U/L | 0–34 | 388 | 498 | 498 | 514 | 502 | 557 | 484 | 361 | 222 | 177 | 116 | 59 | 51 | 38 | 30 |
| Alanine Aminotransferase, U/L | 10–49 | 226 | 289 | 306 | 368 | 408 | 509 | 510 | 507 | 408 | 382 | 313 | 218 | 159 | 149 | 101 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine Tumor Research Advances · Bone health and treatments · Fibroblast Growth Factor Research
Introduction
Neuroendocrine tumors (NETs) are rare neoplasms originating from neuroendocrine cells and demonstrate a wide spectrum of clinical and biochemical profiles depending on their anatomical site and secretory activity. Among these, pancreatic neuroendocrine tumors (pNETs) comprise 5% of all pancreatic tumors and 7% of all NETs [1]. These tumors are categorized as functional, meaning they secrete pancreatic hormones such as insulin or glucagon, or nonfunctional, meaning they do not secrete hormones [2]. Nonfunctional tumors typically present later, with symptoms resulting from tumor burden, mass effect, or metastatic disease [3].
Paraneoplastic hypercalcemia is a rare but serious complication of pNETs, most often mediated by secretion of parathyroid hormone-related peptide (PTHrP) [4]. Hypercalcemia of malignancy is a common metabolic complication seen in up to 30% of cancer patients, particularly those with squamous cell carcinoma, renal cell carcinoma, and breast cancer [2,5-7]. Although rarely seen in NETs, recent case reports of PTHrP-producing pNETs causing severe hypercalcemia requiring intensive treatments suggest that this phenomenon may be underrecognized and clinically significant [2,6-11,12].
We present the case of a well-differentiated pNET in a patient with acute encephalopathy due to profound hypercalcemia from elevated PTHrP. This case underscores the importance of considering pNETs in the differential diagnosis of hypercalcemia of unclear etiology. This report adds to growing evidence of the diverse clinical manifestations of PTHrP-secreting pNETs, emphasizing the need for clinical vigilance and timely diagnostic workup in patients with unexplained hypercalcemia and neurologic symptoms.
Case presentation
Emergency department course
A 67-year-old female with a past medical history of multiple sclerosis and uveitis presented to the emergency department with confusion and slurred speech after being found down by family. The patient was agitated, required frequent redirection, and answered questions intermittently. The patient’s husband provided the majority of the initial history due to the patient’s confusion and inattention. He reported that she had poor appetite, low energy, and a 40 lb weight loss in the previous six months, as well as constipation. The husband also confirmed that the patient’s current behavior and confusion were an acute change from her baseline, which was fully oriented to person, place, and time with the ability to attend to and actively participate in conversation. Initial vital signs in the emergency department are shown in Table 1.
Significant laboratory results in the emergency department are shown in Table 2.
Table 2: Laboratory values of significance from the emergency department.The table displays significant laboratory values from tests conducted in the emergency department upon the patient’s initial presentation. They are significant for leukocytosis (white blood cell count > 11,000/µL) with a left shift (neutrophils >70%), mild anemia (hemoglobin <12 g/dL), kidney dysfunction evidenced by elevated creatinine (>1.02 mg/dL) and accompanied by electrolyte abnormalities, including hypermagnesemia (magnesium >2.6 mg/dL) and severe hypercalcemia (calcium >>10.4 mg/dL). Additionally, results showed muscle injury evidenced by elevated creatinine kinase (>145 IU/L), liver injury evidenced by elevated liver function tests (alkaline phosphatase >116 U/L, aspartate aminotransferase >34 U/L, alanine aminotransferase >49 U/L), and chronic inflammation suggested by elevated ferritin (ferritin >270.7 ng/mL), an acute-phase reactant.
Due to her altered mental status, the patient underwent a non-contrast head CT scan, which was unremarkable. Elevated liver function tests were investigated further with a non-contrast CT of the abdomen and pelvis (CTAP), which revealed a 15.2 × 11.4 × 14.9 cm abdominal mass involving the head and body of the pancreas, notably without significant dilation of the pancreatic or biliary ducts. The mass also impinged on the duodenum but caused no gastric outlet obstruction. Evidence of suspicious metastatic disease was also present on initial CTAP, including a focal sclerotic lesion at the 12th thoracic vertebra (T12) as well as bilateral (R>L) adrenal masses (Figures 1, 2).
Axial view of the initial CT of the chest, abdomen, and pelvis.The image displays an axial cross-section from the patient’s CT scan of the chest, abdomen, and pelvis, obtained in the emergency department due to elevated liver function tests (see Table 2). The yellow circle and arrow indicate a large abdominal mass measuring 11.40 cm × 15.22 cm.
Coronal view of the initial CT of the chest, abdomen, and pelvis.The image displays a coronal cross-section from the patient’s CT scan of the chest, abdomen, and pelvis, obtained in the emergency department due to elevated liver function tests (see Table 2). The yellow circle and arrow indicate a large abdominal mass measuring a length of 14.87 cm. This is a different view of the same CT scan and the same mass indicated in Figure 1.
In the emergency department, the patient received a 1 L bolus of normal saline, one dose of piperacillin-tazobactam 3.375 g in D5W 50 mL, one dose of vancomycin 1 g in normal saline 250 mL, and potassium chloride 20 mEq in 100 mL.
Hospital course
Follow-up MRI in the form of magnetic resonance cholangiopancreatography showed the large abdominal mass, a right adrenal mass, and a distended gallbladder, with no gallstones, gallbladder wall thickening, or common bile duct obstruction (Figures 3, 4).
Axial view of magnetic resonance cholangiopancreatography.The image displays an axial cross-section of the patient’s magnetic resonance cholangiopancreatography scan taken during hospital admission to better visualize the origin of the abdominal mass. The yellow arrow and circle highlight the large abdominal mass, as seen on initial CT scan in Figures 1, 2.
Coronal view of magnetic resonance cholangiopancreatography.The image displays a coronal cross-section of the patient’s magnetic resonance cholangiopancreatography scan taken during hospital admission. The yellow arrow and circle draw attention to a right adrenal nodule, which may be an incidental finding or suggestive of metastatic disease.
Further workup included tumor marker studies, endocrine studies, ammonia, vitamin B12, folate, and a serum protein electrophoresis. Results are displayed in Table 3.
The patient’s hypercalcemia was treated with aggressive hydration, calcitonin 300 units every 12 hours for a total of four doses, zoledronic acid 4 mg intravenously once, and emergent hemodialysis for two days. Hemodialysis was delivered through a central venous catheter in the right internal jugular vein, placed by vascular surgery. Improvement in her comprehensive metabolic panel is shown in Table 4.
The patient’s mental status was formally assessed with regular mental status and neurologic examinations, which documented marked improvement in functioning following these treatments. Initial mental status and neurologic examinations demonstrated confusion, limited speech, inability to identify objects, limited answers to questions, and poor command following. In contrast, her examination on the day of discharge demonstrated that the patient was alert and oriented to person, place, and time and conversing appropriately with fluent speech.
During her hospitalization, the patient also underwent interventional radiology percutaneous biopsy of the abdominal mass, from which pathology revealed a well-differentiated NET. The tumor cells were arranged in highly vascularized trabeculae or nests and stained positive for AE1/3, synaptophysin, chromogranin (weak), and CD56. They stained negative for CK7, CK20, CDX2, GATA3, and TTF-1. The Ki-67 proliferative index was ~15%.
Pertinent outpatient follow-up
After discharge, the patient underwent an outpatient positron emission tomography scan for initial NET staging, which showed pathologic radiotracer uptake in the known abdominal mass, which was indistinguishable from the head of the pancreas. Additionally, there was uptake in a nodule located between the tail of the pancreas and the splenic hilum, thought to be a splenule, though an active lymph node could not be ruled out. Physiologic uptake of the radiotracer in the adrenal glands limited the evaluation of the right adrenal nodule, with further imaging recommended. Additionally, there was a new subpleural nodule in the right lower lung measuring 17 × 15 mm, which did not exhibit abnormal radiotracer uptake, though continued follow-up was recommended.
The patient continued to follow up as an outpatient with the oncology team and was started on lanreotide (somatuline) 120 mg every four weeks. The patient also followed up with the endocrinology team for monitoring of her adrenal nodule and nephrology for monitoring of her kidney function and fluid-electrolyte balance.
Discussion
pNETs are a rare and heterogeneous group of neoplasms with diverse clinical presentations depending on functional status, tumor size, and metastatic burden [9]. While functional pNETs may produce distinct hormone-related syndromes, nonfunctional pNETs frequently present late, often as large masses with metastatic disease [5]. This case highlights an uncommon manifestation of a well-differentiated pNET with paraneoplastic hypercalcemia and altered mental status, an unusual and clinically significant presentation.
Hypercalcemia of malignancy is a well-established paraneoplastic syndrome and is most commonly mediated by the secretion of PTHrP. However, the secretion of PTHrP is typically associated with specific types of cancer, including squamous cell carcinoma, renal cell carcinoma, and breast cancer [13]. NETs rarely produce PTHrP. However, our patient came to medical attention due to acute metabolic encephalopathy and was subsequently found to have a markedly elevated serum calcium level (22.4 mg/dL) and PTHrP (327 pg/mL). Elevated liver enzymes prompted imaging evaluation with an abdominal CT, revealing a large mass arising from the pancreatic head. Therefore, paraneoplastic syndrome due to an underlying malignancy was suspected. Acute management was required due to the patient’s significantly altered mental status, which included intravenous hydration, bisphosphonates, calcitonin, and urgent hemodialysis. After several days of treatment with these aggressive measures, her calcium was corrected to a normal serum level, and with that came improvement in her mental status, which ultimately returned to baseline, underscoring the neurologic impact of this metabolic derangement [14].
Several case reports have been published in recent years regarding instances of refractory hypercalcemia in patients with pNETs. Many report the development of hypercalcemia several months or years after the initial diagnosis [4,7,15]. Others describe cases of pNETs with hypercalcemia present at the time of diagnosis [2,9,10,13,16-18]. There is also a wide range of symptom severity, severity of the calcium elevation, and treatments required to normalize calcium levels among these patients. This case adds to the literature, representing that great diversity in the time course, clinical symptoms, severity, and necessary interventions exists among patients with hypercalcemia of malignancy due to PTHrP-secreting pNETs.
Conclusions
In summary, this case illustrates altered mental status due to paraneoplastic hypercalcemia as the initial manifestation of a pNET, emphasizing the importance of pNETs as part of the differential diagnosis of hypercalcemia. Early recognition and appropriate biochemical and histological workup are essential for prompt treatment initiation, which improves patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Islet cell tumors of the pancreas Gastroenterol Clin North Am Amin S Kim MK 831004520162689568210.1016/j.gtc.2015.10.007 · doi ↗ · pubmed ↗
- 2Pancreatic neuroendocrine tumor with humoral hypercalcemia and high tumor PD-L 1 score Oncology (Williston Park) Copur MS Vargas L Wedel W Merani S Cushman-Vokoun A Drincic A 5485523420203339549610.46883/ONC.2020.3412.0548 · doi ↗ · pubmed ↗
- 3Diagnosis and management of neuroendocrine tumours Clin Med (Lond) Cuthbertson DJ Shankland R Srirajaskanthan R 1191242320233695884210.7861/clinmed.2023-0044 PMC 11046558 · doi ↗ · pubmed ↗
- 4Hypercalcemia of malignancy: an update on pathogenesis and management N Am J Med Sci Mirrakhimov AE 48349372015 https://pubmed.ncbi.nlm.nih.gov/26713296/2671329610.4103/1947-2714.170600 PMC 4683803 · doi ↗ · pubmed ↗
- 5Pancreatic neuroendocrine tumors (PNE Ts): incidence, prognosis and recent trend toward improved survival Ann Oncol Halfdanarson TR Rabe KG Rubin J Petersen GM 172717331920081851579510.1093/annonc/mdn 351PMC 2735065 · doi ↗ · pubmed ↗
- 6Unusual complication of a pancreatic neuroendocrine tumor presenting with malignant hypercalcemia J Clin Endocrinol Metab Kanakis G Kaltsas G Granberg D Grimelius L Papaioannou D Tsolakis AV Öberg K 03197201210.1210/jc.2011-259222319031 · doi ↗ · pubmed ↗
- 7Clinical practice. Hypercalcemia associated with cancer N Engl J Med Stewart AF 37337935220051567380310.1056/NEJ Mcp 042806 · doi ↗ · pubmed ↗
- 8Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States JAMA Oncol Dasari A Shen C Halperin D 13351342320172844866510.1001/jamaoncol.2017.0589 PMC 5824320 · doi ↗ · pubmed ↗