When Coagulase-Negative Staphylococci Mislead: Transient Metabolic Acidosis in a Healthy Toddler
Filippos Filippatos, Dimitra-Ifigeneia Matara, Vasiliki Karava, Konstantinos Kakleas, Athanasios Michos

TL;DR
A healthy toddler developed temporary metabolic acidosis linked to a rare Staphylococcus hominis blood culture, highlighting the need for careful diagnosis to avoid unnecessary antibiotics.
Contribution
This case highlights the diagnostic challenge of coagulase-negative staphylococci in pediatric patients with transient metabolic acidosis.
Findings
A previously healthy toddler presented with transient metabolic acidosis and S. hominis bacteremia.
Clinical improvement occurred with supportive care, suggesting non-infectious causes for acidosis.
True S. hominis infections are rare in immunocompetent children and often linked to severe conditions.
Abstract
Staphylococcus hominis (S. hominis), a coagulase-negative staphylococcus (CoNS), is commonly encountered in blood cultures and presents diagnostic challenges in both pediatric and adult infections. Its clinical significance remains uncertain, especially in previously healthy children without evident immunodeficiency or indwelling devices. Metabolic acidosis associated with S. hominis bacteremia is rarely reported, further complicating clinical interpretation. We report a previously healthy two-year-old boy presenting with high-grade fever, cough, mild respiratory distress, and metabolic acidosis (pH 7.28, bicarbonate 12 mmol/L). Initial blood culture yielded S. hominis, while subsequent cultures remained negative. The patient had no immunodeficiency or indwelling devices. Clinical improvement occurred rapidly with supportive care, inhaled bronchodilators, intravenous fluids,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
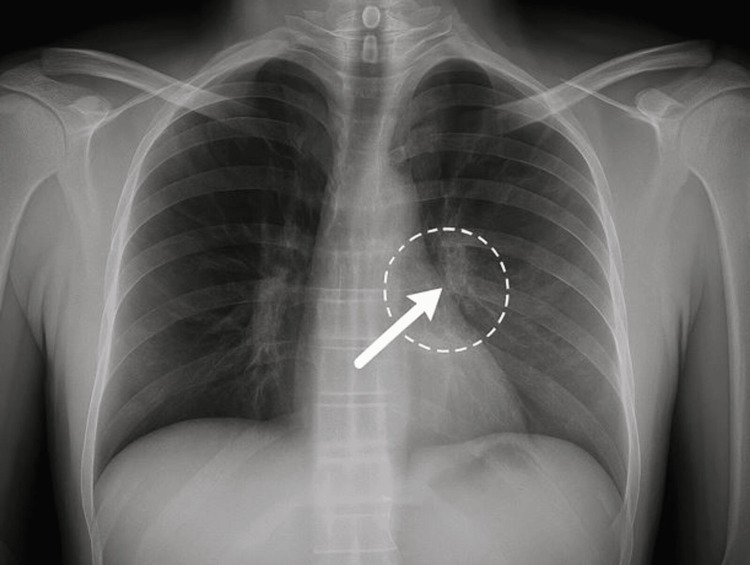 Figure 1
Figure 1| Parameter | Admission Value | Discharge Value | Reference Range | Units |
| Arterial Blood Gas | ||||
| pH | 7.28 | 7.4 | 7.35–7.45 | |
| pCO₂ | 26 | 23.2 | 35–45 | mmHg |
| HCO₃⁻ | 12 | 14.6 | 22–28 | mmol/L |
| Lactate | 1.4 | 2.2 | <2.2 | mmol/L |
| Base Excess | –9.6 | –7.9 | –2 to +2 | mmol/L |
| Inflammatory Markers | ||||
| CRP | 3.25 | <1.0 | <5.0 | mg/L |
| Procalcitonin | 1.2 | 0.12 | <0.5 | ng/mL |
| Complete Blood Count | ||||
| WBC | 7.55 | 6.8 | 5.0–14.5 | x10³/μL |
| Neutrophils % | 36.6 | 32 | 25–55 | % |
| Lymphocytes % | 47.8 | 48 | 35–65 | % |
| Monocytes % | 8.6 | 9 | 2–10 | % |
| Hemoglobin | 12 | 12.2 | 11.0–13.5 | g/dL |
| Platelets | 265 | 260 | 150–450 | x10³/μL |
| Biochemistry | ||||
| Glucose | 76 | 82 | 70–100 | mg/dL |
| Urea | 11 | 15 | 10–35 | mg/dL |
| Creatinine | 0.28 | 0.3 | 0.20–1.00 | mg/dL |
| SGOT | 46 | 35 | 10–60 | U/L |
| SGPT | 7 | 10 | 5–45 | U/L |
| γ-GT | 6 | 7 | 5–32 | U/L |
| ALP | 208 | 190 | 60–240 | U/L |
| Total Bilirubin | 0.25 | 0.2 | <1.00 | mg/dL |
| Albumin | 4.8 | 4.9 | 3.7–5.5 | g/dL |
| LDH | 407 | 340 | 120–300 | U/L |
| Magnesium | 2 | 2.1 | 1.5–2.3 | mg/dL |
| Potassium | 4.1 | 4.2 | 3.5–5.5 | mmol/L |
| Sodium | 137 | 138 | 135–150 | mmol/L |
| Chloride | 103 | 104 | 95–110 | mmol/L |
| Calcium | 10.5 | 10.6 | 8.2–11.0 | mg/dL |
| Urinalysis | ||||
| pH | 5.5 | 6 | 5.0–7.5 | |
| Specific gravity | 1026 | 1018 | 1005–1030 | |
| Protein | Negative | Negative | Negative | |
| Glucose | Positive | Negative | Negative | |
| Ketones | +++ | Negative | Negative | |
| Blood | Positive | Negative | Negative | |
| WBC (urine, per hpf) | 1–2 | 0–1 | 0–5 | /hpf |
| RBC (urine, per hpf) | 2–3 | 0–1 | 0–5 | /hpf |
| Nitrites | Negative | Negative | Negative | |
| Bacteria | Few Gram (+) | None | None | |
| Antibiotic | Interpretation | MIC (mg/L) |
| Penicillin | Resistant | ≥0.5 |
| Oxacillin (Methicillin) | Sensitive | ≤0.25 |
| Vancomycin | Sensitive | ≤1.0 |
| Teicoplanin | Sensitive | ≤2.0 |
| Linezolid | Sensitive | ≤2.0 |
| Daptomycin | Sensitive | ≤1.0 |
| Gentamicin | Sensitive | ≤1.0 |
| Ciprofloxacin | Sensitive | ≤0.5 |
| Clindamycin | Sensitive | ≤0.25 |
| Erythromycin | Resistant | ≥8.0 |
| Trimethoprim/Sulfamethoxazole | Sensitive | ≤2/38 |
| Rifampicin | Sensitive | ≤0.5 |
| Fusidic acid | Sensitive | ≤1.0 |
| Moxifloxacin | Sensitive | ≤0.25 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntimicrobial Resistance in Staphylococcus · Neonatal and Maternal Infections · Streptococcal Infections and Treatments
Introduction
Coagulase-negative staphylococci (CoNS), such as Staphylococcus hominis (S. hominis), are among the most common skin commensals and represent the leading cause of blood culture contamination in both adult and pediatric clinical practice [1,2]. In hospitalized children, mainly five days post-admission, CoNS bacteremia accounts for up to 40% of positive blood cultures, but distinguishing contamination from true infection remains a clinical challenge [2]. While S. epidermidis and S. saprophyticus are more frequently pathogenic, S. hominis has occasionally been implicated in invasive infections, mainly in immunocompromised hosts or those with indwelling devices [3,4].
Metabolic acidosis is an uncommon but potentially serious presentation in pediatric infections. It is most often linked to dehydration, catabolism, or sepsis but rarely to CoNS bacteremia [5]. The association of S. hominis with metabolic acidosis in otherwise healthy children is rarely described.
Here, we present a case of a young child with metabolic acidosis and a single S. hominis-positive blood culture and review the available literature to contextualize this finding and optimize the approach to diagnosis and management. This study was conducted in accordance with the Declaration of Helsinki. Institutional review board approval was not required for this single case report at our institution. Written informed consent was obtained from the patient’s parents for publication of this case report and any accompanying images.
Case presentation
A previously healthy two-year-old boy was admitted to the pediatric department of a tertiary hospital with a 36-hour history of high-grade fever, peaking at 39°C, associated with a persistent cough without expectoration and mild respiratory distress. The child’s parents reported a significant reduction in oral intake over the preceding three days and noted a single episode of non-bloody, non-mucoid diarrhea. There was no known exposure to sick contacts, no recent travel, and no significant family or perinatal history of diseases/conditions.
On initial examination, the child was alert and in a generally good condition. His weight was 10.9 kilograms, with a body temperature of 36.9°C (antipyretic was administered at admission to the Emergency Department), oxygen saturation of 98% on room air, heart rate of 126 beats per minute, and blood pressure measured at 104/77 mmHg (diastolic blood pressure: 95th percentile). Physical examination revealed mild periorbital hyperemia, erythematous tonsils, and mildly increased work of breathing characterized by expiratory wheeze and inspiratory crackles localized to the left upper lung field. Noted dehydration signs included reduced skin turgor, dry mucous membranes, and prolonged capillary refill time (3.5 sec). There was no evidence of lymphadenopathy or hepatosplenomegaly, and no other clinical dehydration signs were noted. The chest radiograph demonstrated a subtle interstitial infiltrate in the left upper lobe, consistent with mild lower respiratory tract involvement. No evidence of consolidation, pleural effusion, or significant hyperinflation was noted (Figure 1).
Chest radiograph demonstrating a subtle interstitial infiltrate in the left upper lobe (LUL), consistent with mild lower respiratory tract involvement. The arrow and dashed circle indicate a subtle interstitial infiltrate in the LUL. There was no evidence of consolidation, pleural effusion, or significant hyperinflation.
Laboratory investigations on admission showed a metabolic acidosis, with a blood gas revealing a pH of 7.28, pCO₂ of 26 mmHg, bicarbonate of 12 mmol/L, and lactate of 1.4 mmol/L. The complete blood count showed mild leukocytosis (WBC: 7.55x10³/μL) with a predominance of lymphocytes (47.8%), normal hemoglobin (12.0 g/dl) and platelet counts (265x10³/μL), and no features of hemolysis. C-reactive protein (CRP) and procalcitonin were mildly elevated at 3.25 mg/L (normal values: <5 mg/L) and 1.2 ng/mL (normal values: <0.5 ng/mL), respectively. Streptococcus pyogenes tonsilar infection was ruled out (rapid strep test and pharyngeal cultures were negative). Urinalysis was remarkable for glycosuria and significant ketonuria (+++), along with mild microscopic hematuria; urine culture was negative. The respiratory viral antigen panel was negative for respiratory syncytial virus, influenza, and adenovirus. Detailed laboratory findings at admission and discharge are summarized in Table 1.
On the day of admission (hour 0), one aerobic blood culture was obtained, which yielded Staphylococcus hominis after incubation. Two subsequent blood cultures were collected at +24 hours and +48 hours post-admission, both of which showed no growth. Antibiogram with minimum inhibitory concentration (MIC) values is presented in Table 2.
The patient received intravenous cefotaxime (150 mg/kg/day in three divided doses) and clindamycin (40 mg/kg/day in four divided doses), intravenous fluids, inhaled bronchodilators, and a three-day course of intravenous corticosteroids (methylprednisolone 1 mg/kg/day) for presumed lower respiratory tract infection. Cefotaxime was initially administered as empiric antibiotic coverage until blood cultures and antibiogram results were obtained. Within 48 hours, fever and metabolic acidosis resolved, and laboratory parameters normalized. Given the absence of persistent symptoms and negative follow-up cultures, the S. hominis isolate was deemed a contaminant after infectious diseases consultation. Antibiotics were de-escalated to oral amoxicillin/clavulanic acid (50 mg/kg/day of amoxicillin component in two divided doses). The patient received intravenous cefotaxime and clindamycin for two days, followed by oral amoxicillin/clavulanic acid, completing a total antibiotic course of seven days. The patient was discharged on day four in excellent condition with full clinical and laboratory recovery.
Discussion
S. hominis is commonly encountered in blood cultures and presents diagnostic challenges in both pediatric and adult infections. However, distinguishing contamination from true bacteremia remains a challenge, as CoNS may act as opportunistic pathogens in neonates, immunocompromised patients, or those with indwelling devices [1-4]. True infection in immunocompetent children is extremely rare and often debated. Our patient presented with persistent metabolic acidosis during a febrile lower respiratory tract infection, but with stable hemodynamics and no organ dysfunction or ongoing bacteremia, highlighting this diagnostic dilemma.
In this case, metabolic acidosis, characterized by low bicarbonate, mild lactate elevation, and ketonuria, likely resulted from mild dehydration and catabolic stress, rather than infection-related hypoperfusion, as there was no evidence of shock or renal compromise [5]. In the literature, metabolic acidosis in S. hominis bacteremia occurs as a non-specific feature of severe sepsis or multi-organ failure, not as a direct bacterial effect [6,7]. Reported pediatric cases nearly always involve significant risk factors [8-10]. Our case is unique in describing a healthy child with only transient acidosis and no signs of severe infection, underlining the rarity of true S. hominis bacteremia in this group.
When S. hominis was isolated from a single blood culture, a comprehensive assessment was triggered. CoNS are the most common cause of false-positive blood cultures in children, with contamination rates up to 40% [2,5,10,11]. Criteria that favor true infection include multiple positive cultures, persistent fever, signs of sepsis, or host risk factors [2,4,10]. In our case, only the initial culture was positive, symptoms quickly resolved, and there were no risk factors, supporting the diagnosis of contamination and justifying antibiotic de-escalation.
True S. hominis bacteremia has been reported, primarily in neonates with central lines, oncology patients, or those with severe comorbidities, and is rare [4,8-10]. These cases often involve persistent bacteremia and systemic inflammation, and metabolic acidosis arises mainly in the context of severe sepsis. By contrast, our patient had no such risk factors and recovered rapidly with supportive care.
CoNS, including S. hominis, can trigger host immune responses via recognition of their cell wall components (peptidoglycan, lipoteichoic acids) by Toll-like receptor 2, leading to the release of cytokines such as interleukin-1β, tumor necrosis factor-α, and interleukin-6 [11,12]. In genuine infections, this immune activation can contribute to systemic inflammation, endothelial dysfunction, and alterations in tissue perfusion, all of which may result in metabolic derangements including lactic acidosis. However, S. hominis is considered less virulent than S. aureus and possesses limited exotoxin production and reduced capacity for rapid tissue invasion [6,7]. Chronic or biofilm-associated infections by CoNS, while significant in specific populations, were not relevant to our patient, who lacked risk factors and responded rapidly to supportive management.
Clinically, this case illustrates the importance of careful interpretation of single CoNS-positive cultures in otherwise healthy pediatric and adult patients. Overuse of antibiotics can be avoided by integrating clinical findings, repeat cultures, and risk assessment. Common causes of metabolic acidosis in children, such as dehydration and increased catabolism, should be prioritized in differential diagnosis, and multidisciplinary input is valuable when ambiguity remains.
Conclusions
The case highlights the diagnostic and therapeutic challenges posed by the isolation of S. hominis in blood cultures from pediatric patients with metabolic acidosis. In immunocompetent children, a single S. hominis-positive blood culture in the absence of risk factors, persistent symptoms, or positive repeat cultures should raise strong suspicion of contamination rather than true bacteremia. Nonetheless, the temporal association with metabolic acidosis in our case underscores the diagnostic challenges posed by CoNS in pediatrics. Careful interpretation and clinical correlation are essential to avoid both overtreatment and missed diagnoses. Further studies are warranted to better define the clinical significance and metabolic impact of CoNS in otherwise healthy children.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Coagulase-negative staphylococci Clin Microbiol Rev Becker K Heilmann C Peters G 8709262720142527857710.1128/CMR.00109-13PMC 4187637 · doi ↗ · pubmed ↗
- 2Value of time to positivity of blood culture in children with bloodstream infections Can J Infect Dis Med Microbiol Pan F Zhao W Zhang H 5975837201920193073384610.1155/2019/5975837 PMC 6348829 · doi ↗ · pubmed ↗
- 3Are coagulase-negative staphylococci virulent?Clin Microbiol Infect Heilmann C Ziebuhr W Becker K 107110802520193050248710.1016/j.cmi.2018.11.012 · doi ↗ · pubmed ↗
- 4Bloodstream infections in pediatric hematology/oncology patients: six years’ experience of a single center in Turkey Turk J Med Sci Tural Kara T Erat T Yahşi A 115711644920193134273410.3906/sag-1812-101PMC 7018311 · doi ↗ · pubmed ↗
- 5Time-to-positivity of blood cultures in children with sepsis Front Pediatr Dierig A Berger C Agyeman PK 222620183013585910.3389/fped.2018.00222 PMC 6092514 · doi ↗ · pubmed ↗
- 6Quorum-sensing regulation in staphylococci-an overview Front Microbiol Le KY Otto M 1174620152657908410.3389/fmicb.2015.01174 PMC 4621875 · doi ↗ · pubmed ↗
- 7Coagulase-negative staphylococci (Co NS) as a significant etiological factor of laryngological infections: a review Ann Clin Microbiol Antimicrob Michalik M Samet A Podbielska-Kubera A Savini V Międzobrodzki J Kosecka-Strojek M 261920203249871110.1186/s 12941-020-00367-x PMC 7271473 · doi ↗ · pubmed ↗
- 8Epidemiology and pathogenesis of Staphylococcus bloodstream infections in humans: a review Pol J Microbiol Lisowska-Łysiak K Lauterbach R Międzobrodzki J Kosecka-Strojek M 13237020213381552310.33073/pjm-2021-005PMC 8330453 · doi ↗ · pubmed ↗