Role of Ultrasound in Tracheotomy and Cricothyrotomy: A Research Study of Midline Cervical Vasculature in Healthy Individuals
Okechukwu Nkwocha, Chinedu J Enwerem, Michael Adeniyi, Tarek Alambrouk, Unaiza Jawad, Sadia Javed, Haider Hilal

TL;DR
This study shows that ultrasound can detect midline neck blood vessels in healthy people, suggesting it should be used more often during airway procedures to prevent injuries.
Contribution
The study provides empirical evidence on the prevalence of midline cervical vasculature in healthy individuals and advocates for routine ultrasound use in airway procedures.
Findings
Midline vascular structures were found in 28.7% of healthy individuals using ultrasound.
Most vessels were located at the thyroid isthmus level (22.5%).
No consistent guidelines recommend routine ultrasound use for tracheotomy or cricothyrotomy.
Abstract
Introduction Tracheotomy and cricothyrotomy are life-saving airway interventions that carry a risk due to the presence of midline vascular structures in the anterior neck. Injury to these structures during blind landmark-based procedures can lead to serious complications. Ultrasound (US) is a non-invasive, real-time imaging modality that enables direct visualization of cervical anatomy and vascular variants. Despite its advantages, its routine use is not yet standardized in clinical protocols. This study aims to evaluate the prevalence of midline vasculature using US in healthy individuals and to review current guidelines regarding US use in airway access. The aim of the study is to assess the prevalence of midline cervical vasculature using US in healthy adults and to review national and international guidelines on US use in tracheotomy and cricothyrotomy procedures. Methods This…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
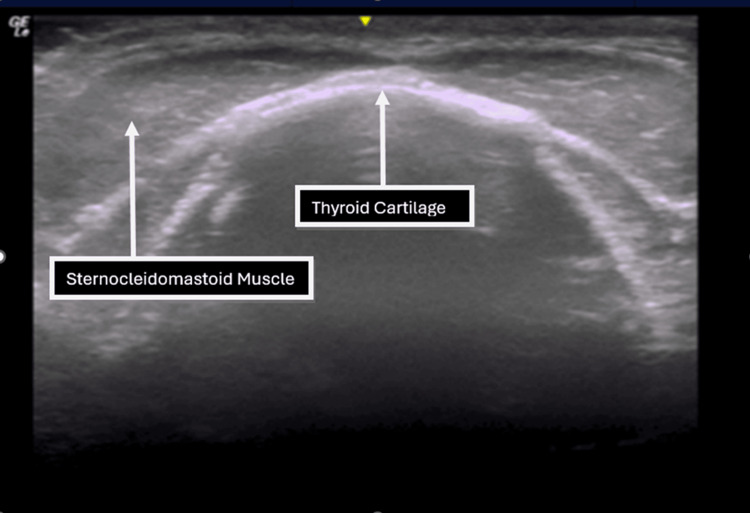 Figure 1
Figure 1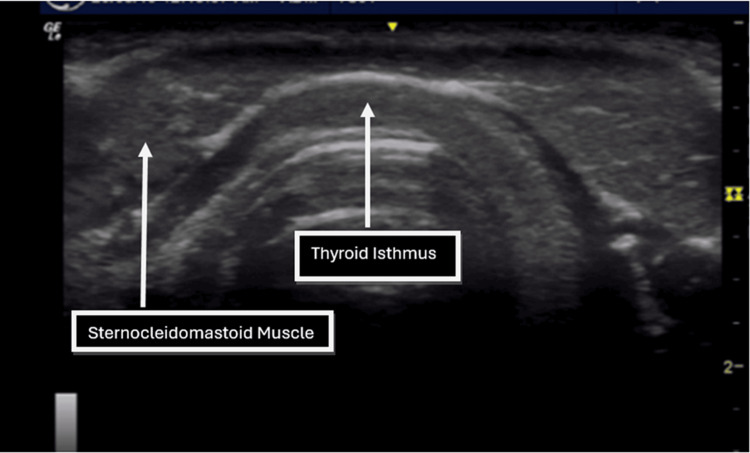 Figure 2
Figure 2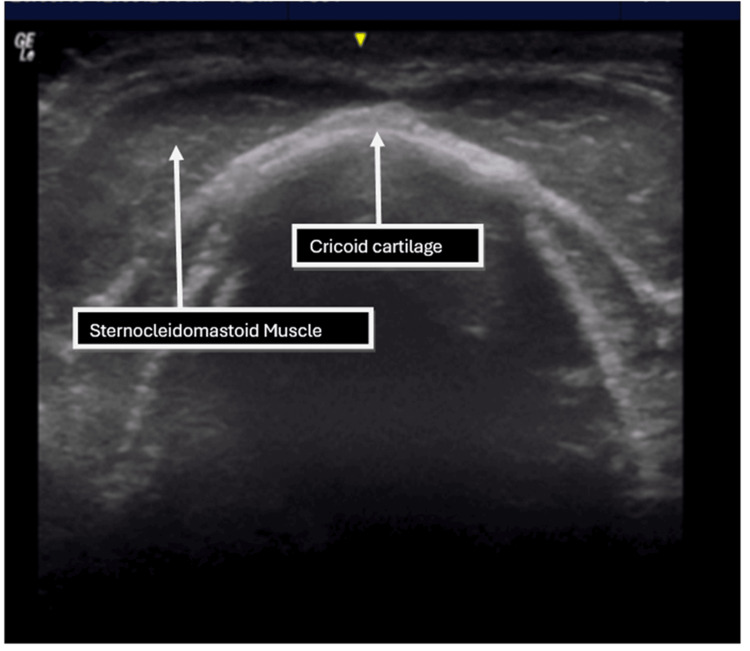 Figure 3
Figure 3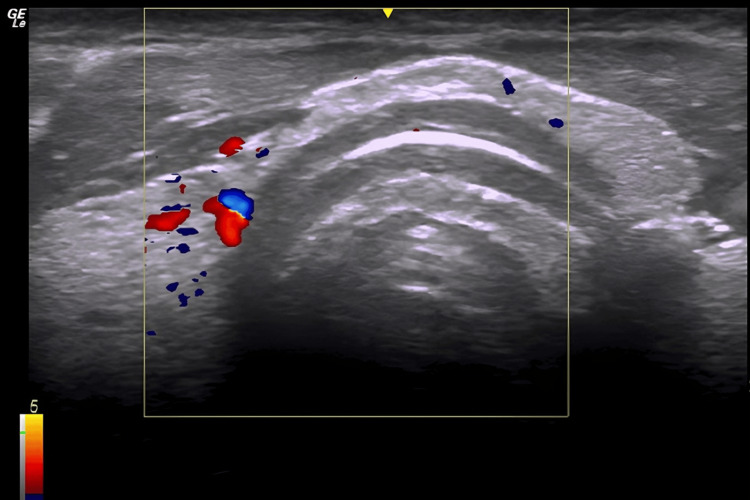 Figure 4
Figure 4| Anatomical Landmark | Participants With Midline Vessels (n) | Total Participants (N) | Prevalence (%) | 95% CI (Clopper-Pearson Exact) (%) |
| Inferior edge of the thyroid isthmus | 18 | 80 | 22.5 | 13.7-32.8 |
| Superior border of the cricoid cartilage | 3 | 80 | 3.8 | 0.8-10.7 |
| Inferior border of the thyroid cartilage | 2 | 80 | 2.5 | 0.3-8.7 |
| Variable | Vessels Present, n (%) | Vessels Absent, n (%) | χ² (df) | p-Value | |
| Gender | 0.150 (1) | 0.699 | |||
| Male | 14 (30.4) | 32 (69.6) | |||
| Female | 9 (26.5) | 25 (73.5) | |||
| Ethnicity | 0.338 (3) | 0.953 | |||
| White (n=53) | 15 (28.3) | 38 (71.7) | |||
| Black (n=11) | 3 (27.3) | 8 (72.7) | |||
| Asian (n=11) | 3 (27.3) | 8 (72.7) | |||
| Mixed (n=5) | 2 (40.0) | 3 (60.0) |
| Demographics | n (%)/Mean | |
| Age (years) | 25.4 ± 7.2 (18-49) | |
| Gender | Male | 46 (57.5%) |
| Female | 34 (42.5%) | |
| Ethnicity | White | 53 (66.3%) |
| Black | 11 (13.8%) | |
| Asian | 11 (13.8%) | |
| Mixed | 5 (6.3%) | |
| BMI (kg/m²) | 22.7 ± 3.3 (17-29) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTracheal and airway disorders · Airway Management and Intubation Techniques · Voice and Speech Disorders
Introduction
Tracheotomy, the surgical creation of an airway opening in the trachea, is one of the oldest known surgical procedures, with origins dating back to ancient medical texts [1]. Early descriptions resembling tracheotomy appear in documents such as the Ebers Papyrus (circa 1550 BC) and the Sushruta Samhita (circa 600 BC), underscoring the longstanding recognition of securing the airway in emergencies [1]. Over centuries, the procedure evolved through the works of Greek and Renaissance physicians, including Antyllus in the 2nd century AD and Antonio Musa Brasavola in the 16th century, who performed the first documented successful tracheotomy [2]. These developments laid the foundation for modern airway management techniques.
Today, tracheotomy and cricothyrotomy remain vital, life-saving interventions used to bypass upper airway obstruction in both elective and emergency settings [3]. However, these procedures carry risks, particularly the inadvertent injury to vascular structures located in the anterior midline of the neck. Such injuries can cause serious complications, including hematoma, airway obstruction, and even mortality [4]. Previous studies have reported that vascular structures may be present in the midline neck region in a significant proportion of patients, with prevalence estimates reaching up to 41%, highlighting a clinically significant risk during blind landmark-based procedures [5].
Ultrasound (US) has emerged as a non-invasive and portable imaging modality that enables real-time visualization of neck anatomy, including tracheal landmarks and critical vasculature [5]. Its use can enhance the safety and accuracy of tracheotomy and cricothyrotomy by helping clinicians identify individual anatomical variations and avoid vascular injury. Despite this, US guidance is not yet routinely incorporated into airway management protocols [6].
This study aims to investigate the prevalence of midline vascular structures in the anterior neck region relevant to tracheotomy and cricothyrotomy and to evaluate the role of US in reducing procedural risks. By enhancing anatomical understanding and procedural safety, this research supports the advancement of airway management practices toward greater patient safety.
Materials and methods
This cross-sectional observational US study was conducted on 80 healthy adult volunteers. All participants had no prior history of tracheotomy or cricothyrotomy and no known neck pathology. Volunteers were recruited from university staff and students through convenience sampling. Individuals with a history of neck trauma, surgery, tumors, vascular malformations, or other neck-related disorders were excluded to minimize anatomical variability. Exclusion criteria were confirmed using self-report and brief physical examination.
US equipment and operator
US examinations were carried out using a GE LOGIQ e ultrasound system (GE Healthcare, Chicago, IL) equipped with a 12L-RS linear transducer (5-12 MHz). All scans were performed by a physician with more than five years’ experience in clinical US, ensuring procedural consistency and reducing inter-observer variability.
US procedure
Each volunteer was positioned supine with the head in slight extension and the upper body elevated to approximately 30-45 degrees, simulating a clinically relevant airway access posture used in tracheotomy and cricothyrotomy procedures. A transverse (short-axis) US scan was performed using the linear probe placed transversely across the neck at three specific anatomical levels:
1. Inferior border of the thyroid cartilage
2. Superior border of the cricoid cartilage
3. Inferior edge of the thyroid isthmus.
At each level, the probe was adjusted for optimal image acquisition. The presence or absence of midline vascular structures was noted. Vessels were defined as compressible (veins) or pulsatile/non-compressible (arteries), though detailed vessel classification was not consistently possible across all participants. All US images were reviewed in real time during the scan and again post-scan to confirm findings. The primary outcome was the presence or absence of midline vascular structures at each of the three predefined anatomical levels (Figures 1-3).
Transverse ultrasound image at the level of the inferior border of the thyroid cartilage.
Transverse ultrasound image at the level of the inferior border of the thyroid isthmus.
Transverse ultrasound image at the level of the superior border of the cricoid cartilage.
Data analysis
Data were recorded in a standardized spreadsheet, and statistical analysis was performed using SPSS version 26.0 (IBM Corp., Armonk, NY). Descriptive statistics were used to calculate the prevalence of midline vascular structures at each level, expressed as percentages and with corresponding 95% confidence intervals (CIs).
Comparative analyses were conducted to evaluate the relationship between the presence of midline vasculature and demographic variables (sex, BMI, and ethnicity). Chi-square tests were applied for categorical variables, and logistic regression was used to identify any independent associations. The prevalence of midline vascular structures at each anatomical level was reported with corresponding 95% CIs using the exact (Clopper-Pearson) method. A p-value <0.05 was considered statistically significant. A priori sample size calculation was not performed; the study size was based on feasibility and is acknowledged as a limitation.
Results
A total of 80 healthy volunteers were scanned (46 male volunteers and 34 female volunteers), with an age range of 18-49 years (mean age: 25.4 ± 7.2). US imaging revealed the presence of midline vessels in 23 participants (28.7%), as shown in Figure 4, whereas 57 (71.3%) participants did not have midline vessels.
Transverse ultrasound image showing vessels around thyroid gland.
US imaging also revealed variable prevalence of midline vascular structures at different anatomical landmarks in the cervical region, as seen in Table 1. At the level of the inferior edge of the thyroid isthmus, midline vascular structures were identified in 18 participants (22.5%). At the level of the superior border of the cricoid cartilage, midline vasculature was seen in three participants (3.8%). At the inferior border of the thyroid cartilage, vascular presence was lowest, observed in only two participants (2.5%).
Importantly, in this study, the presence of midline vessels showed no significant association with gender (χ²(1) = 0.15, p = 0.699) or ethnicity (χ²(3) = 0.34, p = 0.953), suggesting that these vascular variations occur independently of demographic factors, as shown in Table 2. There was no statistically significant correlation between the presence of midline vasculature and sex, BMI, or ethnicity (p > 0.05 across comparisons using chi-square or Fisher’s exact test as appropriate). These results suggest that vascular variation in this region is not easily predictable based on patient demographics, as shown in Table 3.
Discussion
The study offers critical insights into the anatomical variations of anterior neck vasculature and their implications for airway management procedures such as tracheotomy and cricothyrotomy. Among the study participants, vascular prevalence at the cricothyrotomy level was markedly lower (2.5-3.8%), supporting its relative safety as an emergency airway procedure. Our findings are also consistent with previous studies. For example, cadaveric studies have identified midline vasculature, particularly the inferior thyroid vein, in up to 97.5% of specimens [7] while live imaging studies reported lower rates ranging from 0.16% to 48.8%, because smaller venous branches may have been missed [8,9].
This presence of midline vessels is clinically relevant and highlights the risk of vascular injury that may often be overlooked when these procedures are performed without image guidance. Common risks associated with these procedures include hemorrhage, hematoma, and airway compromise. These risks may be magnified in patients with obesity, neck tumors, or distorted anatomy, where surface landmarks are unreliable [10]. Importantly, national and international guidelines, including American Society of Anesthesiologists (ASA) and Difficult Airway Society (DAS) recommendations, do not currently mandate routine pre-procedural US [11], which highlights a gap between emerging evidence and practice. One possible reason why ASA and DAS do not mandate pre-procedural US could possibly be because of emergency timing, limited operator availability, or lack of access to equipment in resource-poor settings.
US offers the advantages of portability, real-time imaging, and non-invasiveness. By detecting patient-specific anatomical variations it provides a low-cost means to prevent vascular complications and enhance procedural safety. Its use enables precise identification of the trachea, cricothyroid membrane, and adjacent vasculature, thereby significantly reducing the risk of inadvertent injury [11].
Beyond the technical and safety benefits, the US also holds educational value. Its integration into medical training enhances anatomical understanding, improves procedural confidence, and fosters early competence in airway management techniques [12]. Several studies have shown that exposure to the US at the undergraduate or early postgraduate level leads to improved clinical outcomes and decision-making, especially in high-stakes environments [13,14]. Importantly, in this study, the presence of midline vessels showed no significant association with gender (χ²(1) = 0.15, p = 0.699) or ethnicity (χ²(3) = 0.34, p = 0.953), suggesting that these vascular variations occur independently of demographic factors.
The small sample size limits the generalizability of the findings. In addition, the use of convenience sampling from a single center may limit representativeness. Finally, resource constraints, including limited access to multiple operators and equipment, prevented assessment of inter-operator variability and restricted the scope of data collection.
Future research should involve larger, multicenter cohorts with heterogeneous populations and include inter-operator reliability assessments. Studies conducted in emergency settings would also help determine whether the US can be feasibly integrated into time-critical airway management.
Conclusions
This study highlights the clinically significant presence of midline vascular structures in the anterior neck, particularly at the level of the thyroid isthmus, in healthy individuals, as detected via high-resolution US. These findings highlight the potential risk of vascular injury during tracheotomy procedures performed using traditional landmark-based methods. In contrast, the incidence of vascular structures at levels associated with cricothyrotomy was notably lower, supporting its relative safety in emergency airway management. US, as a non-invasive, portable, and real-time imaging modality, offers clear advantages in both elective and emergent airway procedures. Its ability to identify individual anatomical variations, particularly vascular anomalies, makes it an essential adjunct to safe airway access. In conclusion, the integration of point-of-care US into tracheotomy and cricothyrotomy practice represents a critical step forward in improving safety and reducing avoidable complications in airway management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tracheostomy Stat Pearls [Internet] Raimonde AJ Westhoven N Winters R Treasure Island, FL Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 559124/
- 2Tracheostomy: From surgical to percutaneous techniques Percutaneous Tracheostomy in Critically Ill Patients Servillo G Pelosi P Cham Springer 2016
- 3Management of difficult tracheal intubation: A closed claims analysis Anesthesiology Joffe AM Aziz MF Posner KL Duggan LV Mincer SL Domino KB 81882913120193158488410.1097/ALN.0000000000002815 PMC 6779339 · doi ↗ · pubmed ↗
- 4Complications of cricothyroidotomy versus tracheostomy in emergency surgical airway management: A systematic review BMC Anesthesiol Zasso FB You-Ten KE Ryu M Losyeva K Tanwani J Siddiqui N 2162020203285462610.1186/s 12871-020-01135-2PMC 7450579 · doi ↗ · pubmed ↗
- 5The ultrasound neck imaging for tracheostomy study: A study prompting ultrasound screening prior to percutaneous tracheostomy procedures to improve patient outcomes J Intensive Care Soc Rees J Haroon Y Hogan C Saha S Derekshani S 1071131920182979606610.1177/1751143717739570 PMC 5956683 · doi ↗ · pubmed ↗
- 6Endoscopic percutaneous dilatational tracheotomy: A prospective evaluation of 500 consecutive cases Laryngoscope Kost KM 130115200510.1097/01.MLG.0000163744.89688.E 816227862 · doi ↗ · pubmed ↗
- 7Cricoid palpability as a selection criterion for bedside tracheostomy Otolaryngol Head Neck Surg Husein OF Massick DD 83984413320051636050010.1016/j.otohns.2005.08.008 · doi ↗ · pubmed ↗
- 8The role of ultrasound in percutaneous dilatational tracheostomy Australas J Ultrasound Med Rudas M 1431481520122819116010.1002/j.2205-0140.2012.tb 00197.x PMC 5024914 · doi ↗ · pubmed ↗